
Abstract
Introduction
Colonoscopy is able to diagnose, resect and retrieve colonic polyps. Although retrieval of resected polyps is still globally advised, it is not always successful. We aimed to define the risk factors for polyp retrieval failure in colonoscopy.
Methods
A single-center, retrospective study assessed 3507 consecutive and non-urgent colonoscopies, performed between September 2011 and December 2012. Colonoscopies were included in our analysis if the diagnosis of at least one polyp was established, and one or more snare polypectomies were performed. Demographic and technical data were collected according to the patient’s endoscopy report.
Results
A total of 1109 polyps were analyzed, corresponding to 496 colonoscopies from 483 different patients. We found that 53 (4.8%) of the resected polyps were not retrieved. In a univariate analysis, the factors associated with polyp retrieval failure were: age, polyp size, resection technique, bowel preparation, location and the presence of a previous colorectal surgery (p < 0.05). In the multivariate analysis, a previous colorectal surgery, resection by cold snare, location in the right colon, inadequate bowel preparation and a polyp size up to 5 mm were independently associated with higher polyp retrieval failure (p < 0.05).
Discussion
Different and well-defined factors were associated with polyp retrieval failure. Because bowel preparation was the only modifiable factor identified, a special focus should be given to this topic.
Keywords
Introduction
Colorectal cancer (CRC) is the most common gastrointestinal cancer and the third most frequent cancer in the world. 1 Colonoscopy has an essential role in the diagnosis and prevention of CRC. The detection and removal of colonic polyps, namely adenomas and serrated polyps, lead to a decrease in CRC incidence.2,3
Although increasing evidence suggests that histological evaluation is not necessary for all resected polyps, this policy cannot yet be applied globally, in clinical practice. Histological evaluation of resected polyps is still advised to discard CRC as a risk, to classify the pre-malignant condition and subsequently, to schedule post-polypectomy surveillance. 4 Moreover, the polyp retrieval ratio is being increasingly considered as an important quality indicator in screening colonoscopy. The European Society of Gastrointestinal Endoscopy suggests that more than 90% of resected polyps should be retrieved for histological evaluation. 5 Nevertheless, the factors related to polyp retrieval failure have not been widely evaluated.6,7 We aimed to evaluate the prevalence of polyp retrieval failure and to identify the risk factors for this condition, in consecutive colonoscopies that were performed in a single tertiary referral center.
Materials and methods
A single-center retrospective study assessed 3507 consecutive, non-urgent colonoscopies performed between September 2011 and December 2012. From these, the procedures with a diagnosis of polyp(s) were automatically selected by a specific query for ‘polyp(s)’ in our endoscopy software (Siima®, First Solutions, Portugal). These reports were then manually revised and included in our study, if at least one snare polypectomy was performed. A total of 496 colonoscopies, corresponding to 483 patients, were finally considered for analysis. Written informed consent was obtained for all patients before the procedure.
Demographic and technical data were collected according to the endoscopy report. As globally recommended, 5 in our center the endoscopists are strongly advised to fulfill a detailed report describing each pathological finding, technique and adverse event. The database was created on a per-polyp basis, so that each resected polyp could be analyzed individually.
The endoscopy team was composed of an endoscopist and a nurse. A total of 14 different endoscopists (11 consultants and 3 fellows in training) performed the colonoscopies. The procedures performed by the fellows were always supervised by one of the consultants. These procedures were performed with the following colonoscopes: Olympus® CF Q165 L, CF Q180 L and rarely, CF Q2T160I and CF Q2T160L.
Colonoscopy depth
Total colonoscopy is defined by a successful cecal and/or ileal intubation. An incomplete colonoscopy refers to a colonoscopy that did not reach the cecum and/or the ileum. This may occur by an unsuccessful progression (e.g. loop or technical issues), patient intolerance or according to the aim of the colonoscopy (e.g. planned polypectomy in the sigmoid).
Polyp size
The size of each polyp was estimated during the procedure, according to its visual appearance, by visual analogy with a biopsy forceps. No ruler was used to measure the resected polyps.
Polyp location
The left-side colon includes the descending colon, sigmoid and rectum. The right-side colon is defined by the cecum, and ascending or transverse colon.
Deep sedation
Deep sedation was performed by a specific team, composed of an anesthesiologist and a nurse. Propofol (Diprivan® 1 mg/1 mL; 10 mL) was usually administered by bolus and/or perfusion. Supplemental oxygen was given by a nasal catheter, with no need for orotracheal intubation. The endoscopic team did not have any specific role in the sedation process.
Bowel preparation
Bowel preparation was classified into adequate (no stool or areas with residual stool and/or clear liquids that can be cleared by washing or suction) or inadequate (areas of solid stool that cannot be cleared). Although this is not a validated classification, it was well known and accepted by all endoscopists. Bowel cleansing solutions composed of polyethylene glycol (PEG) were taken by the great majority of patients evaluated.
Resection techniques
Cold snare polypectomy
Cold snare polypectomy (Endoflex® oval and hexagonal loops, 15 mm, Germany) was mainly performed to remove small polyps, usually up to 10 mm long. The recommended strategy in our department was the resection of the polyp without tenting first, and then suction of the transected polyp into a working channel.
Hot snare polypectomy
Hot snare polypectomy (Endoflex® oval and hexagonal loops, 15 mm and 25 mm, Germany) was our most common resection technique. The recommended strategy is resection after tenting, and then suction through the working channel. Piecemeal resection was also performed by hot snaring.
Polyp retrieval devices
A Roth net (Roth Net® 3.0 cm, USA) was used when needed. To collect suctioned polyps, a polyp trap (US endoscopy eTrap®, USA) was also used.
Statistical analysis
After data collection, we calculated the polyp retrieval failure ratio. The relationship between different factors and polyp retrieval failure was evaluated in a univariate analysis (Chi-square and student t tests). The factors with a significant association in the univariate analysis were then integrated in a multivariate analysis, in order to identify independent factors (p < 0.05).
Results
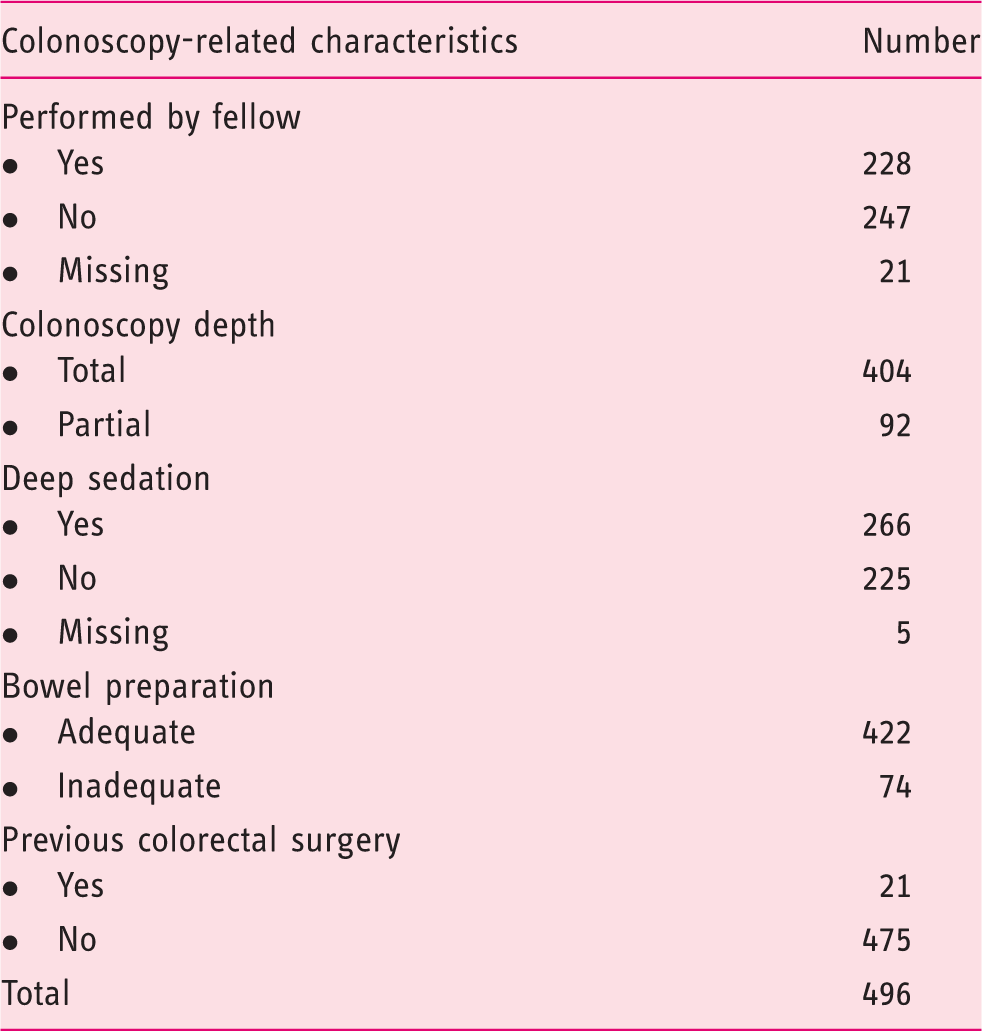
Colonoscopy-related characteristics
Relationship of each factor with polyp retrieval (univariate analysis)
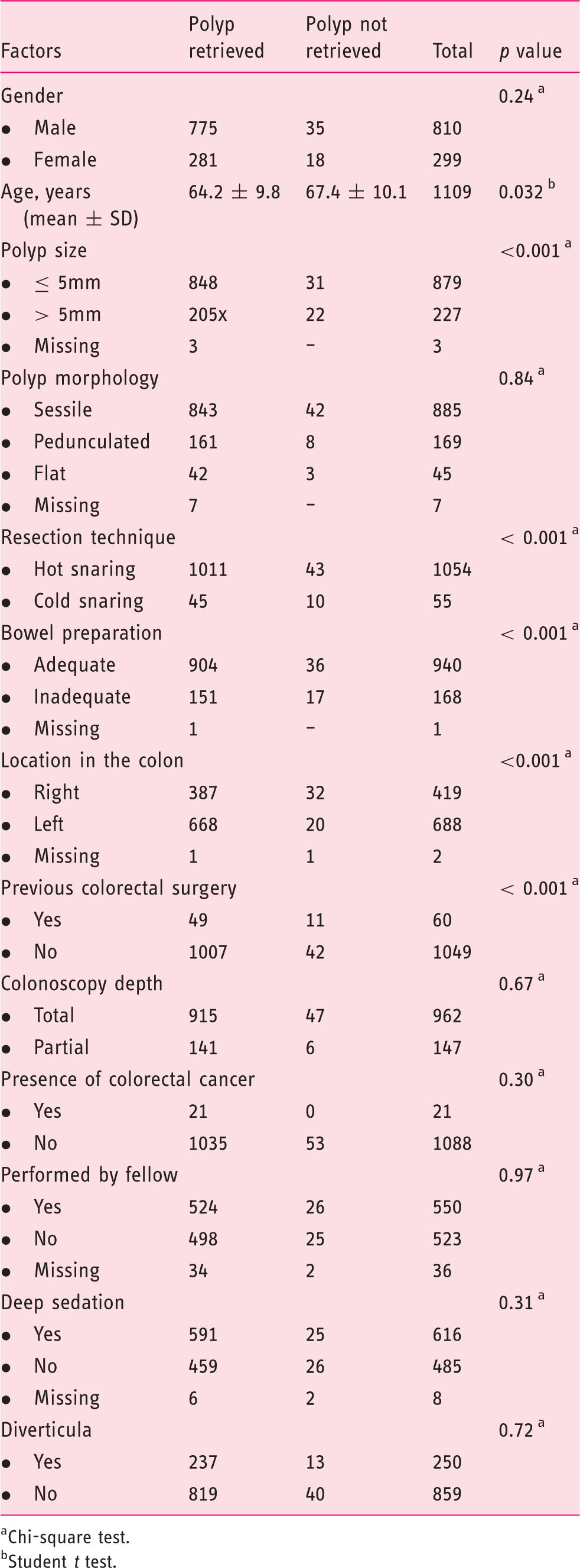
Chi-square test.
Student t test.
In the univariate analysis, an older age (p = 0.032), polyp size ≤5 mm (p < 0.001), cold snare resection (p < 0.001), inadequate bowel preparation (p < 0.001) and history of a previous colorectal surgery (p < 0.001) were significantly related with polyp retrieval failure. Table 2 describes the univariate analysis of each factor with polyp retrieval failure.
Binary logistic regression model OR (95% CI) for the association between different variables and polyp retrieval failure
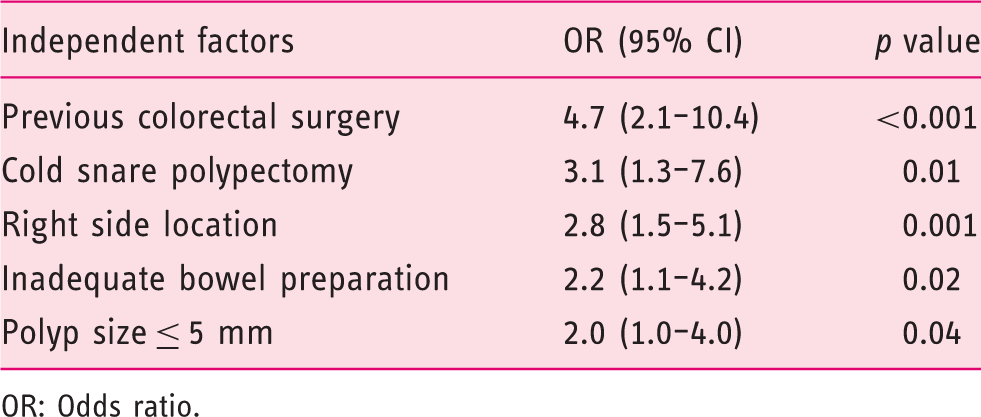
OR: Odds ratio.
Discussion
Colonic polyps are the most common finding in colonoscopy. They are usually a pre-malignant condition that can be diagnosed, resected and retrieved by colonoscopy. The resection of colonic polyps is able to reduce CRC incidence and mortality.2,3
Currently, some controversy exists about the need for histological analysis of resected polyps, mainly for diminutive polyps. A ‘predict, resect and discard’ policy was already suggested, based on an in vivo prediction of the polyp histology.4,8–10 Nevertheless, some limitations are still pointed to in this strategy; 4 , 11 hence, histological analysis of resected polyps is still advised, to exclude a malignant condition and to plan post-polypectomy surveillance.
Currently, a polyp retrieval ratio higher than 90% is a quality indicator in screening colonoscopies; 5 however, this is not always achieved, and polyp retrieval failure rates range between 2.5% and 16.2%.12–14 In our data, we achieved an acceptable polyp retrieval ratio, considering that only 4.8% of the resected polyps were not collected.
Factors related to polyp retrieval failure have not been widely defined.6,7 Recently, Komeda et al. 7 developed a prospective study addressing this issue. In this paper, a small polyp size and cold snare removal were independent factors for polyp retrieval failure. In our data, we achieved similar results. Moreover, we evaluated additional factors and obtained other independent factors.
The relationship between an inadequate bowel preparation and a high polyp miss ratio has already been widely discussed.15–18 Nevertheless, the relationship between bowel preparation and polyp retrieval failure is less documented. 7 In our sample, inadequate bowel preparation was independently associated with polyp retrieval failure. The presence of solid and non-aspirable stool and its mixing with the resected polyps may justify this result. Because this is a unique, modifiable factor, special focus should be given to an adequate bowel preparation and to suctioning of all fluids and aspirable stool prior to polyp resection.
A previous colorectal surgery was strongly associated to polyp retrieval failure. A previous hysterectomy has been related to incomplete colonoscopy, because of a higher frequency of loops and post-operative fixations. 19 These mechanisms may also occur in patients with a previous colorectal surgery and interfere with the polyp retrieval ratio. Of note: Although a previous colorectal surgery has been associated to inadequate bowel preparation,20,21 these two factors were independent in the multivariate analysis.
The association between cold snare polypectomy and polyp retrieval failure is controversial.7,22,23 In our department, cold snare polypectomy is usually performed without previous tenting and immediately followed by suction of the resected polyp into the working channel. A similar technique has been described in previous studies with a high polyp retrieval ratio. 23 The associated factor cold snare polypectomy may be related to a rapid polyp migration after resection, which can hamper polyp retrieval.
Polyps located in the right colon were independently related to polyp retrieval failure. The eventual presence of a loop and consequent poor handling of the colonoscope in the right colon may contribute to this result. Moreover, the presence of a large lumen with prominent folds may promote the loss from sight of resected polyps.
Polyps up to 5 mm in length were also independently related to polyp retrieval failure. Small polyps are easily lost from sight and they are also hard to find. Moreover, taking into account their thin insertion in the mucosa, they can easily displace from their original site after resection. These mechanisms may justify this relation.
We acknowledge some limitations to our study. We performed a single-center retrospective study. Nevertheless, the relevance of retrieving all the resected polyps was well known and accepted by all endoscopists. Hence, the retrieval of resected polyps was a common goal in all polypectomies. Furthermore, although data collection was based on the endoscopy report, the elaboration of a detailed colonoscopy report is routinely pursued by all the endoscopists in our center.
The duration of each procedure and the retrieval time for each polyp were not evaluated. Moreover, the relationship between polyp retrieval failure and each endoscopist was not addressed. Also, three fellows performed colonoscopies under direct supervision of one consultant. Although the performance by fellows could be expected to be related to a higher polyp retrieval failure, this was not found in our study.
Lastly, the link between polyp retrieval failure and the time of the day (e.g. morning versus afternoon) or the number of exams in each shift was also not evaluated. Nevertheless, the effect of these factors in the adenoma detection rate is still not consensual.24,25
In conclusion, a previous colorectal surgery, cold snare polypectomy, right-side location of polyps, an inadequate bowel preparation and polyps≤5 mm long were independently and positively related to polyp retrieval failure.
Because retrieval of resected polyps is globally recommended, intervening in factors related to polyp retrieval failure is of paramount importance. When these factors are present, endoscopists should take even more extra care during and after polypectomy, in order to maximize the chances of polyp retrieval. Moreover, as bowel preparation is the only modifiable factor, we may achieve a higher polyp retrieval ratio by reinforcing the importance of bowel preparation to our patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declare there are no conflicts of interest.