
Abstract
Background
Helicobacter pylori infection causes long-term chronic active gastritis, a risk factor for the intestinal and diffuse forms of gastric cancer. Most gastric cancers develop in a stepwise progression from chronic active gastritis to precursor lesions of gastric cancer. The early detection of gastric cancer improves survival. Studies with recent evidence have proposed circulating-microRNAs as biomarkers of cancer.
Objective
The purpose of this study was to explore the circulating-microRNA profile from H. pylori infection to gastric adenocarcinoma.
Methods
One hundred and twenty-three patients were enrolled and assigned to the discovery or the validation sets. In the discovery phase, circulating-microRNAs were measured by dye-based quantitative polymerase chain reaction and a selection of circulating-microRNAs was validated by probe-based quantitative polymerase chain reaction. A quality control protocol was used.
Results
One hundred and sixty-seven circulating-microRNAs were detected. Precursor lesions of gastric cancer and gastric cancer patients showed the downregulation of eight and five circulating-microRNAs, respectively. We further validated the deregulation of miR-196a-5p in precursor lesions of gastric cancer and the deregulation of miR-134-5p, miR-144-3p and miR-451a in gastric cancer. However, circulating-microRNAs exhibited moderate diagnostic performance due to the overlap of circulating-microRNA expression between non-cancer and cancer patients. miR-144-3p/miR-451a expression levels were correlated. Interestingly, these microRNAs are in 17q11.2, a site of rearrangements associated with gastric cancer.
Conclusion
Circulating-microRNAs are deregulated in precancerous and gastric cancer patients but efforts are needed to improve their diagnostic accuracy.
Keywords
Key summary
Established knowledge
The invasive nature of endoscopy limits its application as screening tool for the early detection of GC in areas of intermediate prevalence. c-miRNAs have attracted attention in minimally invasive testing but there are inconsistencies in the literature regarding c-miRNA measurements. c-miRNAs had not been evaluated in Correa's cascade to GC. Using a strict QC protocol, the present study evaluated c-miRNAs in different stages of Correa's cascade to elucidate their diagnostic potential for the early detection of GC.
Significant findings
miR-196a-5p was deregulated in plasma of patients with precursor lesions of GC. miR-134-5p, miR-144-3p and miR-451a were deregulated in PLGC. miR-144-3p/miR-451a plasma levels were highly correlated. This pair is in 17q11.2, a site associated with GC. c-miRNAs lacked the specificity/sensitivity to translate to the clinic.
Introduction
Gastric cancer (GC) is one of the most common cancers. Advances in diagnostic and treatment have increased survival for early-stage GC, but prognosis for those with advanced stages remains poor. Early stages are often asymptomatic and, currently, screening endoscopy in high-risk populations is the only way to diagnose GC. Its invasive nature limits its clinical application as screening tool in areas of low-to-intermediate GC prevalence. Therefore, the development of biomarkers has become a hot research topic.1,2
Helicobacter pylori is the main aetiologic agent of GC. 3 The infection causes a sequence of events known as Correa's cascade, 3 a stepwise progression from non-active gastritis (NAG), chronic-active gastritis (CAG), precursor lesions of GC (PLGC) and GC. Circulating biomarkers would be helpful for monitoring PLGC and allow the early diagnosis of GC. In this sense, several biomarkers have been proposed but with moderate sensitivity/specificity. 4
MicroRNAs (miRNAs) regulate gene expression and its expression is altered in cancers, 5 acting as tumour suppressors or as oncogenes. 5 Circulating-miRNAs (c-miRNAs) can be found in the blood and they have attracted attention as biomarkers. 6 The discovery of c-miRNAs was first documented in a study demonstrating the existence of placental miRNAs in maternal plasma. 7 Subsequent evidence has shown that serum/plasma contain large amounts of miRNAs derived from other origins, including cancer tissues, 8 reflecting their potential as biomarkers.
Several studies have screened out hundreds of c-miRNAs in GC. 9 However, there have been inconsistencies and discrepancies regarding the accuracy/reproducibility of c-miRNA measurements; in fact, none of them yet have a clinical use as a biomarker. Furthermore, few studies had evaluated tissue miRNA deregulation according to Correa's cascade and, to our knowledge, none of them has profiled c-miRNAs in plasma.
The present study evaluated c-miRNAs at different stages of progression to GC, to help to elucidate their diagnostic potential for early detection of GC in a European country with an intermediate H. pylori prevalence (50%) and an estimated GC incidence of 7.8 per 100,000 habitants.
Materials and methods
Patients and samples
Blood was collected from patients referred to endoscopy for evaluation of dyspepsia and from patients with GC undergoing preoperative endoscopic ultrasound (EUS). The study was approved by the Ethics Committee of the Corporació Sanitària Parc Taulí (Institut Universitari Parc Taulí, Sabadell, Spain) (code: 2005511; approval date: 2006/1/11) in accordance with the Declaration of Helsinki. All subjects provided signed informed consent.
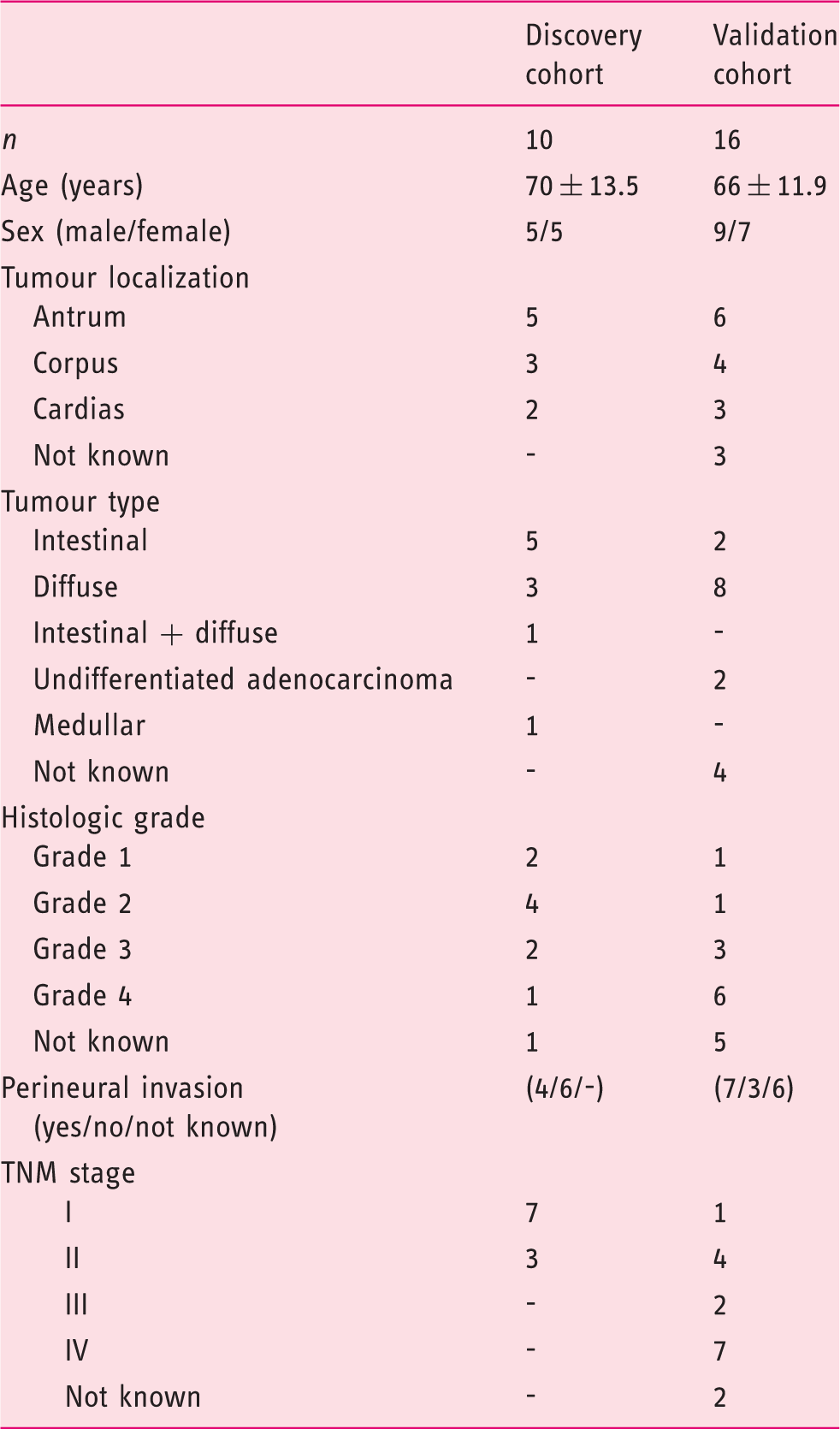
This study enrolled 123 patients classified into: Non-active gastritis and H. pylori negative (NAG; n = 31), H. pylori-infected patients with CAG (n = 35), patients with PLGC (n = 31) and GC (n = 26). GC patients were at early TNM stages I/II (in 15 cases) and in advanced (III+IV) (in nine cases); in two patients TNM could not be determined.
Patients were randomly assigned to discovery and validation sets, except for GC patients, in which patients with early stages were selected for the discovery set (Figure 1). The discovery and validation cohorts were composed of 40 and 83 independent patients, respectively. Four cases were excluded from the final analysis after quality control (QC) checking. Additional data on diagnostic tests, sample collection and RNA isolation are in the Supplementary Material.
Study diagram showing discovery and validation cohorts and the quality control steps used to determine circulating-microRNA (c-miRNA) levels.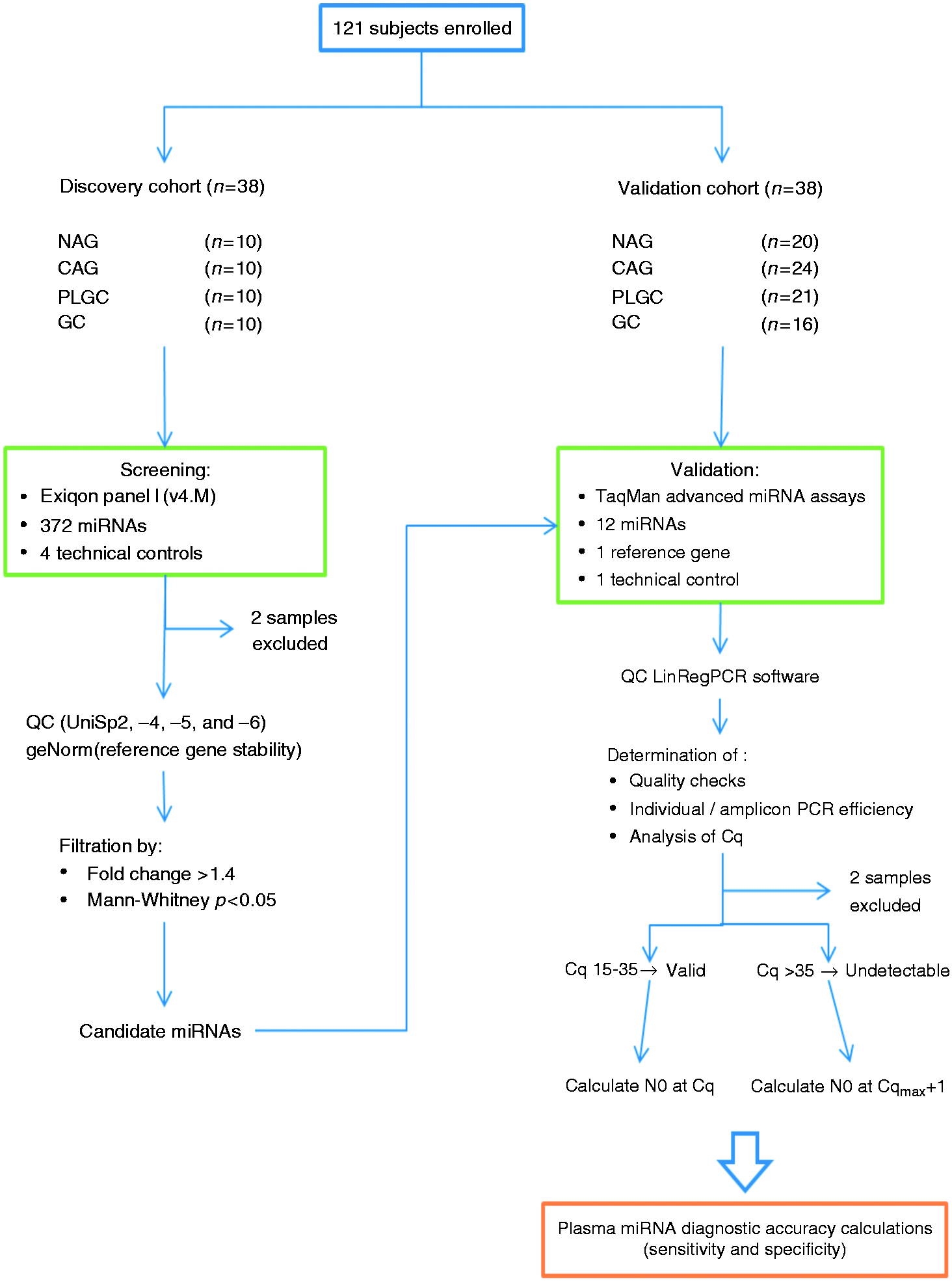
MicroRNA discovery profiling
MiRNA discovery profiling was performed using Exiqon panel I, V4.M (Exiqon, Denmark). Each plate interrogates 372 human miRNAs plus control assays. Details are in the Supplementary Material.
MicroRNA validation
The miRNA levels of 11 selected miRNAs were analysed by quantitative real-time polymerase chain reaction (qRT-PCR) using TaqMan Advanced miRNA Assays (ThermoFisher), in accordance with the manufacturer's instructions. Details about the protocol used can be found in the Supplementary Material.
Data analysis and statistics
Discovery phase
Raw qRT-PCR data from the 38 discovery 384-plates were processed using QuantStudio (ThermoFisher) and raw data imported to ExpressionSuite (ThermoFisher). For all 384 miRNAs and controls, the software calculated the thresholds across all samples. A file containing the data was exported to work in an R statistical environment. As no consensus on the use of internal normalization control is defined for plasma miRNA quantitative polymerase chain reaction (qPCR) studies, we used geNorm 10 to determine the reference miRNA in our cohort. miR-185-5p resulted in the most stable endogenous control identified by geNorm. MiRNAs that were not amplified at least in 35 of the 38 analysed samples were not considered. Significance was set at p < 0.05 with fold-changes >1.4. The Mann–Whitney U test was used without false discovery rate (FDR) correction.
Validation phase
Individual and mean polymerase chain reaction (PCR) efficiencies for amplicon, Cq and N0 values were obtained using LinRegPCR software 11 from raw data exported in RDLM language from QuantStudio. Details about LinRegPCR and subsequent analysis are in the Supplementary Material.
Results
Demographic and clinical data of dyspeptic patients.
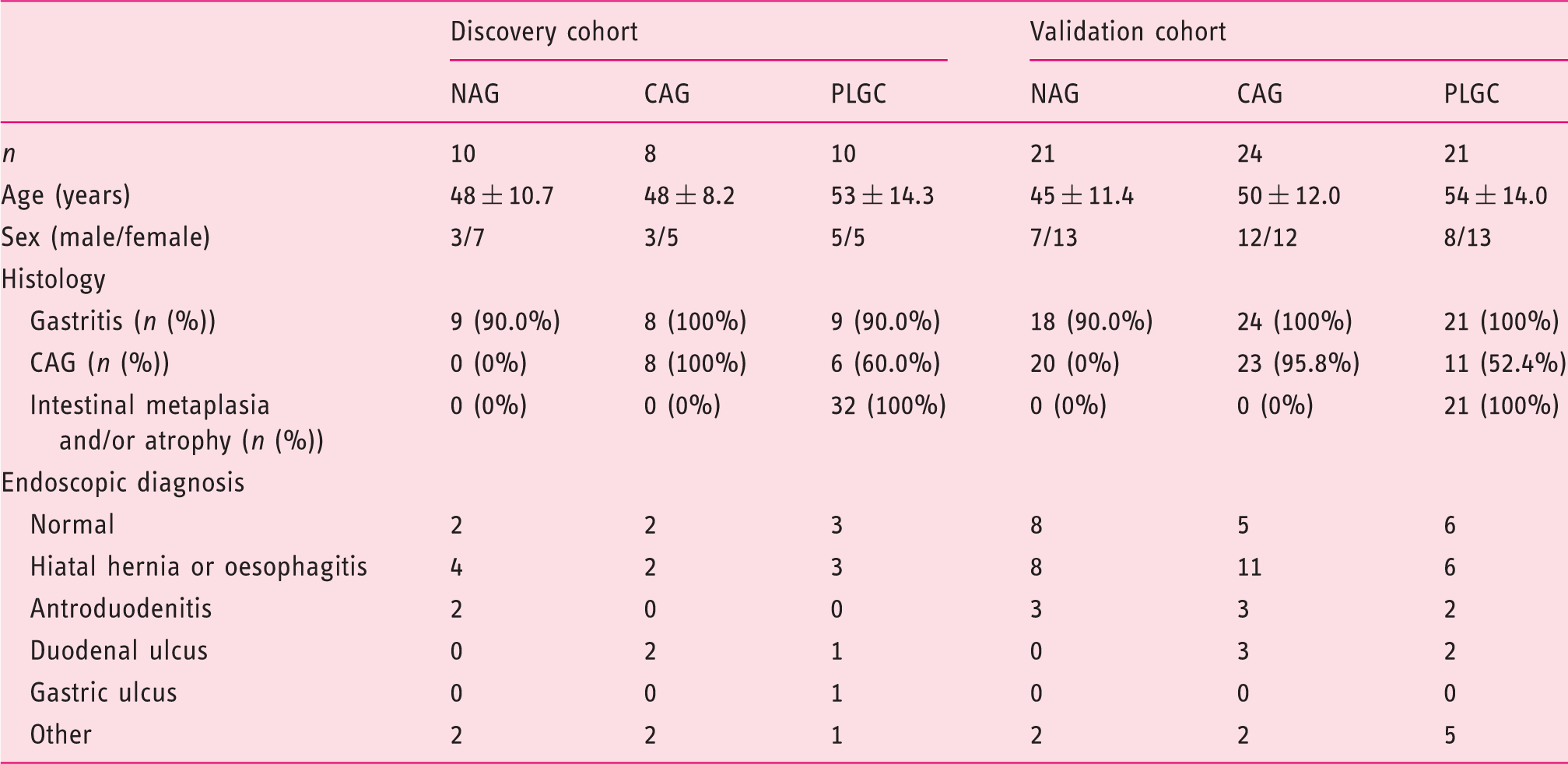
CAG: chronic active gastritis; NAG: non-active gastritis; PLGC: precursor lesions of gastric cancer.
Demographic and clinical data of gastric cancer patients.
Discovery phase
The QC protocol used indicated that the groups of patients had equivalent technical variability (Supplementary Material Results, Supplementary Material Figure 1). Differences in c-miRNA expression in the studied cohort are therefore attributable to biological variability.
In the discovery phase, real-time PCR was performed to identify differential expression patterns of miRNAs in plasma between the four patient groups (NAG, CAG, PLGC and GC). Of all 372 miRNAs included in the panel, 167 (45%) were detected in all 38 samples and 209 (56%) in more than 35. Twenty-seven miRNAs were not detected in any plasma sample (Supplementary Material Figure 2(a)). A total of 142 miRNAs (42%) were detected at mean Cq values greater than 35, which were mainly detected only in a few samples and were therefore not considered in the final analysis. In summary, 203 miRNAs (64%) were correctly quantified in the 25-35 Cq range, among which 18 (5%) had a Cq below 25 (Supplementary Material Figure 2(b)).
Fold changes of candidate circulating-microRNAs (c-miRNAs) as identified by the quantitative polymerase chain reaction (qPCR) panel in the discovery phase.
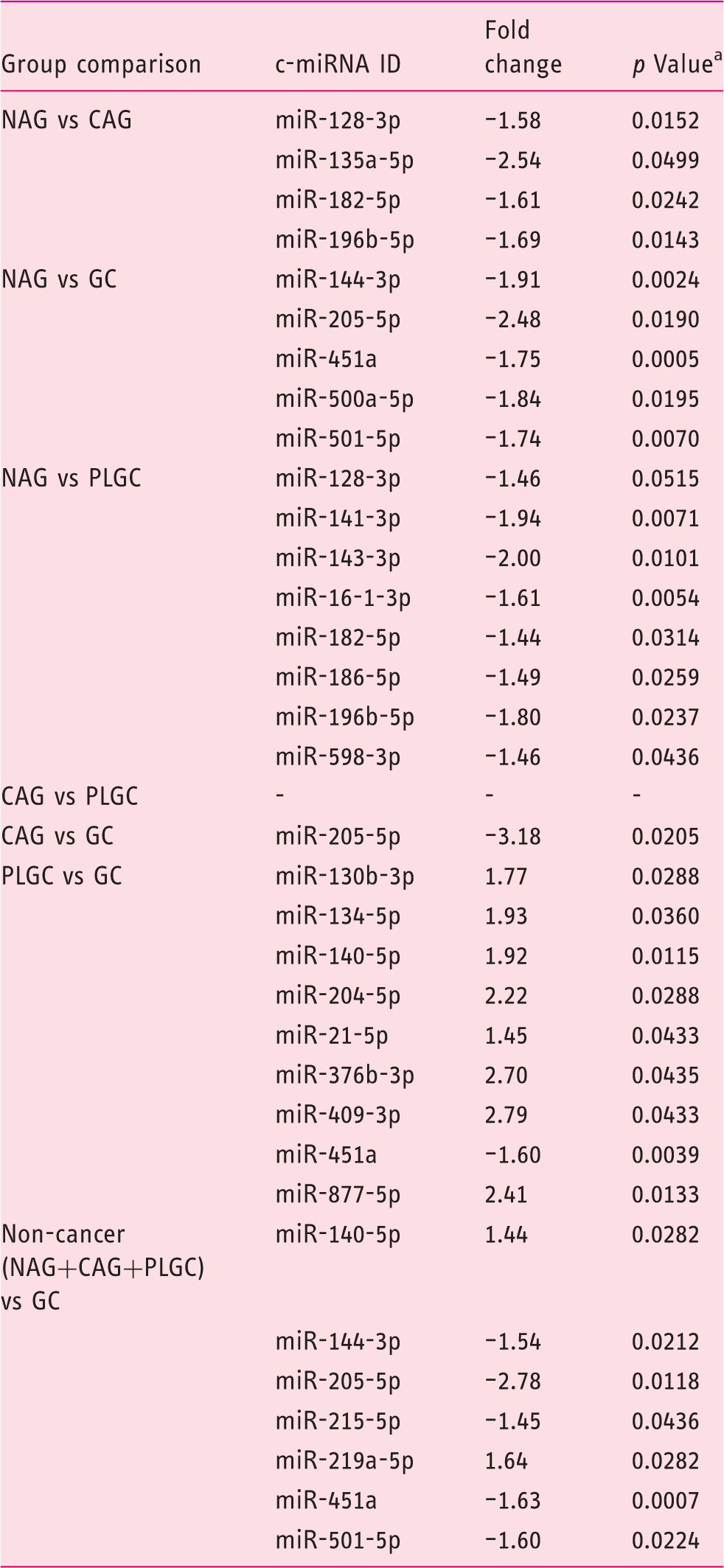
CAG: chronic active gastritis; GC: gastric cancer; NAG: non-active gastritis; PLGC: precursor lesions of gastric cancer.
Mann–Whitney U test.
Compared to NAG, CAG patients showed four down-regulated miRNAs (miR-128-3p, miR-135a-5p, miR-182-5p and miR-196b-5p). Compared to the same control group, PLGC patients showed the down-regulation of 12 miRNAs (miR-16-1-3p, miR-128-3p, miR-141-3p, miR-143-3p, miR-182-5p, miR-186-5p and miR-196b-5p). Finally, five miRNAs (miR-144-3p, miR-205-5p, miR-451a, miR-500a-5p and miR-501-5p) were down-regulated in plasma samples of GC.
The second objective was to compare the miRNA profile between PLGC and GC patients. Expression levels of six miRNAs were up-regulated (miR-130b-3p, miR-140-5p, miR-204-5p, miR-21-5p, miR-376b-3p, miR-409-3p and miR-877-5p) and one miRNA down-regulated (miR-451a).
The final objective was to obtain the c-miRNA profile of GC patients when using all non-cancer patients (NAG+CAG+PLGC) as the control group. Five miRNAs were down-regulated (miR-144-3p, miR-205-5p, miR-215-5p, miR-219a-5p, miR-451a, miR-501-5p) and two up-regulated (miR-140-5p, miR-219a-5p).
Validation phase
The 11 c-miRNAs selected for validation were: miR-134-5p, miR-141-3p, miR-144-3p, miR-182-5p, miR-196b-5p, miR-204-5p, miR-205-5p, miR-215-5p, miR-451a, miR-501-5p and miR-877-5p. Cel-miR-39 was used as an internal QC and c-miRNAs were normalised to endogenous housekeeping miR-185-5p.
miR-141-3p and miR-204-5p showed PCR efficiencies below 1.5 and were excluded from further analysis. miR-185-5p, miR-144-3p and miR-451a were the miRNAs with the lowest Cq values and better LinRegPCR quality checks and LinRegPCR sample use. miR-877-5p, miR-134-5p, miR-451a, miR-205-5p, miR-196b-5p, miR-182-5p, and miR-215-5p had baseline errors that were corrected manually (Supplementary Material Tables 3 and 4).
To validate the c-miRNAs identified using the Exiqon panel we used a separate, independent cohort of 83 patients composed of NAG (n = 21), CAG (n = 25), PLGC (n = 21) and GC patients (n = 16) (Figure 1). Two samples did not comply with the QC protocol and were excluded from the analysis.
We found that the expression levels of miR-144-3p and miR-451a were significantly down-regulated in plasma of GC patients. This was independent of whether the control group consisted of NAG patients (miR-144-3p: p = 0.046, one-way analysis of variance (ANOVA), Figure 2(a); miR-451a: p = 0.033, one-way ANOVA, Figure 2(b)) or all non-cancer patients (miR-144-3p: p = 0.033, t-Test, Figure 2(d); miR-451a: p = 0.042, t-Test, Figure 2(e)). When we used the noncancer group as the control group, a significant increase of miR-134 was also validated (miR-134-3p: p = 0.046, t-Test, Figure 2(f)). miR-196a was also down-regulated in PLGC with respect to NAG (p = 0.045, one-way ANOVA, Figure 2(c)). Five c-miRNAs (miR-182-5p, miR-205-5p, miR-215-5p, miR-501-5p and miR-877-5p) did not reach statistical significance in the validation set.
Circulating-microRNA (c-miRNA) expression validation of miR-144-3p ((a) and (d)), miR-451a ((b) and (e)), miR-196b-3p (c) and miR-134-5p (f) in key steps of Correa’s cascade ((a)–(c)) and in the pool of non-gastric cancer patients ((d)–(f)).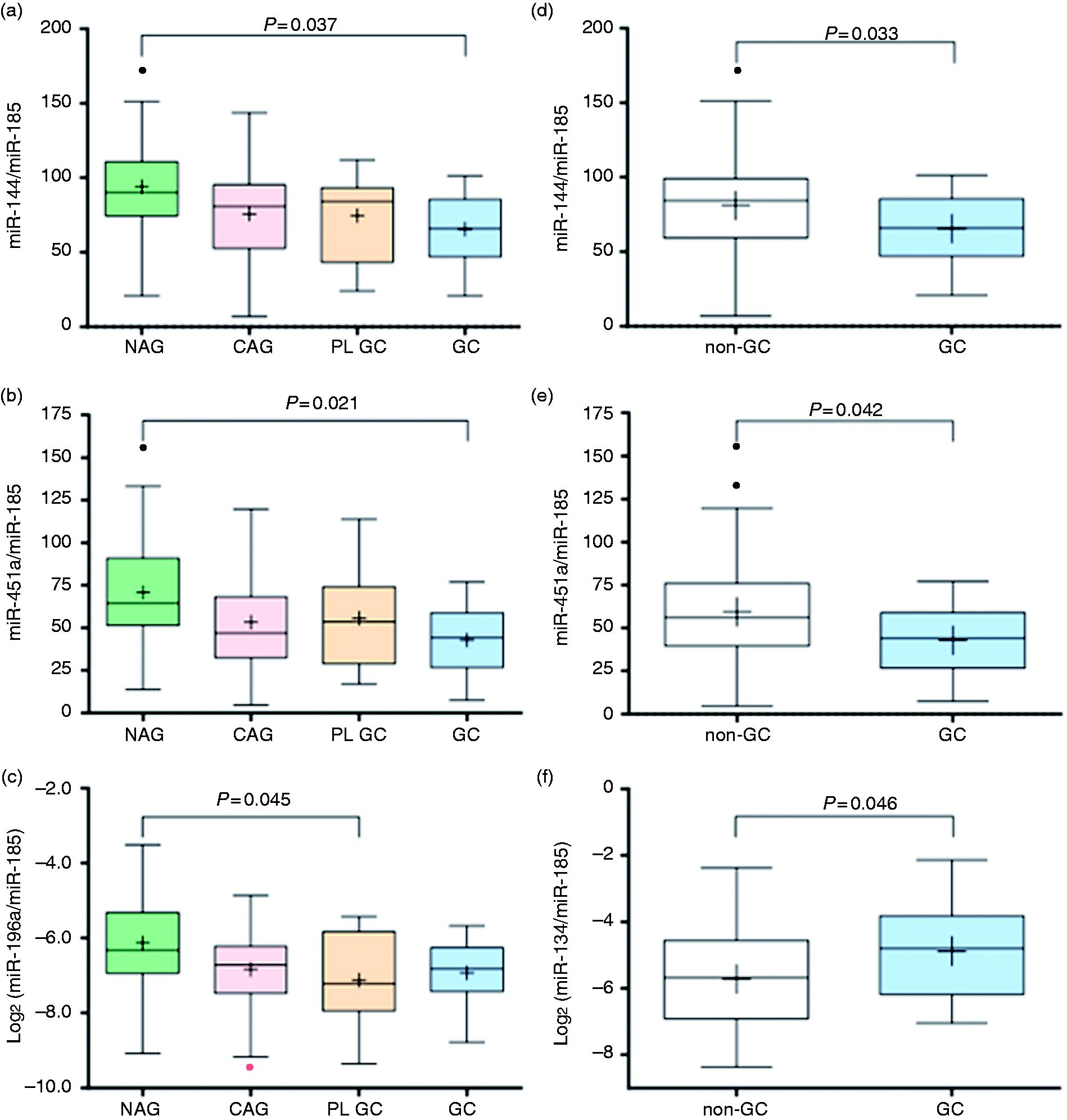
Next we evaluated the correlations in the expression of c-miRNAs. miR-144-3p and miR-451a were highly correlated.
Correlation analysis between circulating microRNAs, miR-144-3p and miR-451a.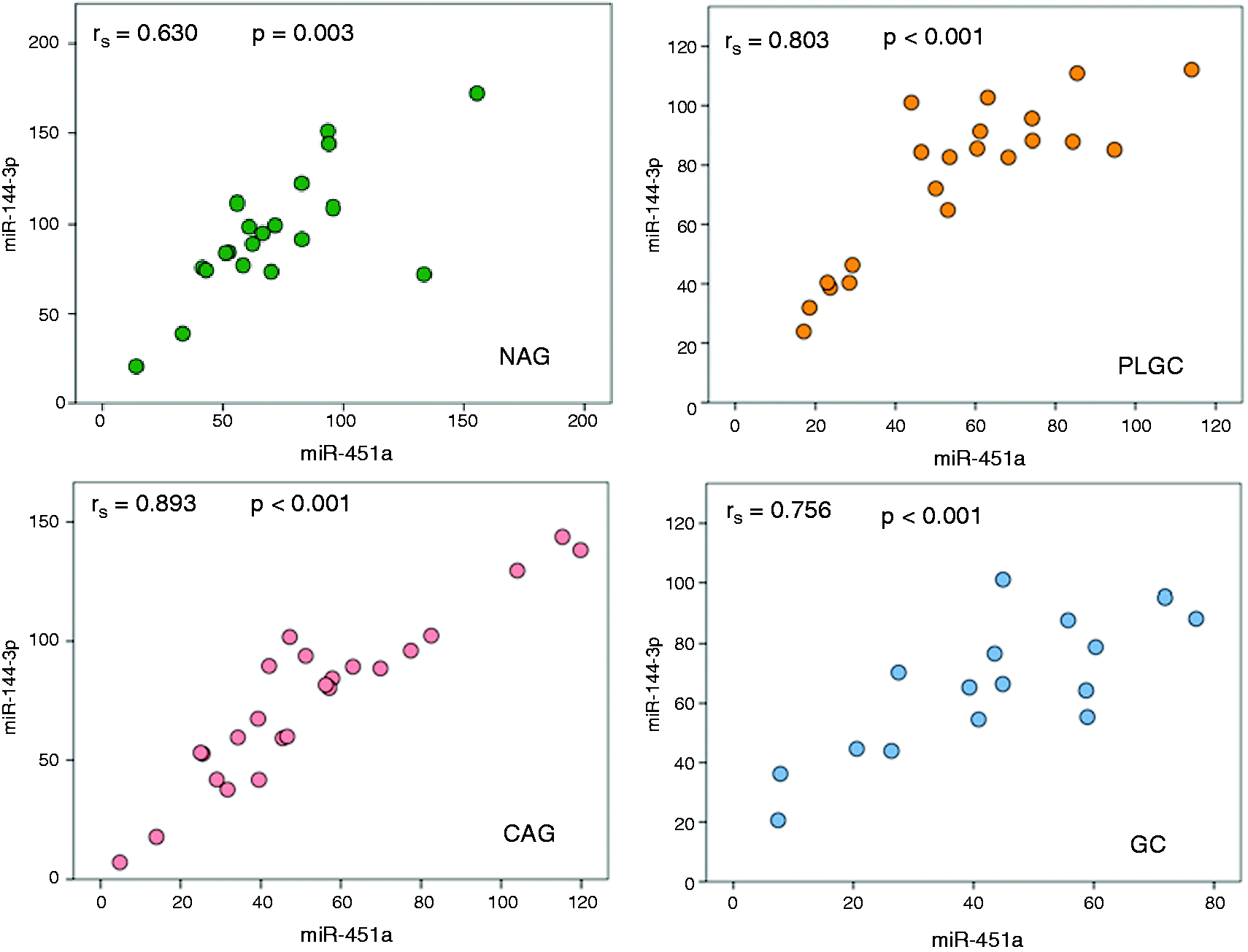
Sensitivity, specificity, positive and negative predictive values of circulating-microRNAs (c-miRNAs) for the diagnosis of gastric cancer using non-active gastritis (NAG) or non-cancer patients (NAG+chronic active gastritis (CAG)+precursor lesions of gastric cancer (PLGC)) as reference groups.
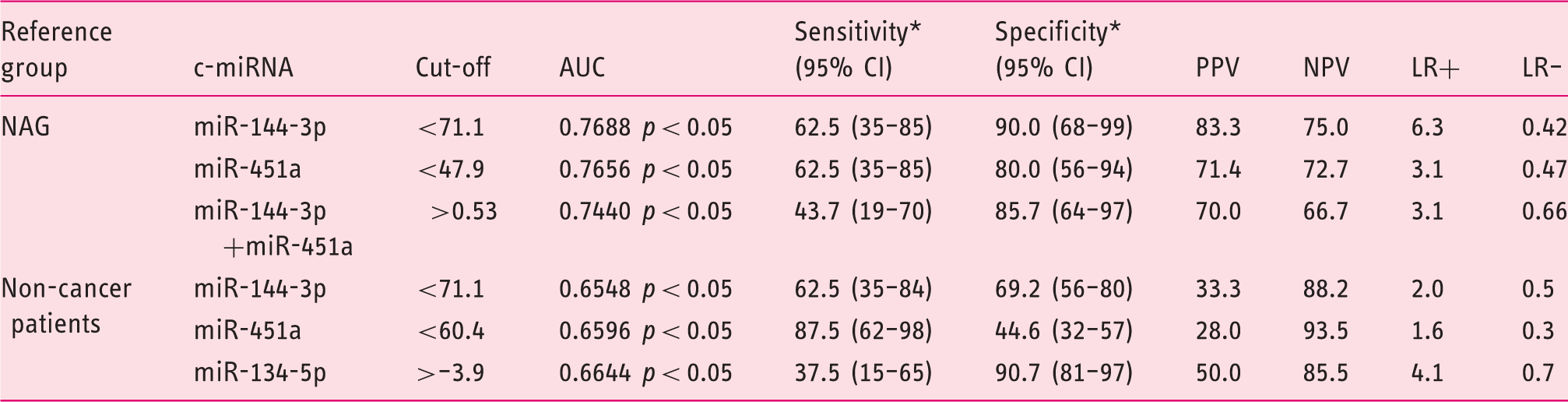
AUC: area under the curve; CI: confidence interval; LR+; positive likelihood ratio; LR–: negative likelihood ratio; NPV: negative predictive value; PPV: positive predictive value.
*Values are percentages and 95% CIs.
Discussion
Increasingly, reports indicate that circulating miRNAs have the potential to be biomarkers in patients with different diseases, including digestive cancers. 12 In the present study, we have assessed the use of c-miRNAs as potential non-invasive biomarkers for the diagnosis of patients with PLGC and GC. Two cohorts of patients with NAG, CAG, PLGC and GC were studied. Three hundred and seventy-two miRNAs were screened in the plasma of the discovery cohort by qPCR and validation was performed in an independent cohort using a different qPCR platform. Quantification was technically controlled by the addition of RNA spike-ins to key steps of c-miRNA quantification, and individual qPCR amplifications were checked for quality parameters. Using this strategy, we have found and validated that miR-196a-5p is down-regulated in PLGC, miR-134-5p is up-regulated in GC patients, and miR-144-3p and miR-451a are highly correlated and down-regulated in GC. However, the magnitude of change in expression levels was small, with overlapping expression patterns between groups, leading to low diagnostic accuracy.
Early GC diagnosis remains an important clinical problem. These patients have no obvious symptoms and dyspeptic symptoms correlate poorly with histological findings. 13 Dyspeptic symptoms can only be associated with H. pylori gastritis if successful eradication is followed by remission of symptoms. 13 CAG is a common pathological event that occurs after H. pylori infection; after years of sustained inflammation, atrophic gastritis and intestinal metaplasia may appear. A low proportion of infected individuals may finally develop GC. Gastric atrophy and intestinal metaplasia are considered as PLGC. There is no general agreement regarding whether patients with PLGC may benefit from endoscopy surveillance since the risk of progression from this step to GC is low. The risk increases when atrophy and/or metaplasia extend to the corpus. In this case, endoscopic surveillance should be offered to the patient, although it is not cost effective. 14 The evaluation of such lesions is made by extensive biopsy sampling and OLGA (Operative Link for Gastritis Assessment) / OLGIM (Operative Link on Gastric Intestinal Metaplasia Assessment) classification. 2 Non-invasive methods based on pepsinogen levels had moderate diagnostic accuracy for detecting PLGC and low accuracy for GC. 1 Our goal was to fill the gap of minimally invasive markers for surveillance from PLGC to GC by measuring c-miRNAs.
We have validated four miRNAs. Both discovery and validation cohorts showed the down-regulation of miR-144-3p and miR-451a. This pair forms a cluster in 17q11.2 and are separated from each other by 100 bp. Interestingly, this region had been reported to be involved in recurrent chromosomal rearrangements associated with GC 15 and it contains oncogenes. 16
In agreement with our results in plasma, miR-451a is down-regulated in GC tissue.17,18 A study shows that patients with down-regulated miRNA-451a in the tumour have poorer survival,18,19 but increased circulating levels of miR-451a have also been described by the same authors. 20 miR-144-3p is a tumour suppressor gene aberrantly expressed in GC. 21 miR-144-3p is significantly decreased in GC tissue and diminished miR-144 expression is associated with a poor prognosis. 22 Its loss promotes proliferation, epithelial-to-mesenchymal transition and it has been associated with metastasis. 21 MET proto-oncogene (MET) and Pre-B-Cell Leukemia Transcription Factor 3 (PBX3) are the target of miR-144-3p in GC cells.21,23 Overexpression of MET is correlated with tumour invasion and prognosis in GC. 24 PBX3 was reported to play an oncogenic role in human cancers. 25 Therefore, it has been suggested that miR-144 may inhibit GC tumourigenesis by targeting MET and subsequently the PIK3/Akt pathway.16,26
Here, we have found that circulating miR-144-3p/miR-451a expression is diminished in GC patients when compared to a control group. The control group is a representation of Correa’s cascade towards GC, with patients with NAG, CAG and PLGC. Interestingly, plasma miR-144-3p/miR-451a are highly correlated and correlation is maintained when the dataset is split into NAG, CAG, PLGC and GC, supporting the concept that they are coexpressed because they belong to the same cluster.
To our knowledge, this is the first report to show that circulating miR-134-5p is deregulated in GC. We have found that miR-134-5p is up-regulated in GC patients when compared to the non-GC group. However, miR-134 has been found to be down-regulated27,28 in GC tissues and has been proposed to act as a tumour suppressor. The overexpression of miR-134 in gastric cell lines reduces proliferation by targeting Kirsten ras oncogene (KRAS) 28 and Golgi Phosphoprotein 3 (GOLPH3). 27 The inverse relationship between tissue and circulating levels has been found in certain miRNAs acting as tumour suppressors, though the origin of this discrepancy is unknown. 26
Although our findings support the deregulation of miR-144-3p, miR-451a and miR-134, their use in the clinical setting is limited by the moderate area under the curve (AUC). This is caused by the overlapping expression pattern between GC and non-GC.
The last c-miRNA validated is miR-196b-5p. miR-196b-5p is down-regulated in PLGC compared with NAG patients. Increased c-miR-196a/b has been previously associated to GC and its levels decrease after surgery; the combined miR-196a/b sensitivity and specificity was 71% and 98%. 29 In the present study, miR-196b was not significantly deregulated in GC patients. Multiple factors may be involved in this divergence. First, in our discovery set, the mean Cq for miR-196b-5p was rather high and detected in only 21% plasmas. Second, the normalization method was different. Tsai et al. 29 use miR-16, a miRNA associated with GC,19,20,30,31 although others have also used it.32–34
Our study has strengths. The first is that few studies have analysed c-miRNAs in European populations, the vast majority of studies being conducted in Asian populations where GC is more prevalent. This study also includes two independent cohorts, with patients from each stage of Correa’s cascade. Another strength concerns the methodology used. Sample processing was controlled by the use of spike-ins and the QC of data by determining PCR efficiency for each amplicon. The use of spike-ins technically controls the process of miRNA quantification, but it cannot correct other sources of variability such as the total concentration of the miRNA fraction that likely changes inter-individually. As a consequence, external controls are not useful for normalization and endogenous controls are required. Some authors use plasma volume 35 and others use referenced c-miRNAs. 36 As there is no consensus on how to normalise, we used the geNorm algorithm in our discovery cohort and applied the resulting stable c-miRNA in the validation set. This study also has some drawbacks. GC patients’ age may be a confounding variable. As the cascade from CAG to GC may take several years, some c-miRNAs may be affected by age. Using mirnacon, 36 a tool that tests miRNAs for their likelihood of being influenced by age, mir-144-3p levels (but not miR-185-5p/miR-451a) may be influenced by age.
In conclusion, c-miRNAs are altered with the progression from H. pylori infection to PLGC and GC, suggesting four c-miRNAs as potential biomarkers for PLGC and GC. However, higher sensitivity/specificity should be achieved for translation to clinical applications. Several points may help achieve this goal such as the analysis of miRNA isoforms, the study of extracellular vesicles containing miRNAs, or the use of innovative and sensitive methodologies with less steps.37,38
Supplemental Material
Supplemental material for Expression profile of circulating microRNAs in the Correa pathway of progression to gastric cancer
Supplemental material for Expression profile of circulating microRNAs in the Correa pathway of progression to gastric cancer by Sergio Lario, Anna Brunet-Vega, María E Quílez, María J Ramírez-Lázaro, Juan J Lozano, Lorena García-Martínez, Carles Pericay, Mireia Miquel, Félix Junquera, Rafael Campo and Xavier Calvet in United European Gastroenterology Journal
Footnotes
Acknowledgments
The authors are indebted to N Piqué for her help with English in this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was funded by Fundació la Marató de TV3 (1007/C/2013) and Fondo de Investigación en Salud (FIS), Instituto de Salud Carlos III, ISCiii (PI12/01802).
Ethics approval
The study was approved by the Ethics Committee (code: 2005511; approval date: 2006/1/11) in accordance with the Declaration of Helsinki.
Informed consent
All subjects provided signed informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.