
Abstract
Aberrant right subclavian artery is one of the most common congenital anatomical variations of the aortic arch, but its occlusion is extremely rare. Although femoral artery access for endovascular treatment has become the mainstream approach for subclavian artery stenosis or occlusion, when the femoral artery approach fails to identify the arterial stump, the radial artery approach becomes an alternative. This report presents a case in which, after failure to treat via the femoral artery, a self-expanding stent was successfully deployed through the radial artery approach to treat a long segment occlusion of the aberrant right subclavian artery. The case involved a 71-year-old female patient who presented with a 3-month history of recurrent dizziness, right upper limb weakness, and episodic coldness in the right hand. Clinical and Duplex ultrasound findings confirmed subclavian steal syndrome secondary to aberrant right subclavian artery occlusion. The patient underwent successful stent implantation via the radial artery approach, and postoperatively, the symptoms resolved, and antegrade flow in the vertebral artery was restored. This case highlights the rare long-segment occlusion of the aberrant right subclavian artery and suggests that the radial artery approach may serve as a potential method for occlusion recanalization.
Keywords
Introduction
Aberrant right subclavian artery (ARSA) is a congenital anomaly of the aortic arch, with an incidence of ~1.0%–2.0%. 1 This variation is characterized by the right subclavian artery originating from the distal portion of the aortic arch, beyond the left subclavian artery branch (rather than from the usual origin at the brachiocephalic trunk), and typically crossing behind the esophagus to enter the right axillary artery. Clinically, it is referred to as “artery lusoria.” Studies have shown a significantly higher incidence of ARSA in patients with chromosomal abnormalities, such as trisomy 21, which may be related to abnormal vascular development during embryogenesis. 2 Most cases of ARSA are asymptomatic, but some patients may present with symptoms such as dysphagia and dyspnea due to anatomical compression. 3 In addition, the origin of ARSA is prone to aneurysm formation (Kommerell diverticulum) or dissection, with a higher risk of rupture. 4 When the aberrant artery is stenosed or occluded, patients may experience symptoms such as dizziness or upper limb ischemia due to vertebrobasilar insufficiency. In this article, we describe a case in which the femoral artery approach failed to locate the remnant stump of ARSA, and we successfully treated long-segment complete occlusion using a self-expanding stent via the radial artery approach.
Case report
As summarized in Table 1, symptom onset occurred 3 months prior. Diagnostic computed tomography angiography (CTA) confirmed ARSA occlusion, leading to an initial femoral access attempt on day 3. After failure due to an absent remnant stump (Figure 1(a)), radial access succeeded.
Timeline.
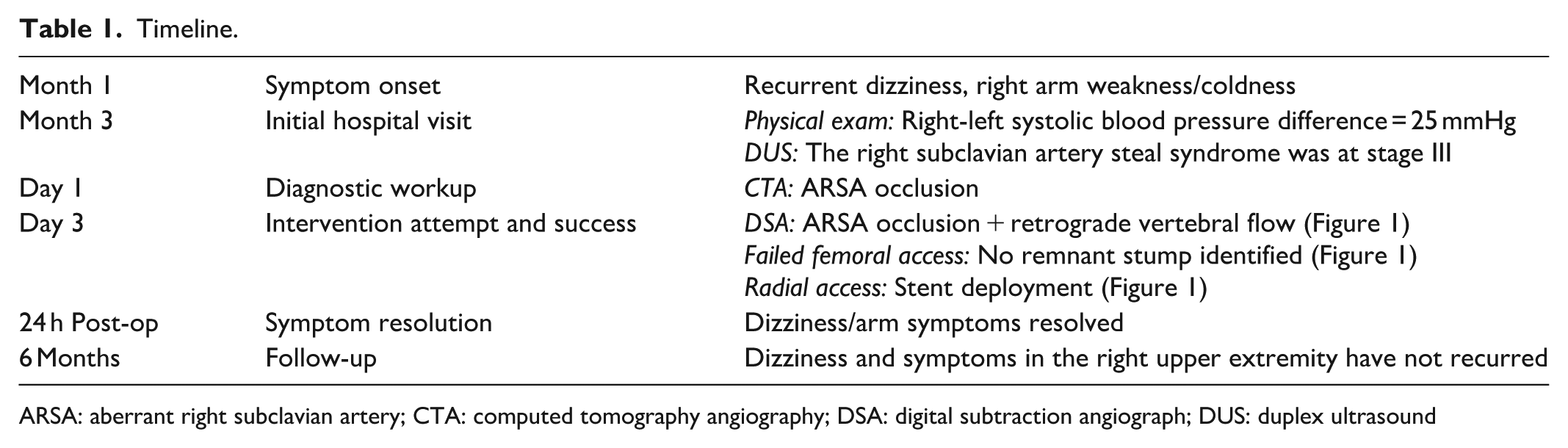
ARSA: aberrant right subclavian artery; CTA: computed tomography angiography; DSA: digital subtraction angiograph; DUS: duplex ultrasound

DSA demonstrated proximal occlusion of the ARSA (red box, a), with compensatory retrograde flow from the right vertebral artery (red arrows) at the distal segment (b). The roadmap (c). Hydrophilic-coated guidewire passed through the occluded segment (d). A balloon was advanced along the guidewire and gradually inflated, transforming from a dumbbell shape to a sausage shape (e). Immediate postoperative DSA indicated complete recanalization of the occluded segment of the ARSA, with restored antegrade flow in the right vertebral artery (f).
A woman in her early 70s presented with a 3-month history of recurrent dizziness triggered by right arm exertion, persistent right upper limb weakness, and intermittent cold sensation in the right hand, which has significantly affected her daily life. Physical examination revealed reduced right radial pulse amplitude and a systolic blood pressure difference of 25 mmHg between arms (right: 100 mmHg; left: 125 mmHg). She has no previous history of surgery, hypertension, diabetes, or smoking.
Upon admission, we measured the blood pressure in both upper limbs and found that the left upper limb systolic blood pressure was 40 mmHg higher than the right side. Duplex ultrasound revealed luminal stenosis in the proximal segment of the left internal carotid artery with a stenosis rate of 59%. The flow velocity at the origin of the left vertebral artery was increased, reaching 197 cm/s. The entire course of the right internal carotid artery showed multiple hyperechoic, isoechoic, and mixed-echo calcified plaques. The right vertebral artery presented retrograde flow signals throughout the cardiac cycle. The right subclavian artery steal syndrome was at stage III. CTA identified an ARSA arising as the fourth branch from the proximal descending aorta distal to the left subclavian artery, demonstrating a retroesophageal course. No Kommerell diverticulum was present at the origin of the occluded ARSA segment; the occlusion length is 35 mm, the vessel diameter is 8.87 mm, and no calcifications are observed (Figure 2). Echocardiographic examination revealed no abnormalities in intracardiac structure or cardiac function. The fasting blood glucose was 5.01 mmol/L, and the triglyceride level was 1.54 mmol/L. Given the presence of subclavian steal syndrome and the fact that the patient’s severe right upper extremity weakness significantly impaired daily work, we decided to perform percutaneous transluminal angioplasty with stent placement after fully informing the patient of the surgical risks and obtaining their consent. Stent sizing/length selection was deliberately chosen to ensure the proximal edge landed distal to the Vertebral artery (VA) origin (confirmed by pre-op CTA measurements), minimizing the risk of ostial coverage or plaque shift. The self-expanding Wallstent was favored for its lower radial force compared to balloon-expandable stents, reducing snowplow effect risk near the VA.
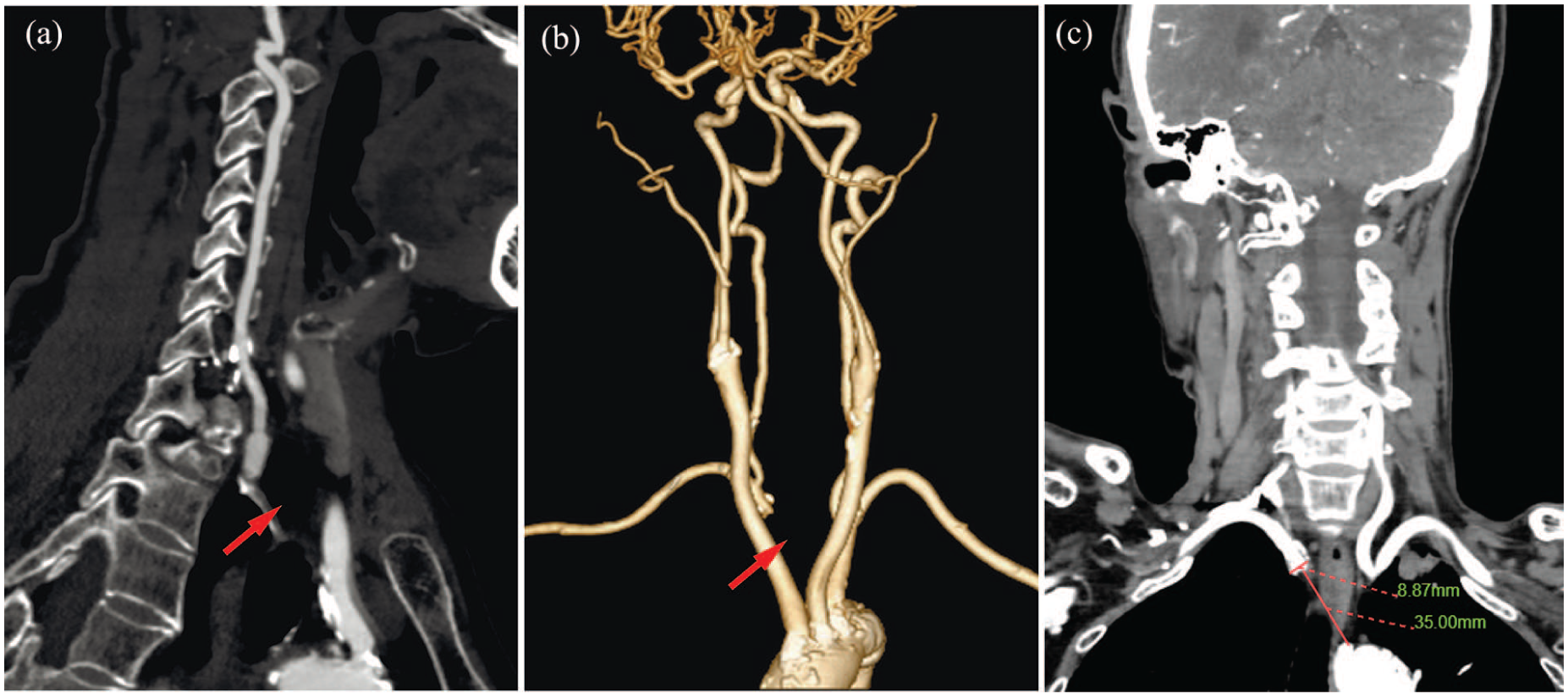
CTA revealed occlusion at the origin of the ARSA (red arrow), with no remnant stump of the ARSA observed in the aortic arch (a). Three-dimensional reconstruction images demonstrated that the right vertebral artery originated from the ARSA, with the proximal portion of the right subclavian artery not visualized (red arrow, b). Occlusion segment length and vessel diameter (c).
Initially, we approached via the right femoral artery, using the Seldinger technique, an 8F arterial sheath was inserted. Under the guidance of a 0.035-in hydrophilic guidewire, an angiographic catheter (Cordis, 5F, 125 cm; Johnson & Johnson, USA) was advanced to the aortic arch for cerebral angiography. Digital subtraction angiography (DSA) revealed occlusion at the origin of the right subclavian artery (Figure 1(a)), with no remnant stump of ARSA on the aortic arch and retrograde flow in the right vertebral artery (Figure 1(b)). After multiple unsuccessful attempts to locate the origin of ARSA using an 8F guiding catheter with a guidewire, we opted for the radial artery approach and replaced it with a 6F arterial sheath. After advancing the radial artery long sheath (Sino, 6F, 115 cm) into position using a hydrophilic-coated guidewire and a multi-purpose angiographic catheter (Cordis, 5F, 125 cm; Johnson), the hydrophilic-coated guidewire directly traversed the occluded segment without the need for guidewire exchange (Figure 1(c) and (d)). After advancing the balloon (Rx Viatrac 14 Plus, 6 × 30 mm; Abbott, USA), slow and repeated inflations were performed to balloon angioplasty the occluded segment (Figure 1(e)), and a 9 × 40 mm self-expandable Carotid Wallstent (Wallstent, Boston Scientific, USA) was successfully deployed. Subsequent DSA showed good visualization of the ARSA with restored antegrade flow in the right vertebral artery (Figure 1(f)). Postoperatively, the patient’s dizziness resolved. During the 6-month postoperative follow-up, the patient expressed profound gratitude for the relief of her symptoms. She described, “Before treatment, I completely avoided using my right arm because even simple actions like stirring a pot would trigger dizziness and weakness. Now I can do housework and carry groceries without fear.” She emphasized that the radial artery approach minimized perioperative discomfort (“only a small bandage on the wrist”) and allowed immediate mobility after surgery.
Discussion
Complete occlusion of the ARSA is extremely rare as a congenital variation of the aortic arch. The 2024 European Society of Cardiology guidelines state that subclavian artery ischemia is often asymptomatic. Some patients are diagnosed through further physical examination due to an upper arm blood pressure difference >10–15 mmHg. Dizziness and visual disturbances during upper limb exercise may indicate subclavian artery stenosis, and the presence of steal syndrome may lead to more typical symptoms. For patients with symptomatic subclavian artery ischemia, revascularization may be considered after thorough discussion with a vascular center (Class IIa/B). 5 In this case, the patient did not present with a related Kommerell’s diverticulum, and no treatment for aortic pathology was required. Therefore, we opted for a less invasive percutaneous intervention. The radial artery approach has demonstrated significant advantages in both neurointerventional and cardiovascular interventions, as it significantly reduces the incidence of puncture site complications compared to the traditional femoral artery approach. 6 However, the safety of this approach in the presence of anatomical variations requires further clinical studies to confirm. Previous studies have reported similar cases of ARSA occlusion, but in those cases, the specific type and dimensions of the stent were not explicitly detailed. In our case, we selected a 9 × 40 mm self-expandable Carotid Wallstent (Boston Scientific), a device typically used for carotid artery interventions. This choice was tailored to the unique anatomical challenges of the ARSA: its self-expandable design provides sustained radial force to counteract potential elastic recoil of the occluded segment, while the 9 mm diameter matched the physiological caliber of the distal ARSA (assessed via preoperative CTA) to avoid overexpansion and adjacent structure compression (e.g. esophagus). This off-label use of a carotid stent for ARSA revascularization reflects the need for device flexibility in complex congenital vascular variants.
The remnant stump of ARSA was visible on the aortic arch, greatly increasing the success rate of the femoral artery approach and avoiding the need to navigate the tortuous subclavian artery.7,8 In the present case, DSA revealed the absence of a remnant stump on the aortic arch, which made it challenging to locate the origin of ARSA via the femoral artery approach.
In this patient, we used the Sino transradial long sheath (6F, 115 cm), which has the advantages of a small outer diameter (1.7 mm) and a large inner diameter (1.15 mm). Compared with other long sheaths, it is more conducive to catheter delivery. There are two key considerations when treating ARSA occlusive lesions via the radial artery approach: First, the abnormal origin of the vessel may cause an angular path, increasing the resistance to the delivery of the stent delivery system. Therefore, a low-profile stent and a supportive guiding catheter are necessary. Although the radial approach reduces puncture-site complications (hematoma, pseudoaneurysm) by 60%–80% compared to femoral access, retrograde intervention for aortic-ostial chronic total occlusion carries inherent risks. The ARSA origin’s acute angle from the distal aortic arch creates a biomechanical challenge: guidewire/catheter forces are directed laterally against the aortic wall during retrograde engagement, increasing iatrogenic dissection risk. Second, the distal ARSA often has branch intersections with the vertebral artery, and stent placement must balance lesion coverage with branch protection. In this case, balloon angioplasty followed by precise stent placement was used to cover the occluded segment, while angiography confirmed that the vertebral artery was not affected. This approach aligns with the “branch protection priority” principle emphasized in previous studies. Furthermore, during ARSA interventions, it is important to be cautious of iatrogenic dissection, which has been reported to occur in 3%–5% of cases. This may be associated with excessive catheter manipulation or guidewire penetration through the intima, highlighting the need for high surgical precision and thorough preoperative understanding of the anatomical structures to prevent dissection. Instrumentation of the ARSA occlusion inherently risks dislodging thrombus/plaque directly into the posterior cerebral circulation or compromising the VA ostium. This demands VA protection as the non-negotiable priority during all procedural steps.
Subclavian artery stents—especially in anomalous vessels with tortuous anatomical structures and high mechanical stress, such as the ARSA—have a 5-year in-stent restenosis incidence as high as 15%. 9 Rigorous imaging follow-up (e.g. annual CTA examinations) is essential to detect asymptomatic restenosis before symptom recurrence. In addition, the retroesophageal course of the ARSA renders its stent vulnerable to repeated compression from esophageal and cervical spine movements. 10 CTA monitoring every 1–2 years can identify stent fracture, migration, or deformation, which may necessitate re-intervention. Patients with congenital arch vessel malformations may develop new atherosclerotic lesions in adjacent vessels (e.g. vertebral artery, carotid artery). Lifelong clinical evaluation (including bilateral blood pressure measurements and neurological examinations) combined with regular imaging studies is therefore crucial.
This case report still has limitations. First, duplex ultrasound should be actively rechecked postoperatively to assess the recanalization of the occlusion. Second, imaging examinations should be completed during follow-up to observe the stent deployment and detect any restenosis.
In summary, this is the first reported case of stent treatment for complete ARSA occlusion via the radial artery approach, offering new technical insights and references for the treatment of patients with similar complex vascular anatomy in clinical practice. The safety of this method should be further validated in future clinical studies.
Conclusion
ARSA is the most common congenital anomaly of the aortic arch. This case suggests that percutaneous radial artery access for the treatment of symptomatic complete occlusion may provide a safe surgical repair alternative for select patients.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Authors obtained written patient consent for the use of their photographs and medical information to be published online, and with the understanding that this information may be publicly available and discoverable via search engines.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (contract grant no. 82302137 to L.Y.)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.