
Abstract
Stapedial fixation coupled with incomplete partition type 2 and enlarged vestibular aqueduct (EVAS) represents a unique challenge in managing hearing loss owing to the risks of stapedial surgery and the need for alternative hearing restoration methods. This case report describes the selection, implementation, and outcomes of an Osia-2 implantable bone conduction device in a 17-year-old male patient with severe bilateral mixed hearing loss. Seventeen-year-old male patient with severe to profound bilateral mixed hearing loss due to incomplete partition type 2 and EVAS in the presence of audiolotical findings of stapedial fixation. His bone thresholds pure tone average of 40 dB hearing level and an air thresholds PTA of 70 dB hearing level. A nonsurgical bone conduction hearing assistive device demonstrated improved sound performance and high patient satisfaction. Subsequently, an OSI200 implant was used. A posteroinferior incision was created with the BI300 carefully placed 6.5 cm from the external auditory canal. The postoperative outcomes were remarkable, suggesting air-bone gap over-closure with an Osia-aided PTA of 31.67 dB hearing level and an aided speech discrimination score of 96%. Notably, the unaided bone conduction hearing remained unchanged, underscoring the efficacy of the implant in enhancing auditory function without compromising residual hearing. The patient maintained stable hearing levels up to 18 months, confirming the durability of hearing preservation and gain. This case underscores the efficacy of the OSI200 device in managing severe mixed hearing loss in patients with inner ear anomalies, such as incomplete partition type 2 and EVAS. The smooth soft drilling needed for the BI300 implant, and posterior placement, thus improving hearing without altering the unaided bone conduction thresholds.
Introduction
In pediatric otolaryngology, the management of hearing loss caused by congenital anomalies presents multifaceted challenges. 1 Of these, congenital stapedial fixation along with inner ear malformations, such as incomplete partition type 2 (IP-2) and enlarged vestibular aqueduct (EVAS), represent a complex clinical scenario. These conditions not only contribute to a mixed hearing loss phenotype but also restrict the applicability of conventional surgical interventions, such as stapedectomy, because of the increased risk of inner ear damage and subsequent sensorineural hearing loss (SNHL).2,3 Thus, alternative hearing rehabilitation strategies, particularly bone conduction devices, have emerged as crucial tools for restoring auditory function while minimizing the risk of residual hearing.
Incomplete partition type 2, a subtype of the cochlear malformation spectrum, is characterized by the triad of enlarged vestibular aqueducts, common cavities, and shortened modiolus. 2 When combined with congenital stapedial fixation, it predisposes individuals to conductive hearing loss and increases the risk of progressive SNHL. 4 Enlarged vestibular aqueduct syndrome (EVAS), which can occur in isolation or as a syndromic entity, complicates auditory rehabilitation by increasing the vulnerability of the inner ear to trauma and fluctuating pressure changes. 5
Researchers have demonstrated the safety, efficacy, and patient satisfaction of bone conduction devices, highlighting its potential as a treatment option for patients with conductive or mixed hearing loss. 6 Unlike traditional percutaneous implants, the Osia-2 system utilizes a piezoelectric transducer that can be implanted under the skin. 7 This in turn reduces the risk of skin complications and provides a more aesthetically pleasing solution. Additionally, the BI300 design facilitates minimal drilling, which is beneficial for patients with inner ear anomalies to avoid the risk of hearing deterioration. 8
Despite its promising features, limited literature have documented the use of the Osia-2 system in patients with complex otologic conditions, such as IP-2 and EVAS. This gap warrants detailed case reports and clinical studies examining the outcomes of Osia-2 implantation in this patient population. Understanding the nuances of surgical techniques, postoperative hearing outcomes, and long-term stability of hearing thresholds can provide valuable insights into optimizing care for patients with similar anatomical challenges.
This case report describes Osia-2 implantation in a 17-year-old male with severe-to-profound bilateral mixed hearing loss resulting from stapedial fixation, IP-2, and EVAS. It focuses on the preoperative considerations, surgical approaches, and postoperative auditory outcomes to elucidate the potential of the Osia-2 system in managing hearing loss and to guide in the multidisciplinary management of such patients.
Case report
Written and informed consent from the patient and his family was obtained. This case report was exempt from full review by the institutional ethics review board.
A 17-year-old boy was referred to our institution for hearing loss. The patient had a family history of hearing loss and his sister had received a cochlear implant. The patient used conventional bilateral hearing aids; however, he did not experience the expected benefit. He had no other comorbidities. Physical examination suggested no dysmorphic features. Results of the otological examination (otoscopy) were normal. Audiometric testing suggested bilateral severe to profound mixed hearing loss with air pure tone average of 70 dB hearing level (HL) and bone pure tone average of 40 dB HL as well as a Carhart notch (Figure 1). His tympanometry revealed type “As” bilaterally with speech discrimination score (SDS) for monosyllabic words was 46%. His aided PTA was 55 dB and aided SDS was 70%. Computed tomography suggested bilateral IP-2 with EVAS. Whole exome sequencing suggested no genetic mutations. Based on the radiological and audiometric results, the patient was suspected to have stapedial fixation in the presence of IP-2 and EVAS (Figure 2).

The preoperative audiometry of the patient showing bilateral mixed hearing loss with Carhart notch representing stapedial fixation.
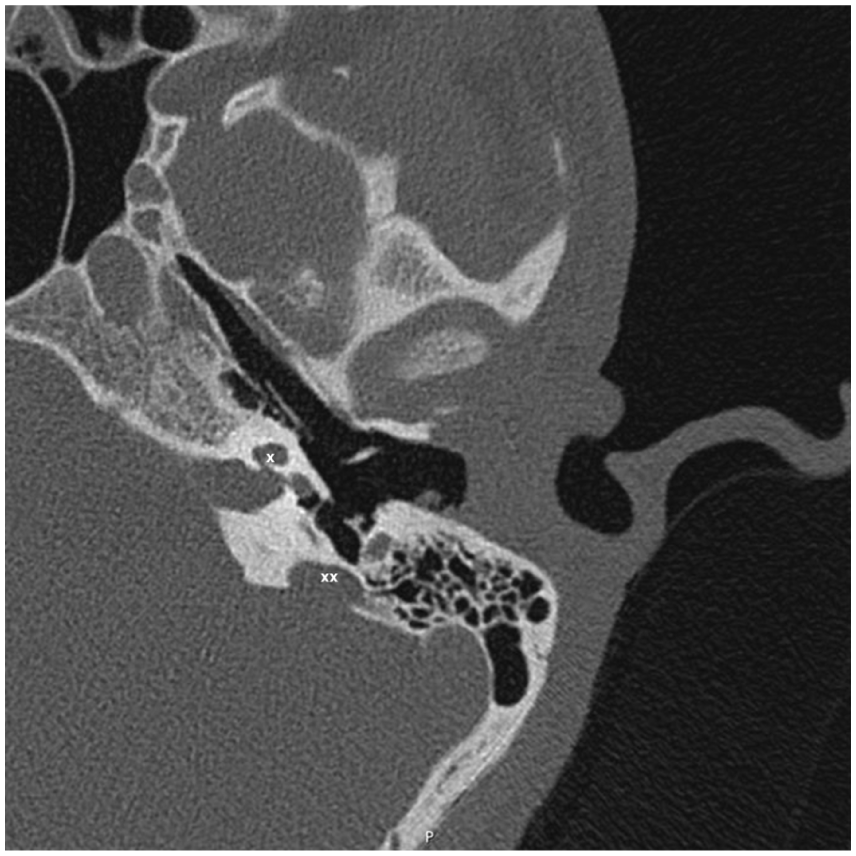
An axial view CT scan of the left inner ear highlighting incomplete partition type 2 (marked by “x”) and enlarged vestibular aqueduct (marked by “xx”).
The patient and his family were counseled on the options available to improve hearing. Stapes/ossicular chain surgery was not recommended because of IP-2 and EVAS, which poses a high risk of gusher and permanent hearing loss. A trial of a nonsurgical bone conduction device (BAHA SoftBand, Cochlear Ltd., Sydney, Australia) yielded an aided-PTA of 45 dB HL and SDS of 86%. A vestibular assessment was performed preoperatively using a video-nystagmography (VNG); it demonstrated decreased response on the left ear upon optokinetic, normal positional, and Dix Hallpike tests. Caloric test suggested complete areflexia on the left side and decreased response on the right. A multidisciplinary meeting was conducted with the family and patient, in which various hearing solution options, including surgical and nonsurgical bone conduction solutions, were discussed. They understood the risk of permanent hearing loss with minor head trauma in patients with EVAS or IP-2. Furthermore, the patient and his family were counseled on the possibility of future deterioration of his hearing given that he has EVAS and IP-2 which may limit the benefit from any bone conduction device and may require cochlear implantation. The patient and family wanted a better hearing solution while understanding the risk. Thus, an active piezoelectric stimulation device that relies on a BI300 implant represented a potentially safer and less traumatic option among other implantable bone conduction devices. Additionally, we decided to proceed with the left ear because it had worse hearing.
Surgery
First, a detailed written informed consent was obtained from the family and the patient. Then surgical planning was initiated under general anesthesia, with orotracheal intubation and routine precautions. We utilized the posteroinferior approach. 9 The skin was marked at the following locations: site of the BI300 (6.5 cm from the external auditory canal) with methylene blue, position of the device, and posteroinferior incision (1.5 cm away from the device edges; Figure 3). Prepping and draping were performed routinely. An incision was created and deepened through the subcutaneous layers and muscles until the periosteum was reached. Methylene blue staining of the BI300 site was identified. The periosteum was excised. The drill speed was set to 2000 RPM. The site was gently drilled to a bone depth of 4 mm, with copious amounts of irrigation. The adequate thickness was determined based on the on the size of drill head used which is capable of drilling down to 4 mm. A countersink drill was used at an identical speed. Subsequently, the BI300 was implanted into the drilled site at 35 RPM. The OSI200 device was fixed over the BI300. The subcutaneous tissue and skin were sutured, and a compressive dressing was applied (Figure 4).
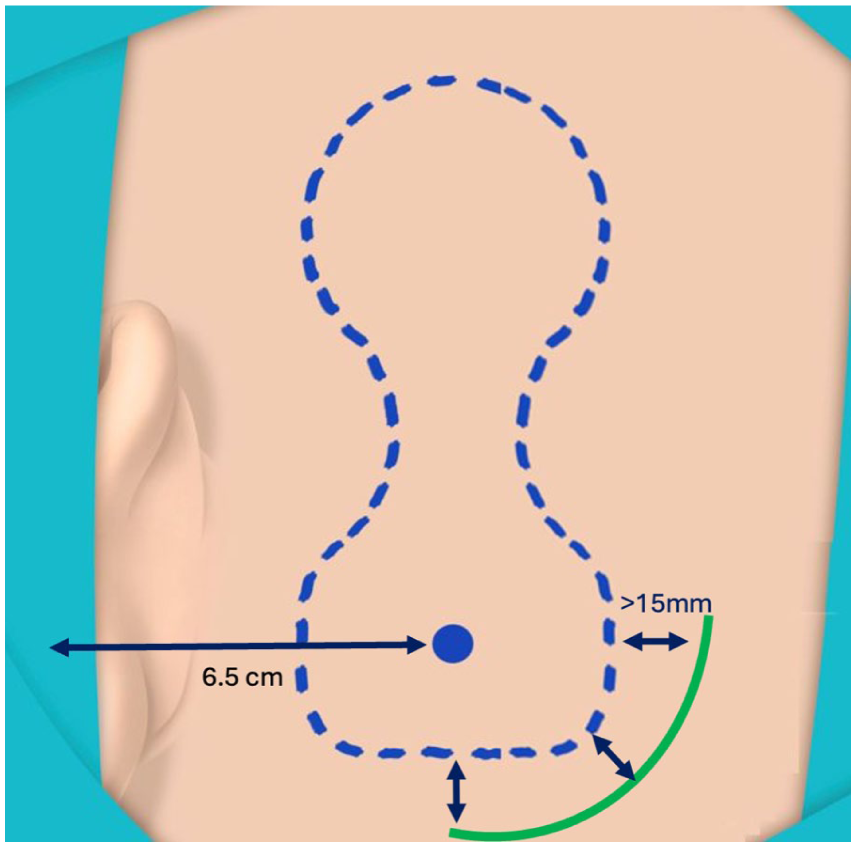
This diagram describe the posteroinferior approach that was utilized in this case. The incision was 1.5 cm away from the edges of the device to reduce the possibility of device exposure in the unlikely event of wound dehiscence or infection.

The OSI200 device implanted in the patient just before closure of the wound.
Postoperative course
The wound healed 3 weeks after the surgery. The patient was fitted with a sound processor, and programming and rehabilitation sessions were initiated. Three months after surgery, his Osia-aided PTA was 31.67 dB HL, with overclosure of the air-bone gap and an SDS of 96% (Figure 5). While writing this report 18 months after surgery, the patient demonstrated stable hearing in both ears. Furthermore, VNG and calorimetry were performed 6 and 18 months after the surgery, and it did not suggest any changes. The patient reported to be very satisfied with the implant and sound processor and wears it regularly and daily.
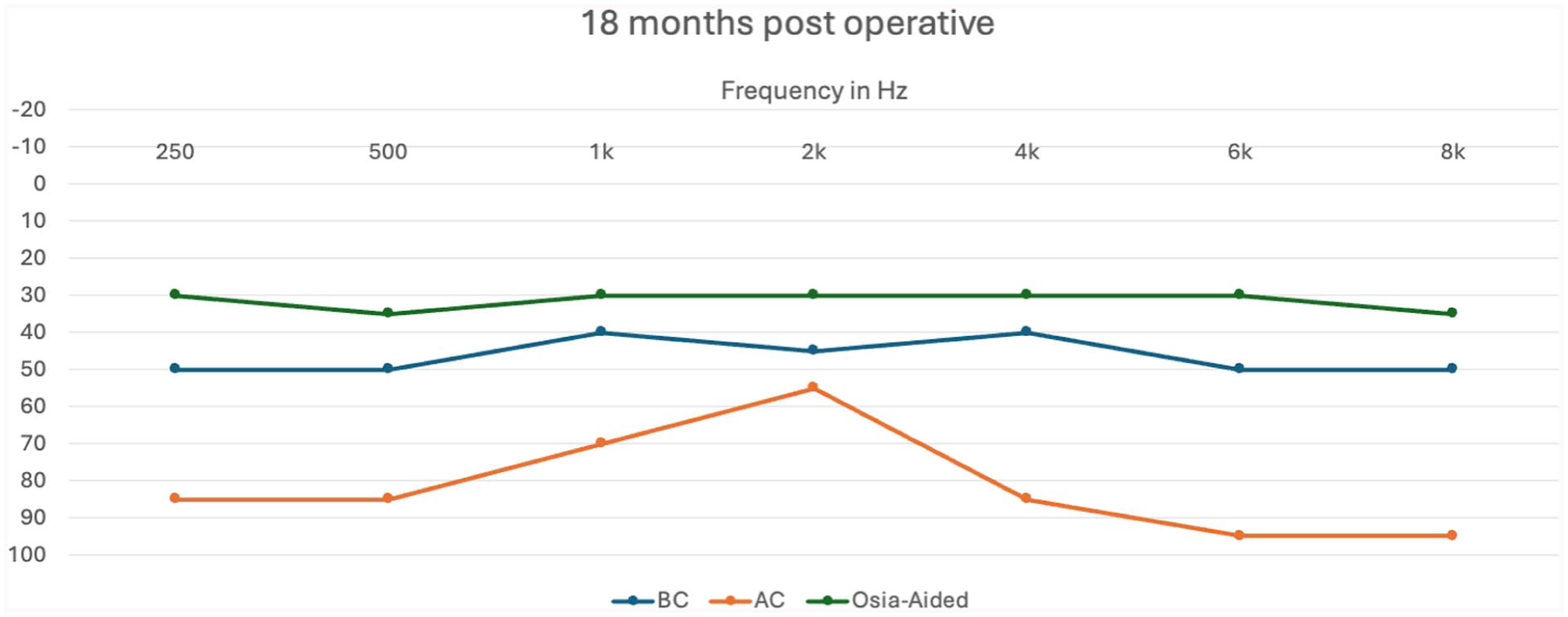
The audiogram of the patient 18 months postoperatively as well as the Osia-aided thresholds. It demonstrates over correction of the air-bone gap. The hearing thresholds remained stable throughout the 18 months postoperatively.
Discussion
The management of hearing loss in patients with congenital anomalies, such as IP-2 and EVAS poses significant challenges. The complexities of these conditions necessitate a multidisciplinary approach to select the most appropriate auditory rehabilitation strategy. A 17-year-old boy with these conditions was managed successfully with an OSI200 implantable bone conduction device. This case provides valuable insights into the nuances of treatment selection and outcomes in complex scenarios.
Several factors influenced the decision to select an OSI200 device over other active bone-conduction implants or surgical interventions, such as stapedotomy. First, the unique anatomical considerations in the patient, including the risk of SNHL after invasive surgery, necessitated a careful approach. The BI300 implant in the Osia-2 system, with its minimal drilling requirement, was a potentially safer alternative for auditory preservation.8,10
In the context of managing mixed hearing loss, bone conduction devices play a critical role, particularly when traditional surgical interventions pose significant risks or have limited efficacy. Karimi Yazdi et al. 11 explored the impact of different surgical techniques on bone conduction improvement in otosclerotic patients with mixed hearing loss, offering valuable comparative insights on stapedectomy and stapedotomy procedures. Their findings revealed that a significant proportion of patients (75%) experienced an improvement in bone conduction thresholds postsurgery, with partial stapedectomy yielding the most favorable outcomes in terms of bone conduction gains. 11 This suggests that while direct surgical interventions on the stapes can be beneficial in specific contexts, they carry inherent risks and variable success rates, especially over extended periods.
Stapes gusher, which occurs when there is an abnormal communication between the perilymphatic space and the subarachnoid space, leading to a sudden and profuse outflow of cerebrospinal fluid into the middle ear and external auditory canal upon the opening of the vestibule. 12 This condition, although rare with a reported incidence of approximately 0.3%, poses considerable challenges in the management of otosclerosis and other middle ear pathologies requiring stapes surgery. Alicandri-Ciufelli et al., 12 highlighted several critical aspects of managing a gusher during stapes surgery. Most commonly, it involves immediate steps to seal the oval window and fill the tympanic cavity with absorbable and autologous graft materials to control the leakage. Despite these measures, the presence of a gusher can lead to severe complications, including complete or profound hearing loss in about 25% of cases and a worsening of hearing function in 31% of the cases. 12 These outcomes necessitate a cautious approach when considering stapes surgery in patients at risk for this complication.
Comparatively, the case reported in the current manuscript utilizes the OSI200, an implantable bone conduction device, which presents a less-invasive alternative with stable, long-term benefits in auditory outcomes. The patient demonstrated a consistent improvement in both pure tone average and SDS, with no adverse changes in unaided hearing thresholds over 18 months follow-up period. This underscores the utility of the Osia-2 system in providing substantial auditory rehabilitation without the surgical risks associated with manipulating the stapes in patients with complex otological conditions like IP-2 and EVAS. Such a strategy is particularly pertinent in cases where traditional surgery poses a high risk of SNHL or other complications, highlighting the role of bone conduction devices as a safe and effective alternative for managing mixed hearing loss.
This case emphasizes the importance of patient and family involvement in the decision-making process, particularly upon weighing the potential risks and benefits of surgery. Shared decision-making practices are essential in pediatric otology to ensure that the selected interventions align with the expectations and goals of the patient and family.8,13
In conclusion, this report not only highlighted the successful application of the Osia-2 implantable bone conduction device in case of congenital hearing loss but also reinforced the importance of a comprehensive, patient-centered approach in managing pediatric hearing loss. The BI300 Osia system low-speed and smooth drilling, coupled with the posterior placement approach, thus improving hearing without altering the unaided bone conduction thresholds.
Footnotes
Authors’ note
This report was presented in the third Arabic cochlear Implant Conference in Abu Dhabi (October 2024).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.