
Abstract
Background
The caecal intubation rate (CIR) is an important quality standard for endoscopists, as well as for national bowel cancer screening programmes; however, individuals undergoing colonoscopy for bowel screening and symptomatic patients represent different groups, and their characteristics may affect colonoscopy performance.
Objective
To compare colonoscopists’ performance, as assessed by the CIR, in symptomatic patients compared to individuals undergoing colonoscopy for bowel cancer screening.
Methods
Retrospective audit of CIRs for all patients undergoing colonoscopy at our institution during the year 2008. We retrieved the data from an endoscopy reporting software database and from the local bowel cancer screening programme database. Demographic data was extracted, as well as details of known factors that may affect completion of colonoscopy, such as poor bowel preparation, presence of diverticular disease, polyps, tumour and strictures. The unadjusted CIRs for colonoscopists participating in the screening programme were compared between the bowel screening and the symptomatic patient groups.
Results
Five screening colonoscopists performed 1056 colonoscopies, of which 488 were bowel screening procedures. The overall CIR was significantly lower in the symptomatic, compared to the screening, individuals (88.5% versus 93%, P < 0.02). No significant differences were observed between the two groups for risk factors that could impair the CIR. The CIR was <90% for two of the five colonoscopists in symptomatic patients, and just under 90% for one colonoscopist in screening individuals. Multivariate analysis revealed that non-screening colonoscopy was an independent predictor for an incomplete procedure (OR 1.8; 95% CI 1.2–2.8).
Conclusions
The CIR, a key quality performance indicator for colonoscopy, is lower in symptomatic patients compared to individuals undergoing colorectal cancer screening. These results suggested that CIR should be monitored independently in screening and non-screening colonoscopies.
Keywords
Introduction
Colonoscopy plays a critical role in colorectal cancer screening in many countries, either as a first-line test or as a second-line screening modality, after faecal occult blood or immunochemical testing. 1 Whilst it is widely accepted as the gold standard for detecting neoplasia of the colon, it is associated with a small but significant risk of morbidity (such as perforation or bleeding) and mortality. 2 In order to deliver high quality colonoscopy for all patients, the British Society of Gastroenterology (BSG) and the US Multi-Society Task Force on Colorectal Cancer developed quality and safety indicators for endoscopy.3,4 The performance of a ‘complete colonoscopy' by passage of the colonoscope along the whole length of the colon to the caecum or terminal ileum/neo-terminal ileum, is a key parameter for measuring the quality of the procedure. The standard for the caecal intubation rate (CIR) is set at an unadjusted rate of 90%, i.e. irrespective of any pathology encountered.3,4 Several factors have been identified that can impair the CIR, including: increasing patient age,5–7 female gender,6,7 poor bowel preparation,8,9 presence of diverticulosis5,9 and obstructing tumours. 9
Symptomatic patients may have different characteristics compared to asymptomatic individuals undergoing colonoscopy for colorectal cancer screening. The Bowel Screening Programme (BSP) in Scotland commenced roll-out in 2007, following the UK demonstration pilot. 10 It is based on the guaiac-faecal occult blood test (FOBT), with test-positive individuals being invited to undergo colonoscopy. This screening strategy has been well evaluated, with a recent meta-analysis demonstrating that the risk of disease-specific mortality can be reduced by 25% using FOBT screening. 11 In Scotland, UK, the FOBT is offered on a biennial basis to all individuals aged between 50 and 74 years of age.
Recently published data suggests a lower CIR in symptomatic patients, compared to patients undergoing screening, although individual colonoscopists’ performance was not evaluated.7,12 The aim of this study was to compare colonoscopists’ performance, as assessed by CIR in symptomatic patients compared to individuals undergoing colonoscopy for colorectal cancer screening.
Methods
We performed a retrospective audit of CIRs for all patients undergoing colonoscopy at our institution during the year 2008. We retrieved the data from an endoscopy reporting software database (Unisoft Medical Systems, Enfield, UK), which records CIR as defined by intubation of the caecum/terminal ileum or neo-terminal ileum. We retrieved additional data from the local BSP database (Microsoft Access). We extracted the demographic data, as well as details of known factors that may affect completion of colonoscopy, such as: poor bowel preparation (recorded within Unisoft as ‘good’, ‘satisfactory’ or ‘poor’), presence of diverticular disease, polyps, tumour and strictures.
Colonoscopies were performed, as per local policy, after bowel cleansing with Picolax® (sodium picosulphate plus magnesium citrate, Ferring Pharmaceuticals, Berkshire, UK), with two sachets administered on the day prior to the procedure, as per the manufacturer’s instructions. The procedures were performed under conscious sedation with Midazolam (median dose 2.5 mg) plus Pethidine (meperidine hydrochloride, median dose 25 mg). Olympus Evis Lucera equipment was used with 260 series colonoscopes.
Caecal intubation rates for those colonoscopists participating in the BSP were compared between the bowel screening and symptomatic patient groups.
Statistical tests
We used the Fisher’s exact test to compare the characteristics between the BSP and symptomatic patient groups. The unpaired student's t-test was used to compare the age of patients between these two groups. We used 2-tailed statistics throughout and deemed a P < 0.05 as statistically significant. We also performed binary logistic regression, to assess predictors of incompletion of colonoscopy for individual colonoscopists, as well as for the pooled group. We excluded benign strictures from the regression analysis, due to there being a very small number of them. We expressed our results as an Odds Ratio (OR) with a 95% Confidence Interval (CI).
Results
Demographic details and CIRs for individuals undergoing colorectal cancer screening in the BSP and symptomatic patients
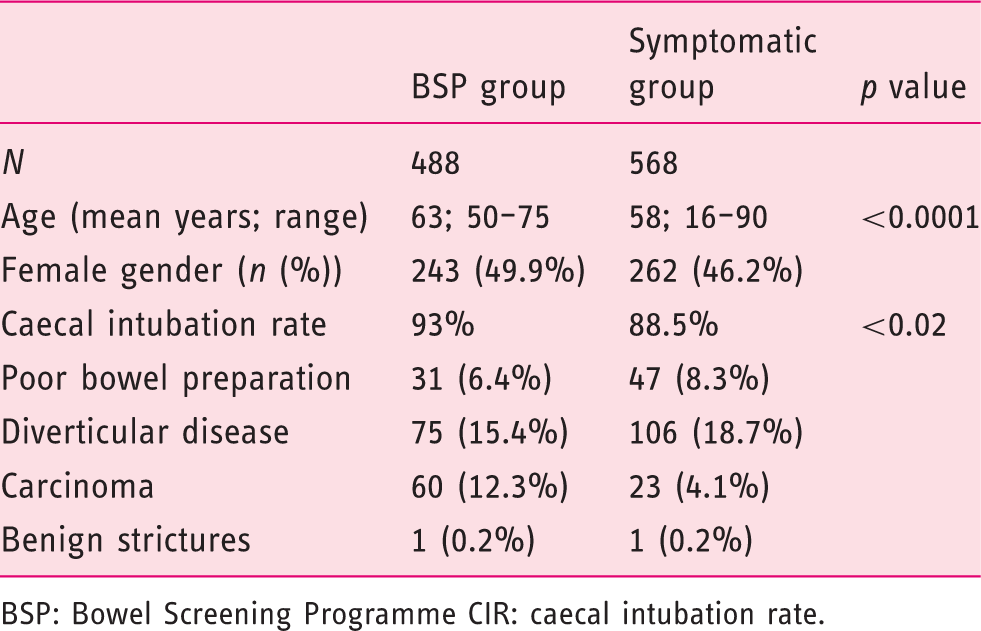
BSP: Bowel Screening Programme CIR: caecal intubation rate.
Multivariate analysis for predictors of incomplete colonoscopy in the BSP
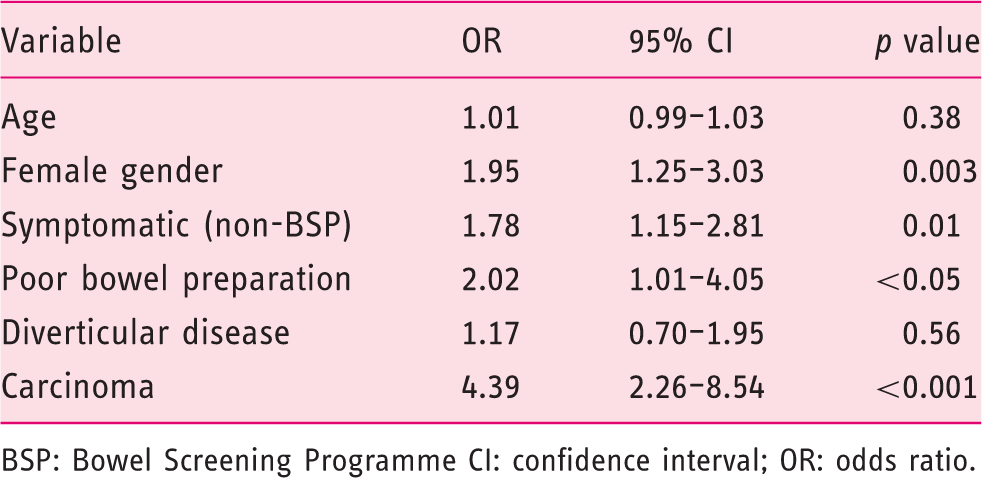
BSP: Bowel Screening Programme CI: confidence interval; OR: odds ratio.
CIRs for individual colonoscopists, with numbers of procedures in parentheses
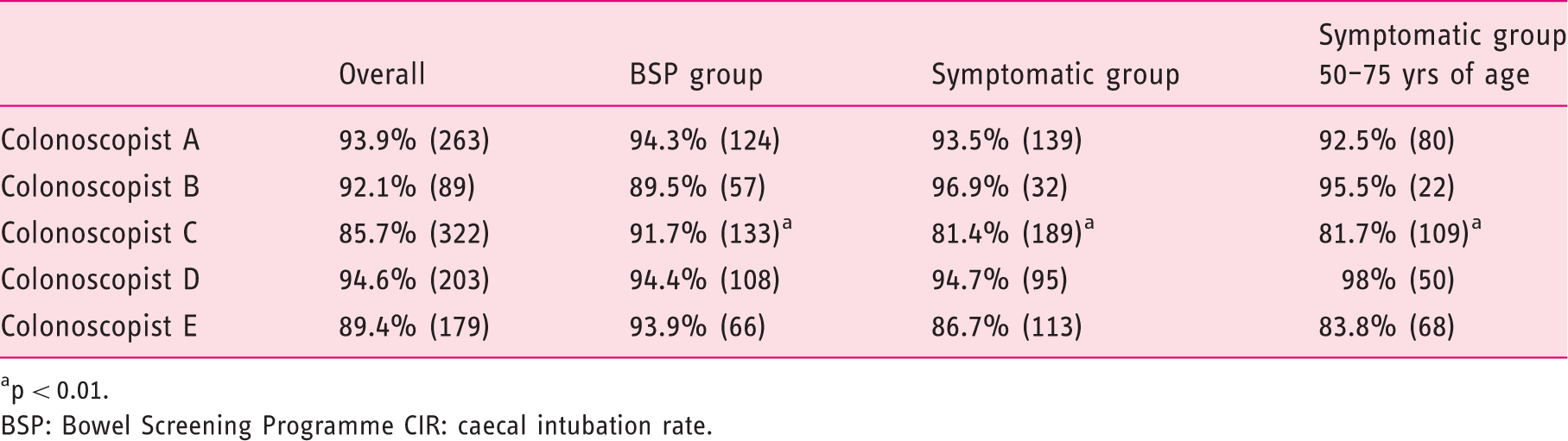
p < 0.01.
BSP: Bowel Screening Programme CIR: caecal intubation rate.
In order to adjust for any effect of age on the observed differences in CIRs, the BSP group of patients was compared to only the symptomatic patients aged 50–75 years; however, even when comparing with just the 50–75 year age group, the CIRs for colonoscopist C and colonoscopist E remained <90% in the symptomatic group.
Comparison of factors influencing CIRs between colorectal cancer screening (BSP) and symptomatic patients, for individual colonoscopists
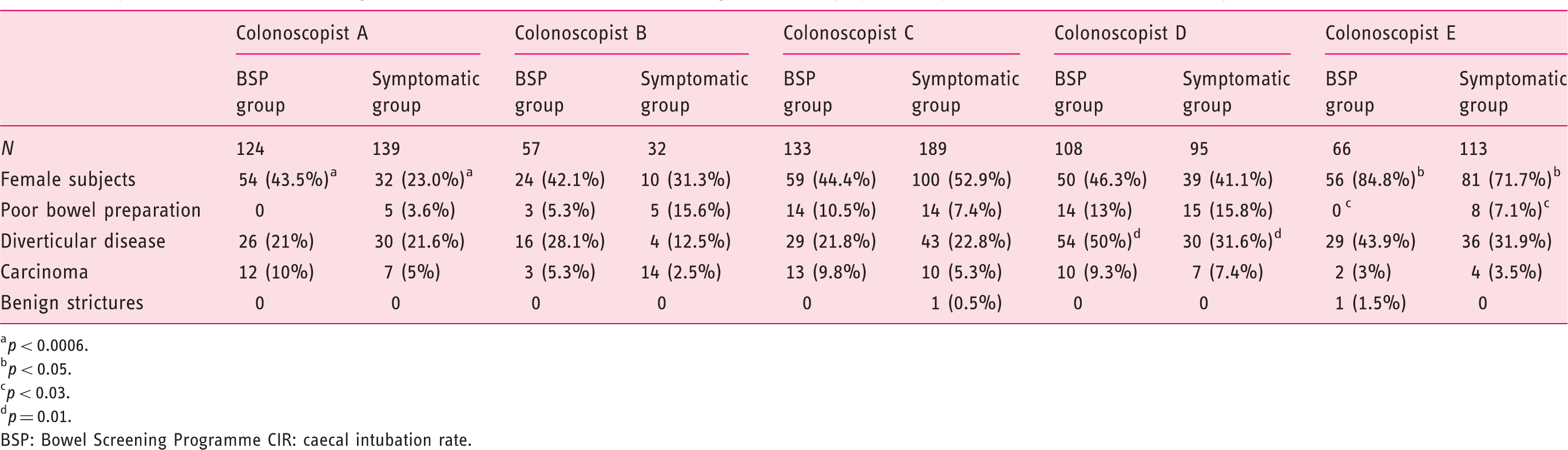
p < 0.0006.
p < 0.05.
p < 0.03.
p = 0.01.
BSP: Bowel Screening Programme CIR: caecal intubation rate.
For colonoscopist C, significant predictors of incomplete colonoscopy on multivariate analysis were symptomatic (non-BSP) patients (OR 2.69; 95% CI 1.27–5.66; p < 0.01) and the presence of carcinoma (OR 5.00; 95% CI 1.67–15.00; p < 0.01); for colonoscopist E, the only predictor was poor bowel prep (OR 2.14; 95% CI 0.92–5.46; p < 0.02).
Discussion
The quality of endoscopic procedures, including colonoscopy, has come under increasing scrutiny in recent times, partly in response to the roll-out of national bowel cancer screening programmes. Quality standards have been produced in the UK and USA, both for endoscopy units and individual endoscopists.3,4 For colonoscopy, the CIR is a key performance standard. This study’s results demonstrated that the CIR in symptomatic patients is lower than in individuals undergoing colorectal cancer screening. This finding is in line with previous studies7,12; Verma et al. found that the CIRs for screening colonoscopists were higher than for non-screening colonoscopists, and this accounted for the observed difference in CIRs between screening and symptomatic patient groups 12 ; however, we demonstrated that even when looking at just screening colonoscopists, there is still a persistent difference in CIRs between these two groups of patients. On multivariate analysis, non-screening colonoscopy was an independent predictor for an incomplete procedure.
Recognised factors that can impair the CIR include: increasing patient age,5–7 female gender,6,7 poor bowel preparation,8,9 presence of diverticulosis5,9 and obstructing tumours. 9 Our results have confirmed the importance of female gender, poor bowel preparation and the presence of tumours; however, we did not demonstrate any significant differences in the proportions of patients with these factors, between the screening and symptomatic groups of patients.
The CIR may also be impaired if there is a history of hysterectomy,6,7,13 prior abdominal surgery,6,7 operator fatigue 14 and in women with a low body mass index (BMI). 15 Due to the retrospective nature of our study, we did not have relevant data available to examine the influence of these factors on the CIRs. The presence of co-morbidity may also influence the CIR and it is likely that symptomatic patients would be less fit than the asymptomatic screening population. A colonoscopist may be less inclined to continue with a difficult procedure in an older patient with co-morbidity, because of the higher risk of adverse outcomes; unfortunately, such co-morbidity information was not available for our patients.
Another possible explanation for the observed difference in CIR between screening and symptomatic patients could be the timing of the colonoscopies in the two groups. It has been demonstrated that colonoscopies undertaken in the afternoon, as compared to the morning, have a lower CIR.16,17 The BSP colonoscopy sessions at our institution during the period of study were all scheduled in the morning, whilst sessions for symptomatic patients would have taken place in the mornings and afternoons. Furthermore, Harewood et al. observed that operator fatigue resulted in a reduction in the CIR with successive colonoscopies performed during a session. 14 At our institution, the BSP sessions tend to have fewer patients booked (4 versus 5 sessions for symptomatic patients). Furthermore, there may be additional time-pressures on the non-screening sessions, due to the possible addition of emergency cases.
A particular feature of our study is the data presented for the individual CIR performance of colonoscopists. This demonstrated that although all colonoscopists had a CIR of >90% (or in one instance just below 90%) in BSP patients, there was more variation between colonoscopists in the symptomatic group and in the overall CIR. On evaluating some of the more well-recognised risk factors that impair the CIR, there were no consistent findings to explain the observed variation. Although, it has been suggested that the CIR correlates positively with the number of procedures performed, 18 it is of note that one of the colonoscopists in this study with a low CIR actually performed the highest number of procedures.
The slightly lower CIRs that we found for some of the colonoscopists may reflect differences in their case mix that we were unable to evaluate. For example, the presence of a trainee may lower the overall CIR. 7 Colonoscopist C, one of the individuals with a low CIR, was the only one of the five colonoscopists in our study who was also supervising colonoscopy training sessions.
Colonoscopy procedures performed as emergency cases out-of-hours may also have a lower CIR. 19 We did not have access to data on how many of the symptomatic patients were emergency cases and/or scoped out-of-hours, but only four of the five colonoscopists that undertake BSP at our institution are also involved in emergency colonoscopy; both of the colonoscopists with low CIRs in symptomatic patients were in this category.
Finally, we were not able to take into account the complexity of the case-mix and performance of therapeutic procedures, such as stricture dilatation or insertion of a stent, which may have resulted in a decision not to perform a full colonoscopy.
In summary, we have demonstrated that the CIR, a key quality performance indicator for colonoscopy, is lower in symptomatic patients as compared to patients undergoing bowel cancer screening, confirming results from previous studies. The reason for the lower CIR is likely multi-factorial, reflecting a different case-mix and possibly the more stringent approach taken to the performance of colonoscopy in screening patients. We also demonstrated that there may be variation in individual colonoscopists’ performance, as assessed by the CIR, between symptomatic patients and individuals undergoing screening for colorectal cancer. These results suggested that in addition to monitoring overall CIR as a performance indicator, it is important to also look at CIRs separately in two groups: as screening procedures and those performed in symptomatic patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Acknowledgements
The authors gratefully acknowledge the co-operation of the BSP colonoscopists at our institution for permission to review their individual performance data.