
Abstract
Background
The effects of an increased risk of sampling error and the lower prevalence of Helicobacter pylori infection on the diagnostic accuracy of standard invasive tests needs to be considered. Despite evidence of enhanced yield with additional biopsies, combined Rapid Urease Tests (RUTs) have not been widely adopted. We aimed to compare the diagnostic efficacy of a combined antral and corpus rapid urease test (RUT) to a single antral RUT in a low prevalence cohort.
Methods
Between August 2013 and April 2014 adult patients undergoing a scheduled gastroscopy were prospectively recruited. At endoscopy biopsies were taken and processed for single and combined RUTs, histology and culture using standard techniques. Infection was defined by positive culture or detection of Helicobacter like organisms on either antral or corpus samples.
Results
In all 123 patients were recruited. H. pylori prevalence was low at 36%, n = 44. There was a significant difference in positivity between single and combined RUTs, 20% (n = 25) versus 30% (n = 37), p = 0.0094, (95% CI 0.15–0.04). The number needed to treat (NNT) for an additional diagnosis of infection using a combined versus a single RUT is 4 (95% CI 2.2–11). The only factor associated with a reduction in RUT yield was regular proton pump inhibitor (PPI) use. Overall the sensitivity, specificity, positive and negative predictive value for any RUT test was 84%, 100%, 100% and 92% respectively.
Conclusion
Our data suggests taking routine antral and corpus biopsies in conjunction with a combined RUT appears to optimizing H. pylori detection and overcome sampling error in a low prevalence population.
Keywords
Introduction
The diagnosis and treatment of Helicobacter pylori infection is a key element of appropriate management of a variety of conditions; peptic ulceration, gastritis, non-ulcer dyspepsia and of gastric cancer prevention. For most dyspeptic subjects without alarm symptoms, identification of infection by non-invasive means is the corner stone of management.1,2 With endoscopy now reserved for older patients, those at higher risk of premalignant or malignant disease and those with failed first line therapy for gastro-oesophageal reflux disease or H. pylori infection. As such the profile of patients undergoing endoscopy including invasive tests for H. pylori has changed, including older age, previous treatment with a proton pump inhibitor and prior empirical eradication therapy. All of which can impact on the accuracy of diagnostic tests.3–5 Similarly, it is well documented that H. pylori prevalence rates are falling in the developed world.6–11 The prevalence of a condition affects test performance for given sensitivity and specificity values. To optimize test performance, disease prevalence should be incorporated in testing decisions, and sensitivity and specificity should be set locally, not globally. 12 As such, the dual effects of reduced sensitivity due to the cohort of patients selected for endoscopy, and the low prevalence rates of infection on the diagnostic accuracy of standard invasive tests needs to be considered and optimal testing strategies developed.
Of available invasive tests for H.pylori; Rapid Urease Test (RUT), histology and culture, a single antral RUT, the ‘Campylobacter like organism (CLO) and go’ remains popular. 13 With extensive biopsy protocols such as the updated Sydney classification and OLGA system rarely used in the clinical setting.14,15 RUTs are perceived to be reliable, relatively cheap and quick to perform and can provide a result before patients are discharged from the day ward. However, false negatives, particularly as a result of sampling errors, do occur, and several studies have reported increased RUT sensitivities with the use of additional biopsies from different gastric sites.16–18 More recently the use of a combined antral and corpus RUT has been shown to have superior sensitivity and more rapid reading times to single RUTs. 19 Despite this evidence, combined RUT biopsy protocols have not as yet been widely adopted. While a combined, dual biopsy approach is likely to offer even more advantage in low prevalence countries, its value in this clinical setting remains to be established. We aimed to prospectively compare the diagnostic efficacy of a combined antral and corpus RUT to a single antral RUT in a low prevalence cohort using antral and corpus histology with modified Giemsa staining as our goal standard.
Materials and methods
Population
Between August 2013 and April 2014 adult patients undergoing a scheduled gastroscopy at Tallaght Hospital, Dublin, Ireland were prospectively recruited to the study. Patients with previous upper gastrointestinal surgery, previous H. pylori eradication treatment, bismuth salts or antibiotics in the preceding 4 weeks or any contraindication to biopsy were excluded. Informed consent was taken from all subjects prior to study inclusion. Patient demographics, endoscopy findings, adverse events and proton pump inhibitor (PPI) use were recorded.
Methods
Endoscopy was performed as standard. During endoscopy a single biopsy was taken from the antrum and placed in a CLO (Campylobacter like Organism, Ballard Medical, Draper) test. A further single biopsy from both the antrum and corpus were taken and placed together in another CLO test, referred to subsequently as a combined RUT. An additional two biopsies each were taken from the antrum and corpus for histological examination. Biopsies were taken with a standard forceps (requires 2.8 mm biopsy channel). Histological examination was done in the pathology core lab, and the gastric specimens were fixed with formalin, embedded in paraffin and stained with Giemsa. Biopsies obtained for the CLO test were taken before those used for histological examination to avoid contamination with formalin. The Consultant pathologist performing histological examination did not have access to the RUT results. Immunochemistry was used in case of discrepancy between RUT and histology results. Culture of H. pylori was carried out on antral samples which were placed in DENT broth. In brief, samples were rubbed on the surface of a Campy-BAP agar plate (Brucella agar (Difco) + IsoVitalex (Gibco)+ 10% whole sheep blood), and then incubated at 35℃ under micro aerobic conditions (5% O2, 10% CO2, and 85% N2) for 4–5 days. H.pylori culture was considered as positive if one or more colonies of gram-negative, oxidase (+), catalase (+) and urease (+) spiral or curved rods were present. CLO tests were stored at room temperature and examined and interpreted at 30 minutes in accordance with manufacturer‘s guidelines by an independent observer in the endoscopy unit. H. pylori infection was defined by either positive histology or culture. Urea breath test (UBT) was performed after treatment of H.pylori, guided by culture sensitivities (if available) or as per protocol where sensitivities were not available to confirm eradication.
Analysis
The positivity rates for single antral and dual antral and corpus CLO tests were compared using a Fisher’s exact test. A p value of <0.05 was considered significant. The positive and negative predictive values for RUT were assessed by comparison with histological and culture data. The effect of diagnosis and PPI use and patient demographics on outcome were assessed by multivariate analysis.
Results
Characteristics of the study population
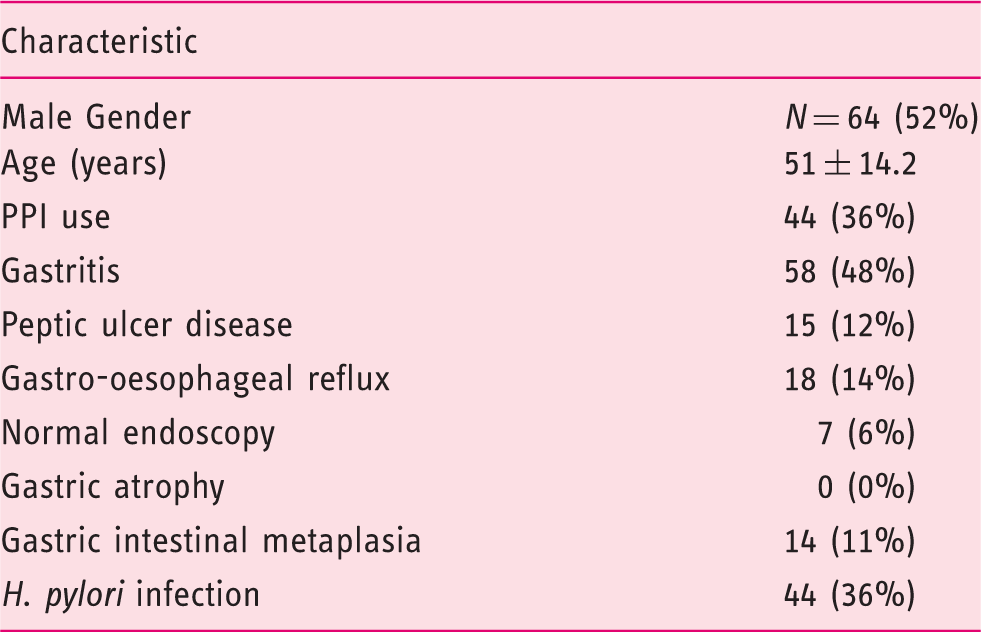
RUT results
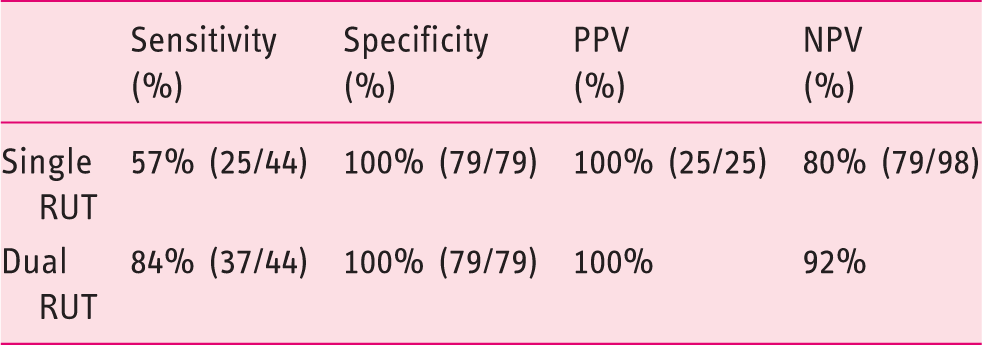
Of the 44 H. pylori infected subjects, 37 (84%) had a positive RUT. Overall the sensitivity, specificity, positive and negative predictive value for any RUT test was 84%, 100%, 100% and 92% respectively. In all there were 7(16%) false negative RUT tests.
Accuracy of single and combined rapid urease tests compared to antral and corpus histological assessment with modified Giemsa staining and culture
In all, 11 patients (25%) patients with H. pylori infection were on a PPI prior to endoscopy compared to 42% (n = 33) without infection, this difference did not reach statistical significance, p = 0.078, (95% CI 0.01–0.35). On univariate analysis the only factor associated with a reduction in RUT yield was regular PPI use. PPI use was associated with a great risk of false negative RUTs, 9 of 19 subjects with a false negative single RUT versus 2 of 25 with true positive RUTs were on a PPI, OR 10, p < 0.007, (95% CI 1.88–56.8) (Figure 1).
Rates of PPI use in true positive and false negative single antral RUT according to prior PPI exposure.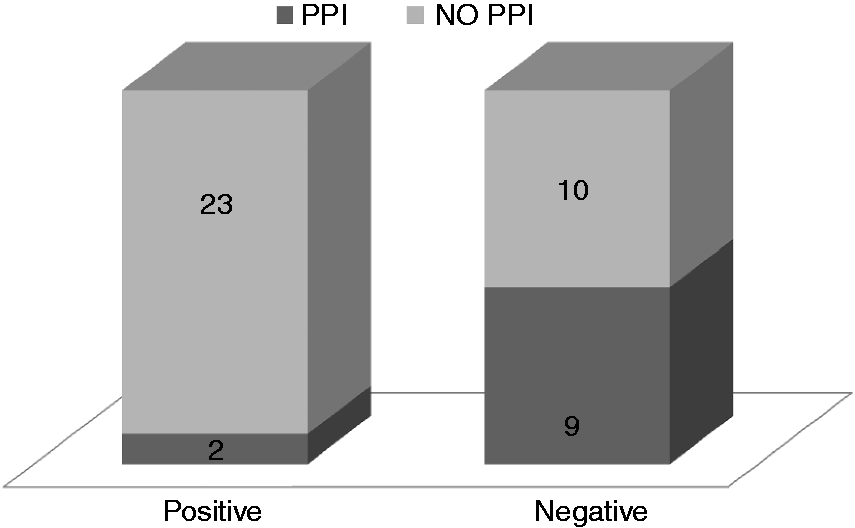
Discussion
The accurate diagnosis of H. pylori infection is a key objective in the management of patients with a variety of gastro-duodenal symptoms and pathology undergoing endoscopy. With a reduced prevalence of infection in the developed world, the routine selection of older subjects for endoscopy and the widespread use of PPIs, all of which increase the risk of sampling error, there is a need to tailor standard biopsy protocols to optimize the diagnostic yield of routine tests. RUTs remain a frequently employed test in this clinical setting and previous publications have shown the diagnostic yield of RUTs are enhanced when multiple biopsies are tested. Including two or more samples from the same site, either in separate RUT chambers or combined in a single chamber or sampling from the corpus and antrum can increase sensitivity and the speed of a positive test.16–18 The increasing yield from additional sampling has also been shown to be more effective post eradication, albeit in a small cohort of 59 subjects in whom only 16% remained positive after treatment. 5 More recently in 2010, Hsu et al. performed a study comparing several different RUTs in treatment naïve and post eradication subjects and included a proportion of dual antral and corpus tests. 13 In all 35% of their treatment naïve and 22% of their post eradication cohort were H. pylori positive. Of interest while the time to a positive test was shorter in the dual antral and corpus group overall, there was a statistically enhanced yield for dual testing compared to single antral testing in the post eradication group only.
To reduce cost and time and optimize yield, including the speed of a positive result the use of a combined, antral and corpus biopsy in a single RUT chamber has been proposed. In 2012, Moon et al. reported an additional yield for a combined RUT approach (69%) compared to both single antral and corpus testing, 59% versus 62%, respectively, in 214 treatment naïve subjects. 19 Although the study designs are similar comparisons are difficult to make as H. pylori infection was very common in their population, 69% versus 35% in ours. As previously discussed low background prevalence will negatively impact on test accuracy. In addition only 52% of cases in the Moon et al. paper were confirmed on histological analysis without recourse to specific H. pylori stains, 19 unlike our study where a modified Giemsa stain was employed and all positive RUTs were confirmed histologically. Of interest also, a significant percentage of the population were reported to have gastric atrophy (79%), which would affect antral based tests and could represent a source of bias in favour of combined testing. Intestinal metaplasia and atrophy were infrequent findings in our cohort 11% (n = 14) and 0% (n = 0), respectively. The different rates of IM and atrophy are not surprising and mirror the expected variation in gastric cancer risk among the two populations.
Our prospective study in a low prevalence cohort has confirmed a significant advantage for a combined antral and corpus RUT approach, with a NNT of four to detect an additional infected subject. The overall accuracy of RUT, however, is surprisingly poor; sensitivity 84% and 57% for combined corpus and antral and single antral RUTs, respectively. In all, just over one third of patients were taking a PPI regularly, and all were asked to discontinue medication for 10 days prior to endoscopy, which should have minimized the risk of false negative tests. However, PPI use was statistically associated with a false negative test, OR = 10, and was the only identifiable at-risk characteristic at the time of endoscopy. Whether extension of the reading time beyond 30 minutes would have increased sensitivity in this cohort remains a possibility. However delayed analysis would not be practical in a day-care environment in which there is a high turnover of patients. Nor is interpretation of RUTs at 24 hours a solution, as false positive tests become a problem at that stage. While H. pylori culture is uncommon in clinical practice, its use in screening for bacterial resistance is advisable in high risk communities such as ours, and is routinely used in our unit. The overall yield of 55% for culture in this study is disappointing, but not surprising in light of the enhanced detection of H. pylori with the addition of both corpus RUTs and histological analysis. Our culture yield could similarly be enhanced by the combination of an additional corpus biopsy with our standard antral sample, but unfortunately was not assessed in this study.
Conclusion
Our data suggests that the regular practice of taking routine antral and corpus biopsies in conjunction with a combined antral and corpus RUT appears to optimize H. pylori detection and overcome sampling error in a low prevalence population. It can be easily undertaken by the majority of endoscopists with a minimal increase in biopsy and procedure time or cost.The effect post eradication is likely to be enhanced but requires further investigation. The comparison of histology with combined RUT would also require further work.