
Abstract
Background
The quality of colonoscopy has been related to a higher risk of interval cancer, and this issue has been addressed extensively in developed countries. The aim of our study was to explore the main quality indicators of colonoscopy in a large emerging country.
Methods
Consecutive patients referred for colonoscopy in 14 centres were prospectively included between July and October 2014. Before colonoscopy, several clinical and demographic variables were collected. Main quality indicators (i.e. caecal intubation rate, (advanced) adenoma detection rate, rate of adequate cleansing and sedation) were collected. Data were analysed at per patient and per centre level (only for those with at least 100 cases). Factors associated with caecal intubation rate and adenoma detection rate were explored at multivariate analysis.
Results
A total of 8829 (males: 35%; mean age: 57 + 14 years) patients were included, with 11 centres enrolling at least 100 patients. Screening (including non-alarm symptoms) accounted for 59% (5188/8829) of the indications. Sedation and split preparation were used in 26% (2294/8829) and 25% (2187/8829) of the patients. Caecal intubation was achieved in 7616 patients (86%), and it was ≥85% in 8/11 (73%) centres. Adenoma detection rate was 18% (1550/8829), and it was higher than 20% in five (45%) centres, whilst it was lower than 10% in four (33%) centres. At multivariate analysis, age (OR: 1.020, 95% CI: 1.015–1.024), male sex (OR: 1.2, 95% CI: 1.1–1.3), alarm symptoms (OR: 1.8, 95% CI: 1.7–2), split preparation (OR: 1.4, 95% CI: 1.2–1.6), caecal intubation rate (OR: 1.6, 95% CI: 1.3–1.9) and withdrawal time measurement (OR: 1.2, 95% CI: 1.6–2.1) were predictors of a higher adenoma detection rate, while adequate preparation (OR: 3.4: 95% CI: 2.9–3.9) and sedation (OR: 1.3; 95% CI: 1.1–1.6) were the strongest predictors of caecal intubation rate.
Conclusions
According to our study, there is a substantial intercentre variability in the main quality indicators. Overall, the caecal intubation rate appears to be acceptable in most centres, whilst the overall level of adenoma detection appears low, with less than half of the centres being higher than 20%. Educational and quality assurance programs, including higher rates of sedation and split regimen of preparation, may be necessary to increase the key quality indicators.
Introduction
Cancer burden is quickly increasing in emerging countries, due to ageing of the population, adoption of Westernised lifestyles (e.g. changes in diet and decreased physical activity), and low socioeconomic status. 1 In Russia, cancer is the second most common cause of death, and colorectal cancer (CRC) represents the second most common cancer in women and the third in men, with an overall incidence of 30 cases per 100,000 people.1,2
At present, no organised CRC screening program is present in Russia, the only means of prevention being primary screening/early diagnosis with colonoscopy. 1 This is similar to what occurs in several Western countries, such as the United States (US) or Austria.3,4 Despite the fact that the availability of endoscopy in Russia is unknown, anecdotal evidence suggests there is no shortage of medical technology in Russia. 1
Quality of colonoscopy has been strictly related to the risk of interval CRC.5,6 In large administrative cohort or case-control studies, the risk of interval cancer – including its proximal localisation – appeared to be independently predicted by a relatively low rate of polyp/adenoma detection, as well as by a suboptimal caecal intubation rate.7–11
A few studies addressed the nationwide level of the quality of colonoscopy. In early 2000, the quality of colonoscopy appeared suboptimal in the United Kingdom and Italy with caecal intubation and polyp detection rates lower than 80% and 18%, respectively.12,13 These data triggered educational campaigns that resulted in nationwide improvement of such indicators.14,15 The quality of colonoscopy in Russia – and more in general in emerging countries – has not been addressed yet.
The aim of our prospective, multicentre nationwide study was to measure the main quality indicators of colonoscopy, and the related variability, in Russia.
Methods
A prospective, multicentre study involving 14 endoscopy centres, selected by the Russian Society of Endoscopy in order to be representative of the different regions of the country, was performed between July and October 2014. According to the study protocol only centres performing more than 1000 colonoscopies per year were considered. Centres were equally distributed among academic hospitals, large non-academic tertiary referral centres and community hospitals. The largest number of centres are located in large or middle-size cities. No data came from hospitals located in rural areas. To minimise intercentre variability, only two endoscopists per centre with more than three years of experience and performing more than 250 colonoscopies per year were allowed to participate in the study. Data were collected through a dedicated Web-based case report form (CRF). Each centre at the time of the study kick-off received a user name and password to enter in its own area. Before starting patient enrolment and data collection, a brief online training session was required for the physicians participating in the study. On a monthly basis, two senior authors (AR and MK) with administrator passwords double-checked the CRFs and in cases of missing or unclear data sent official emails to the specific centre for case-by-case clarification and/or missing data. According to the protocol, all patients referred to the participating centres for routine colonoscopy to the selected endoscopists were prospectively enrolled. Patients were excluded only when referred for emergency colonoscopy. All patients gave written informed consent for colonoscopy. Data were collected uniformly according to a previously defined protocol. In detail, the following variables were systematically collected: Patient level. 1) demographic data (age, sex); 2) family history for CRC (only first degree); 3) clinical indication for colonoscopy: screening, surveillance for adenomatous polyps or CRC, alarm symptoms/signs (i.e. anaemia, rectal bleeding, positive faecal occult blood test), non-alarm symptoms (i.e. abdominal pain/discomfort, alteration of bowel habit, abdominal bloating), workup for inflammatory bowel disease (IBD). Colonoscopy level. 1) sedation (midazolam, pethidine, propofol, flumazenil, none); 2) caecal intubation; 3) documentation of the caecal intubation (photo, movie, none); 4) type, schedule (split/no split), and level of bowel preparation (excellent, good, discrete, poor); 5) measurement of withdrawal time (yes/no); 6) withdrawal time in the measured cases; 7) expert vs. trainee endoscopist; 8) detection of polyps/masses; 9) polypectomy; 10) adverse events. Pathology level. Lesions were classified according to the World Health Organisation. In detail, advanced adenoma was defined as any adenoma ≥10 mm or with high-grade dysplasia (HGD) or villous component. In the case of multiple lesions, patients were classified based on the most advanced case of neoplasia.
Statistical analysis
For the most relevant quality parameters, we calculated the mean and the standard deviation, as well as the intercentre median with interquartile ranges (IQRs). In order to have reliable estimates when exploring intercentre variability, only those centres that enrolled at least 100 patients were included. In order to identify possible predictors of the quality of colonoscopy, we selected the two main quality parameters, namely caecal intubation rate and adenoma detection rate. Stepwise multiple logistic regression analysis was used to identify significant predictor variables for the detection of polyps, neoplasia and advanced neoplasia. The prediction model was built using JMP 98.0, version 8.0 (SAS; Cary, NC, USA) for stepwise logistic regression analysis with an entry criteria of p < 0.05. The stepwise procedure added independent variables to the model one at a time. In the final model variables were removed if the retention criterion of p < 0.1 was not met. Odds ratio (OR) was used to express the association between study variables and the selected outcome.
Results
Study population
Clinical, endoscopic, and endoscopist characteristics of the study population, according to the most advanced lesion detected at univariate analysis
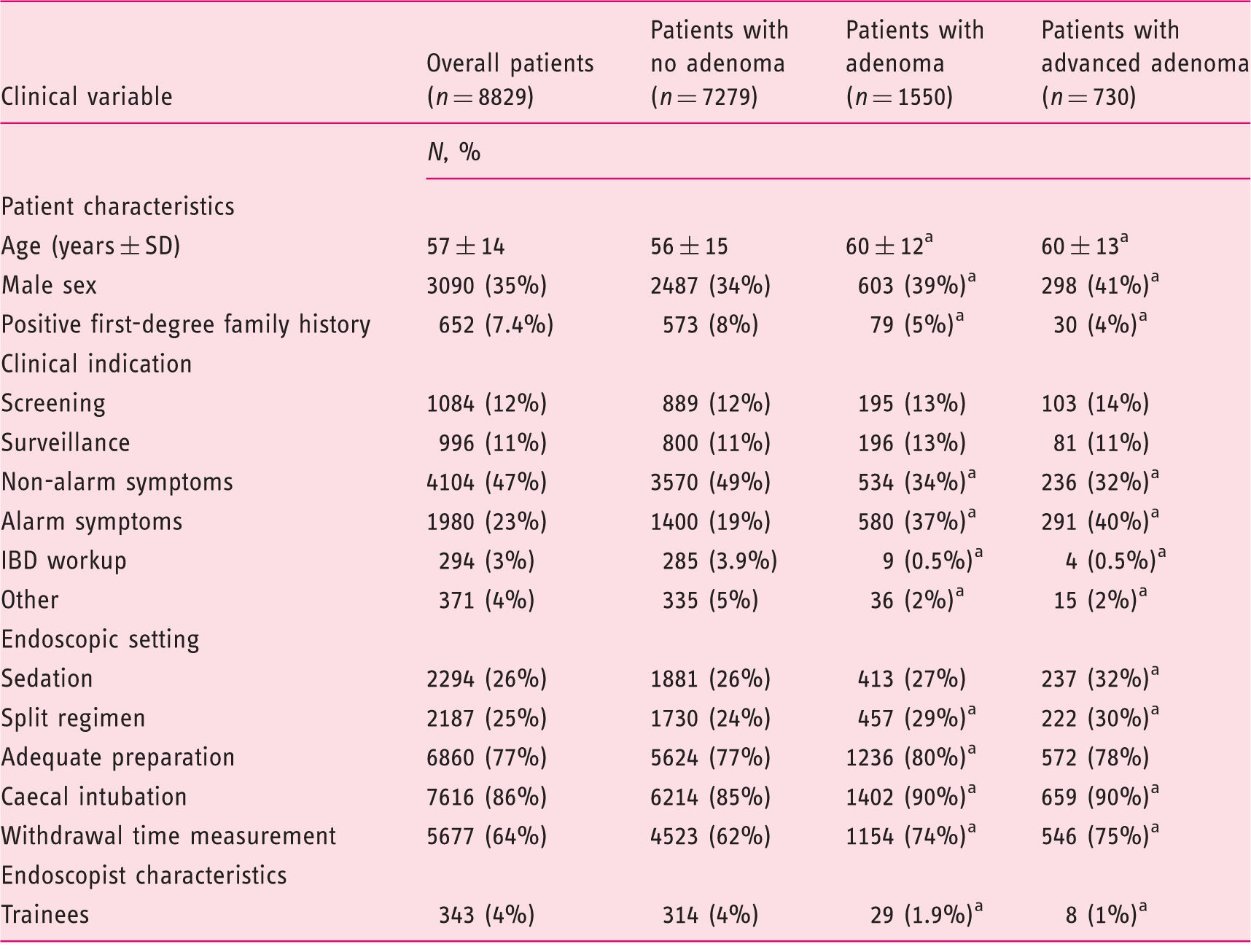
p < 0.05 as compared with patients with no adenoma. IBD: inflammatory bowel disease.
Main quality indicators of colonoscopy in the 11 centres with ≥100 colonoscopies
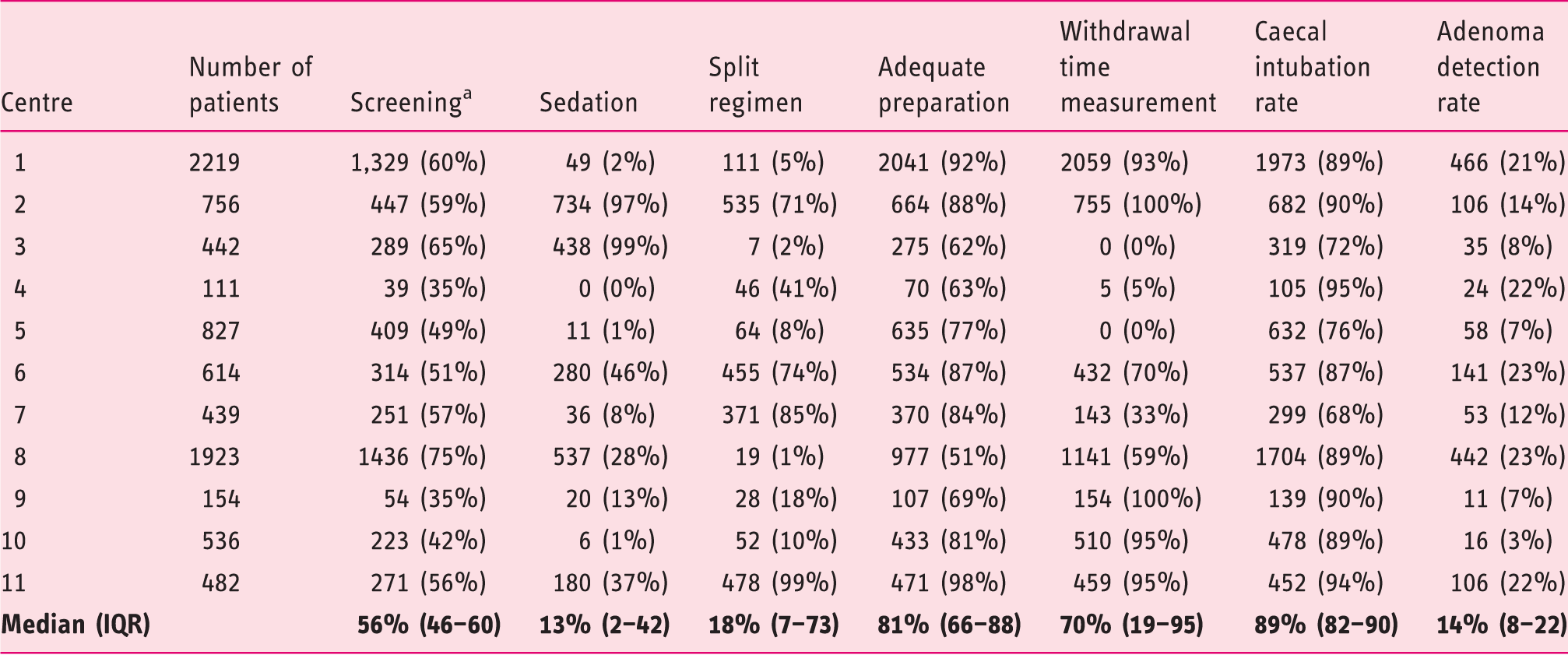
Including patients with non-alarm symptoms. IQR: interquartile range.
A positive family history was present in 652 (7.4%) patients. Clinical indication for colonoscopy was an alarm symptom or sign in 1980 (23%) patients, workup of IBD in 294 (3%), a non-alarm symptom in 4104 (47%), primary screening in 1084 (12%), and post-polypectomy/surgery surveillance in 996 (11%) patients, whilst it was another indication in the remaining 371 (4%) cases. As shown in Table 2, colonoscopy was performed for screening or in patients with only non-alarm symptoms in 5188 cases (59%), ranging from 35% to 75% in the 11 centres with at least 100 cases (median: 56%, IQR: 46%–60%).
Colonoscopy
Colonoscopy was performed with sedation in 2294 (26%) patients. The median of sedation rates among the 11 centres was 13% (IQR: 2%–42%), with only two (18%) centres using it systematically and five (42%) centres using it in less than 10% of the cases (Table 2). When sedation was used, it was with propofol in 1075 (47%), and with benzodiazepine and/or opioids in the remaining 1219 cases. A split regimen of preparation was adopted in 2187 (25%) patients, and an adequate level of preparation (i.e. good or excellent) was reported in 6860 (77%). It was a high-volume polyethylene glycol (PEG)-based preparation in 60% of the cases, a low-volume PEG in 31%, a magnesium citrate with sodium pico-sulphate in 6%, and others in 3% of the cases. The corresponding medians among the 11 centres were 18% (IQR: 7%–73%) and 81% (66%–81%). In detail, a split regimen was adopted in ≥50% in only four (36%) centres, whilst a <75% rate of adequate preparation was reported in four (36%) centres (Table 2).
Caecal intubation rate was achieved in 7616 (86%) cases, and the median among the centres was 89% (IQR: 82%–90%). The main reasons for incomplete colonoscopy were inadequate cleansing (450, 37%), pain (289, 24%), stricture (218, 18%), angulation (85, 7%), and others (171, 14%). As shown in Figure 1, it was ≥85% in eight (73%) centres, whilst it was lower in the remaining three centres.
Distribution of caecal intubation rates (CIR) for the centres with >100 enrolled cases. The vertical series (red font) indicates the progressive levels of CIR represented by the grey circles, and the black dots the CIR level of each centre. While eight centres reported a ≥85% adenoma detection rate (ADR), it was <85% in three centres.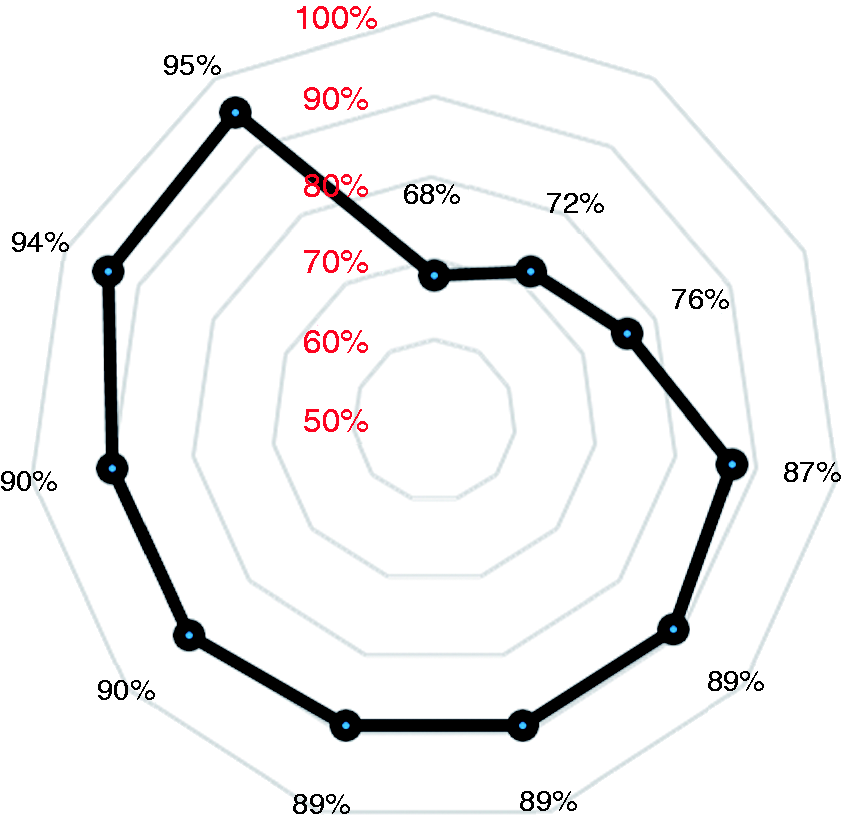
Withdrawal time was measured in 5677 (64%) cases (median in procedures without polypectomy: 10 ± 4 minutes), and it was reported in <5% of the cases in two (18%) out of the 11 centres (Table 2). Overall, 343 (4%) colonoscopies were performed by trainees (Table 2).
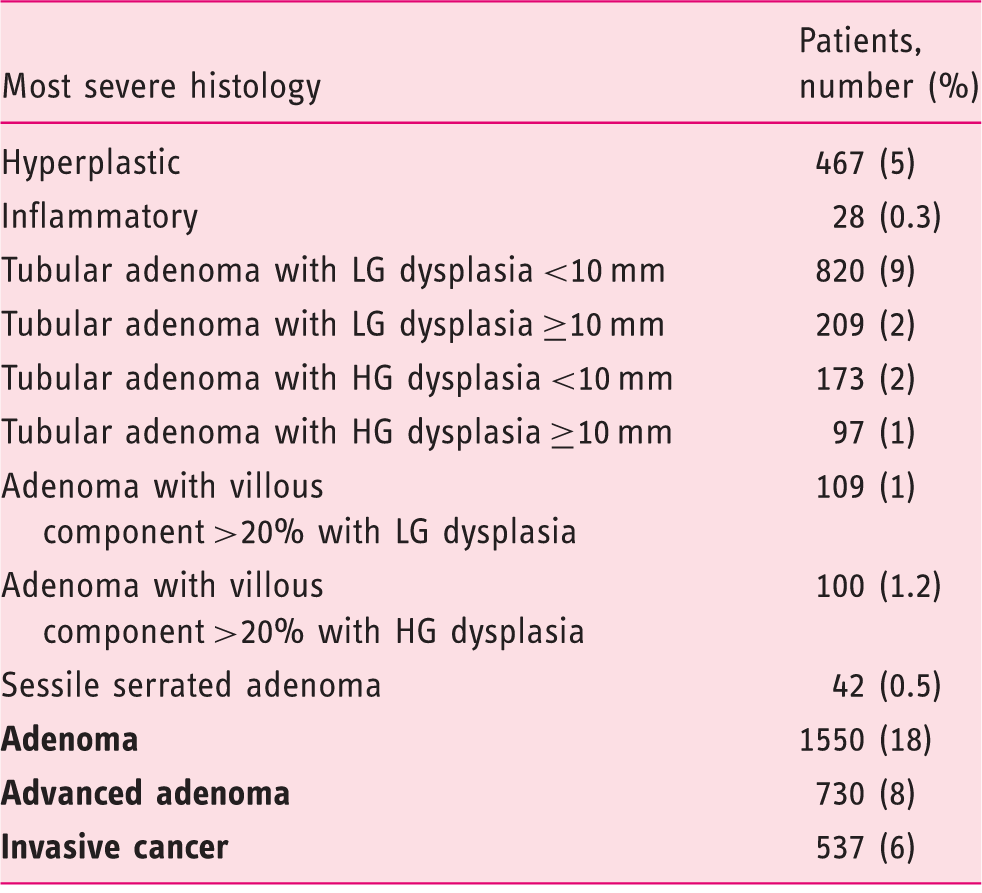
At colonoscopy, 2045 (23%), 1550 (18%) and 730 (8%) patients presented with polyp(s), adenoma(s) and advanced adenoma(s) as the most advanced lesion, respectively. Histological diagnoses are detailed in Table 3. The median of adenoma detection rates among the 11 centres was 14% (IQR: 8%–22%). As shown in Figure 2, it was higher than 20% in five (45%) centres, whilst it was lower than 10% in four (33%) centres. In addition, 537 patients presented with an already invasive cancer (6%). The location of adenomatous polyps was in the distal colon in 67% (1033 patients) of the cases, and in the proximal in the remaining 33% (517 patients). Regarding polyp morphology, it was polypoid in 83% (1286 patients) of the cases, and non-polypoid in the remaining 17% (264 patients) cases.
Distribution of adenoma detection rates (ADR) for the centres with ≥100 enrolled cases. The vertical series (red font) indicates the progressive levels of ADR represented by the grey circles, and the black dots the ADR level of each centre. While five centres reported a ≥20% ADR, it was <10% in four centres. Histological classification of the lesions detected in the study Per patient analysis according to the most severe histology. LG: low-grade; HG: high-grade.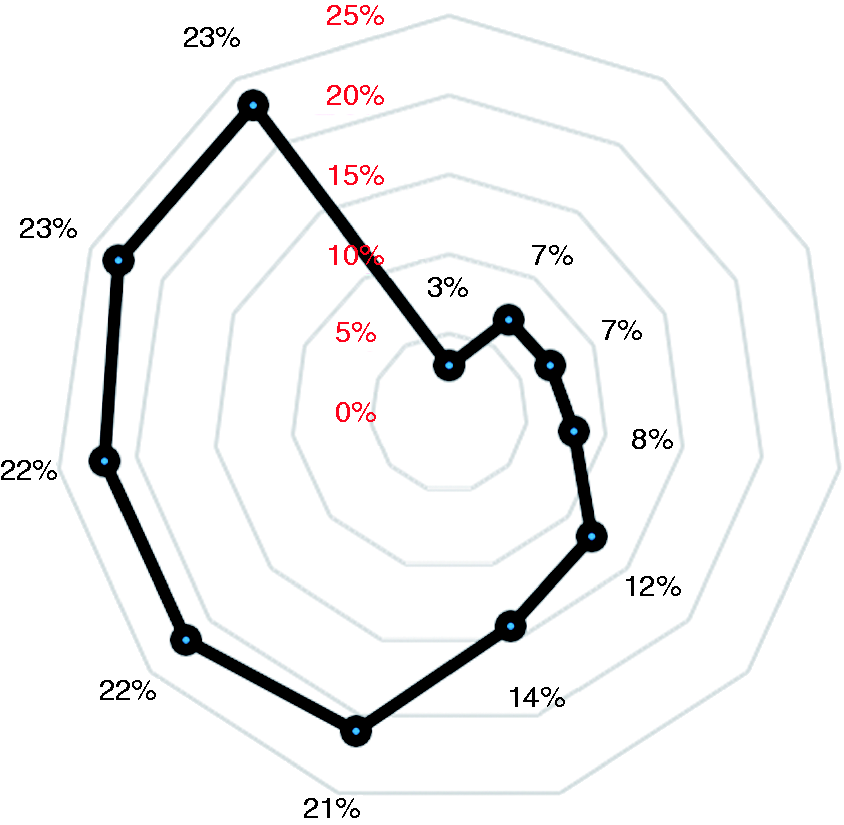
Multivariate analysis
Multivariate analysis for (a) the detection of polyps and neoplastic lesions, as well as for (b) caecal intubation rate
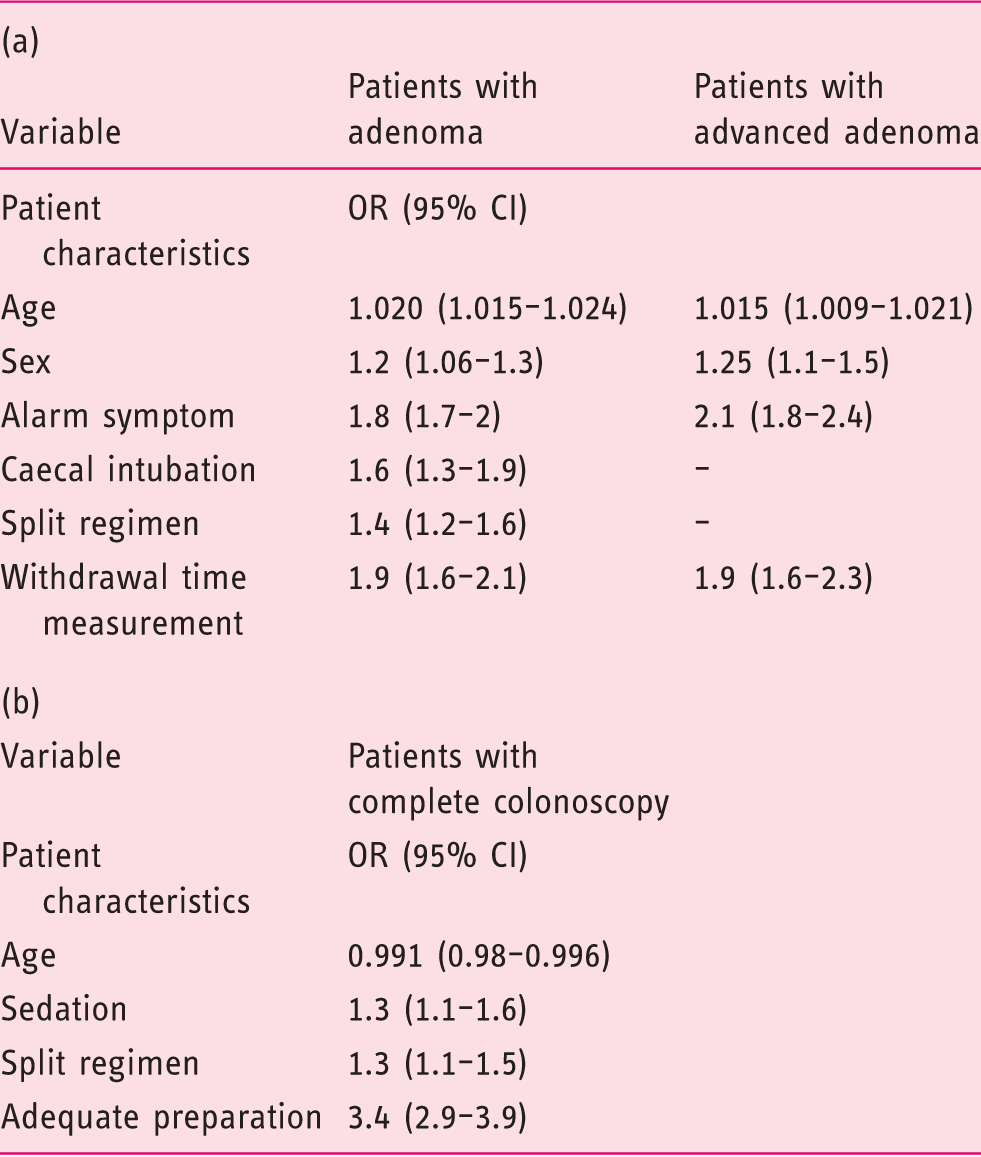
OR: odds ratio; CI: confidence interval.
Discussion
Main quality indicators in previous European series
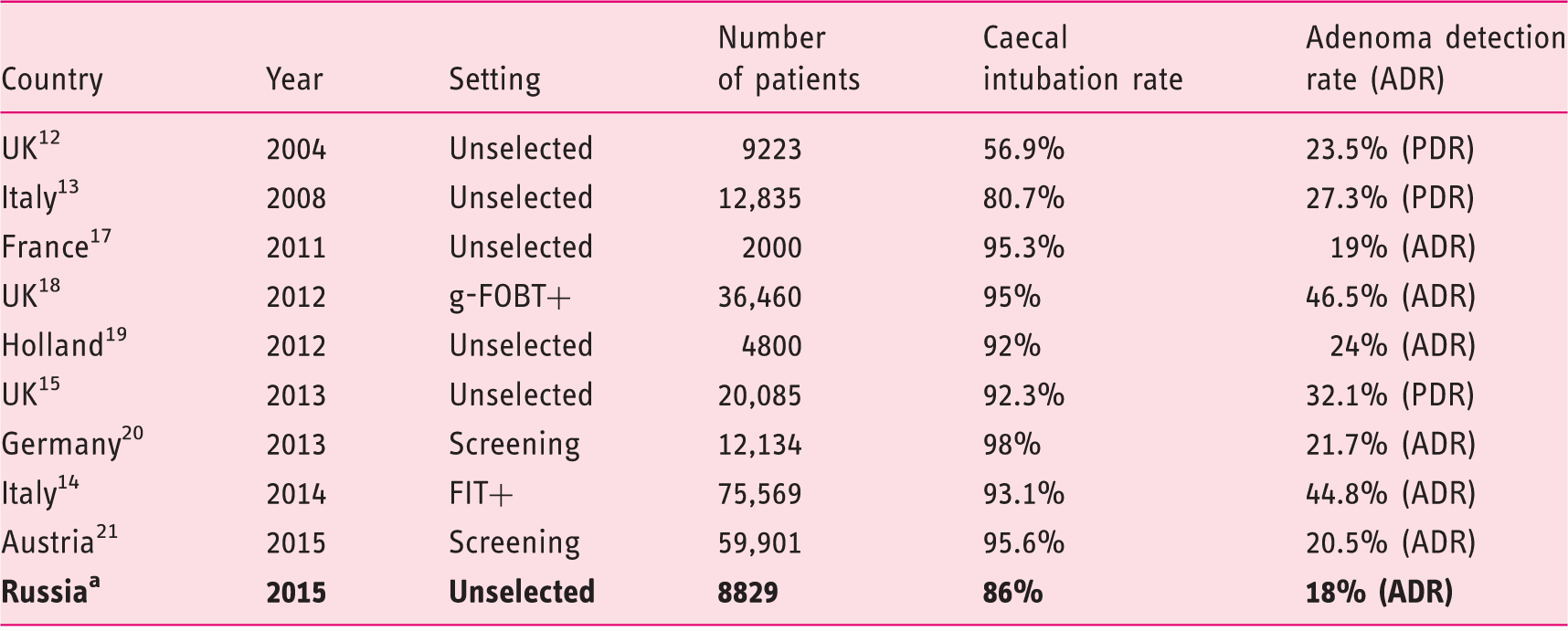
Present study. UK: United Kingdom; gFOBT: guaiac faecal occult blood test. FIT+: positive immunochemical faecal occult blood test; PDR: polyp detection rate.
Thus, educational campaigns may be rationalised by addressing only the minority of centres with poor performance. Such campaigns are urgent when considering the strict association between a suboptimal intubation rate and the risk of post-colonoscopy interval cancer.7,9,10 The 18% adenoma detection rate is not dissimilar from the 19%–24% recently shown in a European audit, whilst the substantial difference with the ≥40% adenoma detection rate shown in CRC screening programs with faecal test is simply related to the disease-enriched setting related to the specificity of guaiac-based or immunochemical-faecal test. However, this 18% average adenoma detection rate is still lower than the 25% benchmark recently recommended by an American guideline. 16 Of note, only a minority of patients – i.e. 23% – came for screening or surveillance, so the over-representation of symptomatic patients should have inflated the neoplastic detection rate at the per patient level. Similarly to the previous indicator, our audit allowed us to identify a small subset of centres with very poor performance, the adenoma detection rate being less than 10%. Only one of the three centres with a poor adenoma detection rate simultaneously had a poor caecal intubation rate, underlining the importance of simultaneously assessing both indicators. It has recently been shown that relatively short and convenient educational initiatives – such as retraining or train-the-trainer courses – may result into a substantial and stable improvement in the adenoma detection rate.17–19 Moreover, a progressive improvement in performance has recently been shown in Germany following the implementation of a strict QA program. 25 However, it could be argued that the 18% adenoma detection rate may simply be related to an intrinsically lower disease prevalence in the Russian as compared with the European populations, especially when considering that only a minority of the endoscopic population was male However, this is unlikely for two reasons. First, the 8% prevalence of advanced neoplasia is equal or substantially higher than that detected in European surveys in unselected or screening cohorts.21–24 Secondly, five out of the 11 centres presented with a ≥20% adenoma detection rate that is in line with the recent European data, indicating that factors other than disease prevalence may explain the suboptimal performance of the remaining centres.
We also assessed possible predictive factors for neoplasia and advanced neoplasia in this large Russian cohort. We confirmed the strict association between age and male sex, on one side, and the detection of both adenoma and advanced adenoma at per patient level, on the other, in agreement with previous large cohorts.14,25,26 This may be informative when planning an organised screening program, in order to identify the target population. We also showed a strict association between a split regimen of preparation and both the detection of neoplasia and the caecal intubation rate, underlining the importance of an adequate bowel preparation for the quality of colonoscopy. When considering that a split regimen was actually adopted for only 25% of the study cohort, a relatively simple and effective intervention could be based on the widespread implementation of split regimen in Russian endoscopic centres. Of note, a split regimen is nowadays recommended by official guidelines for all the procedures, irrespectively of the timing.27,28 Secondly, sedation was associated with a higher caecal intubation rate, in agreement with previous studies. 14 However, sedation was limited to one-quarter of the study cohort, and it was based on propofol in nearly half of the cases. Thus, implementation of more endoscopist-oriented conscious sedation protocols – such as the combination of benzodiazepine and opioid drugs – should be performed at least in those centres with a suboptimal caecal intubation rate.
There are limitations in the present analysis. We decided not to base our study in a screening setting, in order to increase the generalisability of our data. However, the wide range of variability observed was similar to that described in screening series,11,14,15,24 indicating that non-patient-related factors are dominant in explaining such variability. Secondly, we could not exclude that a so-called Hawthorne effect 29 – i.e. the endoscopist could have been influenced in his or her performance by the awareness of participating in a dedicated study – could have improved the detection rate of the individual endoscopists. Therefore, we cannot exclude the intercentre variability in the daily routine to be even worse than that reported in our series. Thirdly, the poor inter-observer agreement in the pathological diagnosis of HGD or villous component could have affected the reliability of our analysis for the factors associated with advanced neoplasia. 30 However, the evidence that most of the factors associated with advanced neoplasia were also associated with the simple diagnosis of neoplasia would minimise such a diagnostic bias.
According to our study, there is substantial intercentre variability in the main quality indicators. Educational and QA programs, including higher rates of sedation and split regimen of preparation, may be necessary to increase the suboptimal levels of key quality indicators.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.