
Abstract
Stricturing Crohn’s disease (CD) is a significant clinical problem. The presence of a stricture may be suggested by clinical symptoms. Cross-sectional imaging using computed tomography or magnetic resonance enterography is essential in diagnosing strictures as it allows further characterization and evaluation for complications such as abscess, fistulizing disease or malignancy. Managing small bowel stricturing CD should be approached in a multidisciplinary fashion. Medical therapy can be considered in strictures which are not associated with complications, with most of the data supporting anti-TNF strategies in this setting. If the disease is refractory to medical therapy, endoscopic therapy or surgery should be performed. Endoscopic balloon dilation (EBD) is an option for short, uncomplicated and straight strictures that are within reach of a colonoscope. Although EBD has good short-term outcomes, repeat dilation is often required. Surgical options mainly include resection and strictureplasty. Strictures refractory to medical therapy, not amenable or refractory to EBD, or associated with complications or malignancy should be managed surgically. However, surgery may also be considered at an earlier stage depending on disease characteristics and patient preference. Postoperative recurrence is common, highlighting the importance of careful monitoring of the patient postoperatively and optimization of medical management accordingly. There is a pressing need to develop anti-fibrotics for the treatment of stricturing CD. This requires the development of standardized diagnostic criteria, patient-reported outcome measures and validation of endpoints in fibrostenotic CD. The STAR consortium is pioneering this effort in order to allow development and testing of anti-fibrotics in future clinical trials.
Keywords
Clinical case
A 35-year-old male patient with a known history of ileocolonic Crohn’s disease (CD) presents with post-prandial abdominal pain, abdominal distention, nausea and vomiting for 1 month. Magnetic resonance enterography (MRE) shows wall thickening and contrast enhancement in the distal ileum, over a segment of approximately 5 cm in length. It is associated with luminal narrowing and pre-stenotic small bowel dilation of up to 3 cm. There are no associated sinus tracts or fistulas.
Natural history of stricturing Crohn’s disease
Although most patients with CD present with an inflammatory phenotype at time of diagnosis, about 10% of patients exhibit a stricturing phenotype. 1 According to population-based studies using the Montreal classification, the probability of progression to stricturing CD is about 15% at 10 years and 21.6% at 20 years. 2 Strictures are a main indication for surgery in CD. About 40–70% of patients overall require surgical treatment for a complication (e.g. stricture, fistula, abscess) 10 years after diagnosis. 3 Unfortunately, postoperative recurrence is common and usually occurs at the ileocolonic anastomotic site, driving re-stricturing and need for redo surgery. 4
The development of fibrostenosis is likely the result of a combination of inflammation-dependent and -independent processes. Although fibrosis in inflammatory bowel disease (IBD) has been traditionally viewed as a consequence of inflammation only,2,5 no change in progression to fibrostenosing CD has been shown despite the introduction of anti-TNF therapy, even early after diagnosis.6–8 This may be explained by the fact that at time of diagnosis (which is considered an “early” treatment point in most publications) tissue damage has already occurred and the process became independent of inflammation. Fibrosis results from the activation of mesenchymal cells, which in turn leads to the excessive accumulation of extracellular matrix. This appears to originate from different profibrotic pathways involving molecules such as TGF-β, tyrosine kinases, IL-13, IL-36, etc. Inflammation is also an important driver of fibrosis through the release of profibrotic factors. A detailed discussion of the pathogenesis of fibrosis is beyond the scope of this review but has been described elsewhere. 5
Fistulizing disease is often found in conjunction with stricturing disease. It is commonly thought to be due to progression of disease from an underlying stenosis, given the fact that most internal fistulae are upstream of the stricture and originate from the area of pre-stenotic dilation. This theory, however, is largely anecdotal and has not been supported by prospective data. 5 In a retrospective study, an underlying stricture was found in most patients with internal fistulizing CD, such that fistulas had a positive predictive value of 86.2% for the diagnosis of a stricture. 9
Although no accurate predicting factors have been identified for the development of stricturing disease, several risk factors were associated with the development of a stenosis in the prospective multicenter TREAT registry and in the ACCENT I trial: duration of disease, severity of disease, ileal location of disease, and new corticosteroid use. 10 Infliximab was not found to be associated with increased rates of stenosis, which helped debunk the opinion that anti-TNF therapy may drive stricture formation through rapid healing. Only colonic disease was shown to be protective. 10
Strictures can occur anywhere in the gastrointestinal tract, but are most commonly found in the small bowel and follow the distribution of inflammation in CD. 11 Colonic CD strictures are less common and associated with a higher rate of dysplasia. In a large French retrospective study, 2.4% of colon strictures were ultimately found to be associated with dysplasia or cancer despite thorough sampling during colonoscopy which did not show any signs of dysplasia or malignancy prior to resection. 12 Strictures can also occur in ulcerative colitis (UC) and are found in 2–11.2% of patients. 5 Although their malignant potential should be strongly considered, more than 70% of strictures in UC are in fact benign. 13 In a series of 59 patients with UC and strictures, some of the factors associated with malignant potential were a location proximal to the splenic flexure, duration of disease longer than 20 years, and strictures associated with large bowel obstruction. 13
Diagnosis
Stricturing CD may be diagnosed by different modalities. Clinically, it may be suggested by obstructive symptoms, such as post-prandial abdominal pain, distention, nausea, vomiting and dietary restrictions. However, symptoms correlate poorly with the presence of a stricture and further testing is essential. 14 Endoscopy typically shows a narrowed lumen which cannot be traversed. Endoscopic scores such as SES-CD and CDEIS have incorporated stenosis as part of their scoring system and have defined stenosis as an area that is impossible or difficult to pass with an adult colonoscope.15,16 In an effort to standardize the diagnosis of stricturing disease, the CrOhN’s disease anti-fibrotic STRICTure therapies (CONSTRICT group), an international panel of experts, has devised the endoscopic definition of a stricture as “inability to pass an adult colonoscope through the narrowed area without prior endoscopic dilation with a reasonable amount of pressure applied.” 14
Although biopsies should be performed in order to rule out underlying dysplasia or malignancy, it is important to note that biopsies may miss underlying dysplasia and cannot inform about the deeper layers of the intestine. Furthermore, there are no validated histology scoring systems to quantify the severity of fibrosis. A recent systematic review led by the Stenosis Therapy and Research (STAR) consortium found significant heterogeneity in histopathologic scores used to evaluate fibrostenotic CD, therefore highlighting the importance of the development of a validated histologic index to be used as a possible endpoint in future clinical trials. 17 This work is currently ongoing.
Diagnostic accuracy of ultrasound, CT enterography and MR enterography in identification of strictures in studies comparing imaging to histopathology. Values are provided as ranges. Adapted from Bettenworth et al. 18

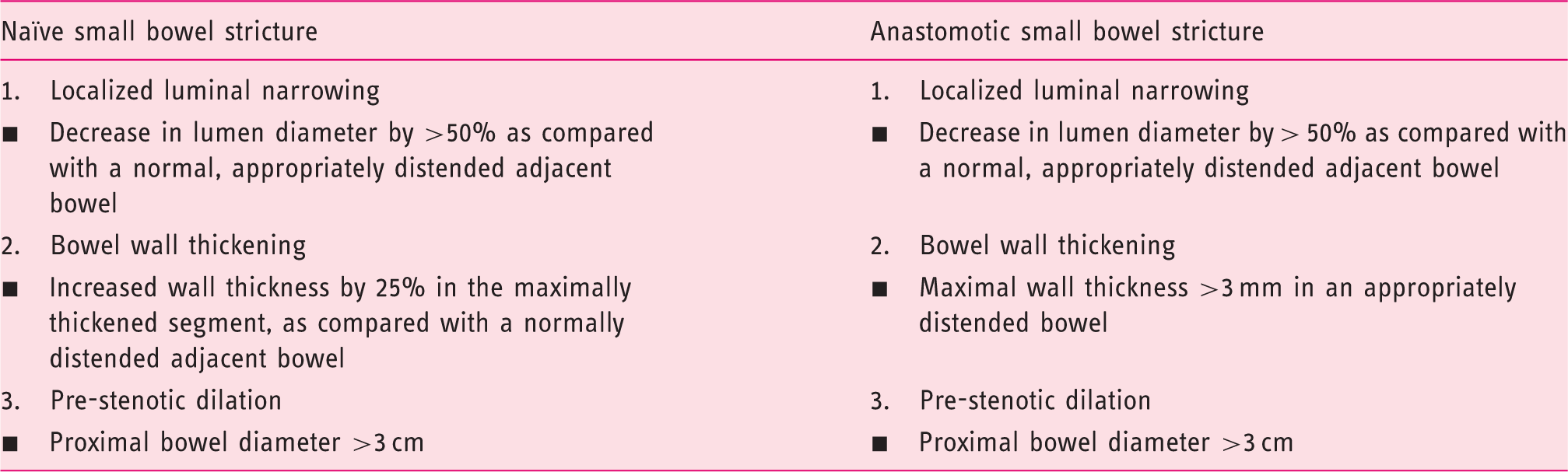
Definition of small bowel strictures according to the CONSTRICT criteria. The combination of all three features should be present to diagnose a stricture on cross-sectional imaging. Adapted from Rieder et al. 14
Determining the degree of inflammation and fibrosis in a stricture can help guide management, but is often difficult as both elements coexist in most patients. 5 MRE appears to be the most accurate in assessing the degree of fibrosis and inflammation, though no imaging modality to date can reliably quantify the degree of fibrosis in stricturing CD.18,23 Indeed, MRI was shown to differentiate between mild–moderate and severe fibrosis deposition with a sensitivity of 94% and a specificity of 89% using percentage of enhancement gain. 24
Novel imaging modalities are being evaluated, such as magnetization transfer MRI, MR with dynamic contrast enhancement and ultrasound elastography; however, these are not ready to be used in clinical practice. 5
Current management
Managing small bowel stricturing CD should be approached in a multidisciplinary fashion, involving input from gastroenterologists, colorectal surgeons, radiologists and pathologists, if necessary. 23 In the acute setting of a CD-related small bowel obstruction, the patient should be hospitalized and promptly evaluated both clinically and by cross-sectional imaging in order to assess the disease and rule out complications such as perforation, abscess or fistulizing disease as well as any signs of underlying malignancy. Patients are initially kept nil per os until decompression is achieved. Hydration, electrolyte replacement and insertion of a nasogastric tube are often required; the C-reactive protein and abdominal X-rays are often reviewed daily. Intravenous corticosteroid therapy is typically started if there is an inflammatory component, despite limited supporting evidence. One study found that 25/26 patients with acute obstruction responded to intravenous corticosteroids within 72 h; however, only 28% remained obstruction-free at 52 months. 25 In the case of persistent obstruction, biologic treatment, endoscopic balloon dilation (EBD), surgery or a combination thereof are often necessary. The management depends on stricture characteristics (such as inflammatory component, length, location), patient preference and the presence of complications such as a phlegmon, fistula, or abscess. 26
Medical therapy
Anti-tumor necrosis factor (anti-TNF) agents have been evaluated in the medical management of stricturing CD. Although they were initially thought to increase stricturing through healing inflammation, more recent data, including data from the TREAT registry and the ACCENT I trial, do not support this finding and have found them to be safe and effective.10,27–30 Adalimumab was evaluated in a prospective observational cohort study in patients with stricturing small bowel CD (the CREOLE study). At week 24, 64% of patients were still on adalimumab without the need for additional therapy (e.g. EBD or surgery), and 50.7% of patients remained surgery free at 4 years. 31 Other biologics such as vedolizumab or ustekinumab have not been evaluated in this setting.
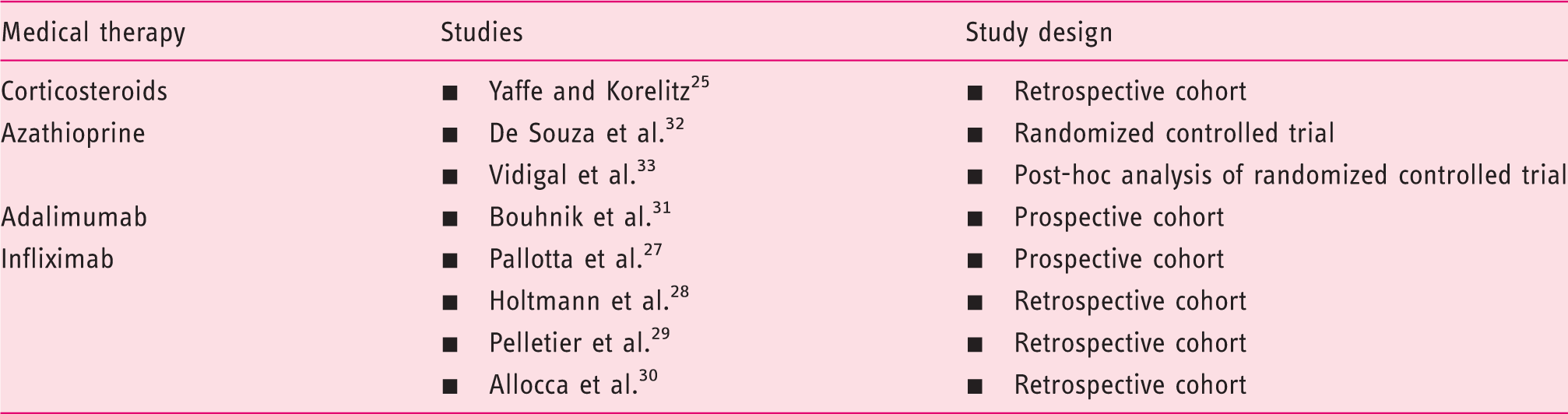
Summary of medical therapies and their evidence in small bowel stricturing Crohn’s disease
Endoscopic therapy
If the disease is refractory to medical therapy, endoscopic therapy or surgery should be performed. EBD is an option for strictures that are short (<5 cm long), straight, and accessible with an endoscope or colonoscope. It should not be performed in the setting of complications, i.e. penetrating disease or suspected malignancy.
5
EBD can be attempted in naïve and anastomotic strictures with similar success rates.
34
EBD is most commonly performed using a through-the-scope balloon, in either retrograde or anterograde fashion, and can be performed in upper gastrointestinal, small bowel and colonic strictures.
26
However, duodenal strictures appear to be five times more likely to necessitate earlier surgery after dilation compared with strictures in the jejunum, ileum or colon.
34
Although EBD can be performed in colonic strictures, surgery should be considered given the higher risk of malignancy in this setting compared with small bowel strictures.
12
A practical guide to EBD can be found in Figure 1.
Key considerations prior to endoscopic balloon dilation of IBD strictures.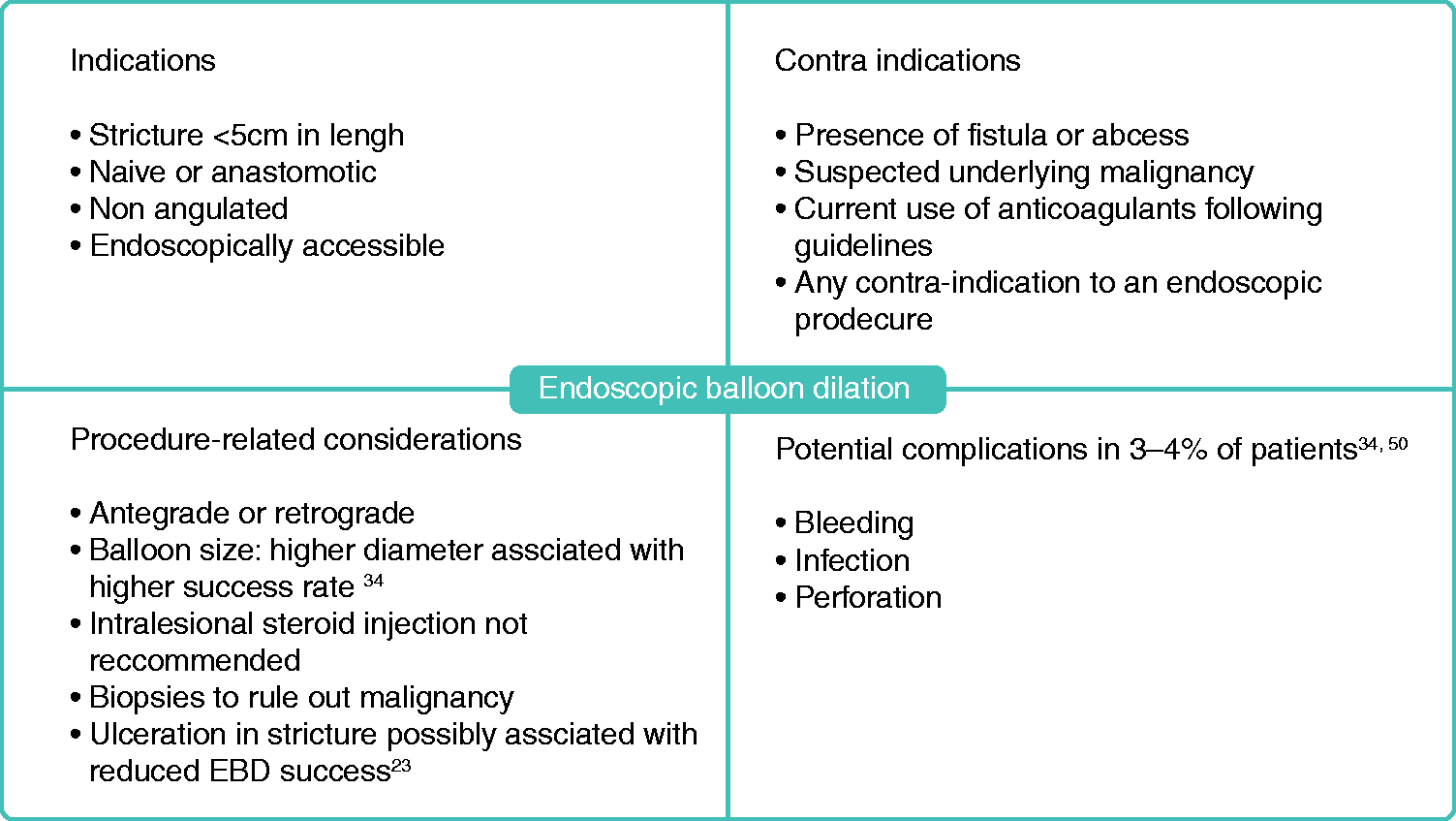
A systematic review including 1463 patients and a total of 3213 EBD procedures found a technical success rate of 89.1%, with clinical efficacy in 80.8% of cases; 42.9% of patients underwent surgical resection at 24 months. Complications occurred in 2.8% of procedures and included perforation, fever and bleeding.
34
Ulceration in the stricture was not associated with increased rates of complications.
34
However, available studies were observational and therefore susceptible to bias toward possible avoidance of EBD in patients with underlying inflammation. Factors such as length <5 cm, absence of ulcerations in the stricture, and technically successful EBD were found to be associated with clinically successful short-term outcomes.
23
However, repeat dilation is often required—up to 73.5% at 2 years in the previously mentioned study
34
—but does not appear to be associated with an increased risk of complications over time.
23
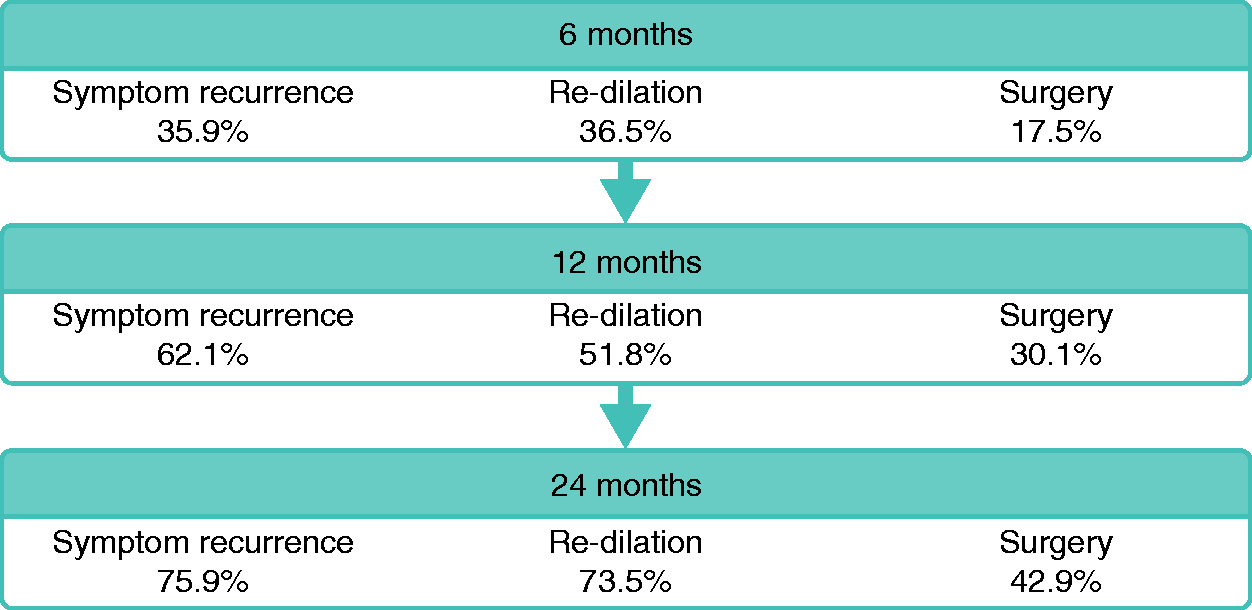
A summary of short-term and long-term outcomes of EBD can be found in Figure 2.
Short and long-term outcomes of EBD: Symptom recurrence, need for re-dilation and need for surgery at 6, 12 and 24 months. Adapted from Bettenworth et al.
34
Other endoscopic modalities have been evaluated such as stent insertion, intralesional steroid or anti-TNF injection but cannot be recommended for routine practice given limited evidence. 26 Needle-knife stricturotomy has been found to have promising short-term outcomes and warrants further exploration, in particular in controlled settings and with a thorough evaluation of complication rates. 35
Surgery
Surgical options include segmental resection and strictureplasty. Strictures refractory to medical therapy, not amenable or refractory to EBD, or associated with complications or malignancy should be managed surgically. 23 However, the timing of surgery appears to be important. Early resection, either at diagnosis or shortly after diagnosis in ileocecal stricturing CD was found to be associated with longer clinical remission, 36 decreased risk of repeat surgery 37 and decreased overall exposure to steroids and biologic therapies. 38 Therefore the decision to proceed with surgery earlier on after stricture diagnosis should be considered and based on disease and stricture characteristics as well as patient preference. 23
Strictureplasty is a bowel-sparing approach. It is preferred in patients with prior extensive resections or at risk of short bowel syndrome. Contra-indications include suspected malignancy, penetrating complications, malnutrition and colonic strictures. The Heineke–Mikulicz technique is typically performed for short strictures (<10 cm) and the Finney technique for intermediate length strictures (10–20 cm), whereas the “non-conventional” strictureplasty such as the Michelassi is rarely performed for very long areas of continuous disease. 39 Interestingly, recurrence at the site of strictureplasty is uncommon and most recurrences occur at a different site. 39 An ultrasound study has in fact shown a decreased bowel wall thickness at the site of strictureplasty over time, and observational data indicate that regression of stricturing disease occurs.40–42 For upper gastrointestinal stricturing CD, bypass surgery is an additional surgical option. 26
Of note, smoking cessation and optimization of nutritional status and anemia are important steps in management and should be addressed in all patients. In addition, patients may need to be on medical therapy postoperatively according to risk factors, and should be monitored closely for recurrence regardless of medical treatment.23,43
Perspective
Despite recent advances in the management of IBD, surgery is often necessary and postoperative recurrence is common. 4 Current biologic therapies address inflammation, but no available agents target fibrosis. Several promising molecules are being evaluated. 44 AMA0825, a Rho-associated protein kinase inhibitor, was found to reverse intestinal fibrosis in mice and reduce the secretion of pro-fibrotic markers in CD biopsies. 45 Tranilast exhibits anti-fibrotic properties through reduction of TGF-β activity in rats. 46 It was evaluated in a prospective study in patients with asymptomatic CD strictures and was associated with higher rates of asymptomatic patients compared with controls over a median observation period of 782 days. 47 The peroxisome proliferator-activated receptor gamma agonist GED-0507-34 indicated anti-fibrotic properties in mice. 48 More recently, an antibody to the IL-36 receptor was found to decrease fibrosis in mice with chronic intestinal inflammation. 49 More detailed mechanistic information can be found in a separate review on this topic. 5
There is a pressing need to develop and evaluate anti-fibrotics for the treatment of stricturing CD. This requires the development of standardized diagnostic criteria, patient-reported outcome measures (PROs) and validation of endpoints for fibrostenotic CD. The STAR consortium, an international group of experts, is laying the groundwork for this and has proposed consensus-based definitions of strictures in CD, as well as diagnostic criteria. Endpoints to be used in future clinical trials are currently being built, which includes PRO, radiology and histopathology indices. 14 The PRO and radiology indices are being validated in a prospective clinical study.
Footnotes
Acknowledgment
SE and FR planned, conducted the study and drafted the manuscript. All authors have contributed to drafting the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
FR is on the advisory board or consultant for AbbVie, Celgene, Receptos, Thetis, UCB, Samsung, Pliant, Boehringer-Ingelheim, Helmsley, RedX, Thetis, Gossamer, Pfizer, Gilead, Takeda and Roche. BC is on the speaker’s bureau for Takeda.
Funding
This work was supported by the Helmsley Charitable Trust through the Stenosis Therapy and Anti-Fibrotic Research (STAR) Consortium.