
Abstract
An aberrant origin of the right subclavian artery arising as the most distal vessel from the aortic arch is an uncommon but clinically important anomaly. Its abnormal course may result in esophageal compression with dysphagia, or tracheal compression resulting in asthma or stridor, and can greatly complicate radial artery access for coronary angiography. When an aberrant right subclavian artery is obstructed by atherosclerotic plaque, it may produce symptoms of arm ischemia such as pain and weakness. For the past 75 years, the standard treatment approach for symptomatic aberrant right subclavian artery has been surgical correction. There are only three case reports of percutaneous therapy, all for nonocclusive stenosis. There are no reported cases of percutaneous treatment of a completely occluded aberrant right subclavian artery. We report a patient with exertional right arm heaviness and weakness who was found to have a 60-mm long aberrant right subclavian artery occlusion. The blockage was successfully treated with angioplasty and placement of a single stent using percutaneous vascular access. Chest computerized tomography and duplex ultrasonography 5 years after treatment demonstrated a patent stent. At 7-year follow-up, she remained symptom-free and had a normal radial pulse. This case represents the first report of total occlusion of aberrant right subclavian artery treated percutaneously. Long-term durability supports this as a viable alternative to surgery in appropriately selected patients.
Keywords
Introduction
The most common congenital abnormality of the aortic arch is an aberrant right subclavian artery (ARSA).1,2 The prevalence in the general population has been estimated to be 0.2%–2.5%. 3 Individuals with this condition have four major vessels arising from the aortic arch: the right common carotid artery, the left common carotid artery, the left subclavian artery, and the right subclavian artery, with the right subclavian as the most distal of the four. The embryologic explanation for this variant is that the proximal fourth aortic arch regresses abnormally with persistence of the distal portion. The seventh intersegmental artery remains attached to the descending aorta. This persistent artery becomes the proximal portion of the ARSA.1,4 In this anomaly, the right subclavian passes from its origin on the left side of the body, crossing the midline, usually posterior to the esophagus, to provide blood supply to the right arm. As a result of this pathway, the vessel sometimes interferes with esophageal function, resulting in “dysphagia lusoria.” 1 Tracheal obstruction may result in wheezing or stridor. 2 Most patients, however, are asymptomatic. Symptomatic patients with ARSA have usually been treated with surgical repair. 4 Surgical technique has evolved over the years in an attempt to optimize upper extremity and vertebral artery blood flow, while minimizing surgical morbidity. Early operations involved a median sternotomy and direct anastomosis of the ligated ARSA to the ascending aorta proximal to the right common carotid artery. Current techniques involve a supraclavicular incision and anastomosis of the ARSA to the right common carotid artery, avoiding thoracotomy or sternotomy. 4 The right vertebral artery typically arises from the ARSA, and special care is necessary to preserve its integrity during surgical repair.
Case report
A 57-year-old woman with a history of hypertension, diabetes, hyperlipidemia, and cigarette smoking presented with an acute myocardial infarction. She underwent successful stent placement in the left anterior descending coronary artery using femoral artery access. During her initial hospitalization, she also reported lifestyle-limiting left leg claudication, and right arm heaviness and weakness exacerbated by movement. She reported no focal neurologic symptoms and had no dysphagia. Left arm blood pressure was 130/90 mm Hg and right arm blood pressure was 80/60 mm Hg. Left dorsalis pedis and posterior tibial pulses were not palpable. She returned 2 weeks later and underwent stent placement for a 95% stenosis of the left common iliac artery. Because right subclavian artery disease was also suspected based on arm symptoms and discordant arm blood pressures, arch aortography was performed at that time, demonstrating the stump of an occluded ARSA (Figures 1 and 2). Delayed imaging demonstrated collateral flow opacifying the distal vessel after a 60-mm occluded segment (Figure 3). The right vertebral artery originated from the right common carotid artery. Duplex ultrasound showed monophasic flow in the right subclavian artery with spectral broadening and a peak systolic velocity of 55 cm/s. After a discussion of therapeutic options for ARSA, the patient chose conservative therapy rather than surgery or percutaneous treatment. She was treated with aspirin, clopidogrel, and atorvastatin.

Left anterior oblique projection of aortic arch angiogram. The stump of the right subclavian artery is seen overlapping the left subclavian artery origin (white arrow). No distal right subclavian artery is seen. The right vertebral artery originates from the right common carotid artery (black arrow).

Right anterior oblique projection of aortic arch angiogram clearly demonstrating the stump of the aberrant right subclavian artery.

Delayed imaging after left anterior oblique aortic arch angiogram showing late filling of the distal right subclavian artery.
During routine follow-up, the patient continued to report exertional right arm pain, heaviness, and weakness. Two and a half years after her initial presentation, she requested percutaneous revascularization. She was aware that there were no prior reports of percutaneous treatment of total occlusion of ARSA. She gave written informed consent for endovascular repair, and later gave written informed consent for publication of this case.
The procedure was performed using right femoral artery and ultrasound-guided right brachial artery access (Figure 4). Ultrasound showed a 3.5-mm brachial artery diameter and 1.4-mm radial artery. Other than ultrasound, no additional pre-procedural imaging was performed. A 4-Fr multipurpose catheter was advanced with a stiff angled 0.035-in hydrophilic guidewire from the distal end of the occlusion. A 6-Fr 55-cm sheath was advanced from the femoral artery with its tip placed into the ARSA stump. The proximal cap of the occluded segment was penetrated with a stiff angled 0.035-in hydrophilic wire. This created a plane through which the brachial wire and multipurpose catheter could be advanced into the awaiting 6-Fr sheath (Figure 5). The wire was then exchanged for a 0.014-in non-hydrophilic support wire, over which a 4 mm × 12 cm balloon was advanced from the femoral sheath. Angioplasty was performed throughout the occluded segment, followed by placement of a 7 mm × 80 mm nitinol stent. Final inflation was performed using a 6 mm × 4 cm balloon. After treatment, there was no residual stenosis (Figure 6) and no pressure gradient between the aorta and right brachial artery. The radial pulse was normal. The patient received aspirin and clopidogrel.

Simultaneous angiography of the stump of the aberrant right subclavian artery from femoral artery access (black arrow) and retrograde subclavian angiography from brachial access.
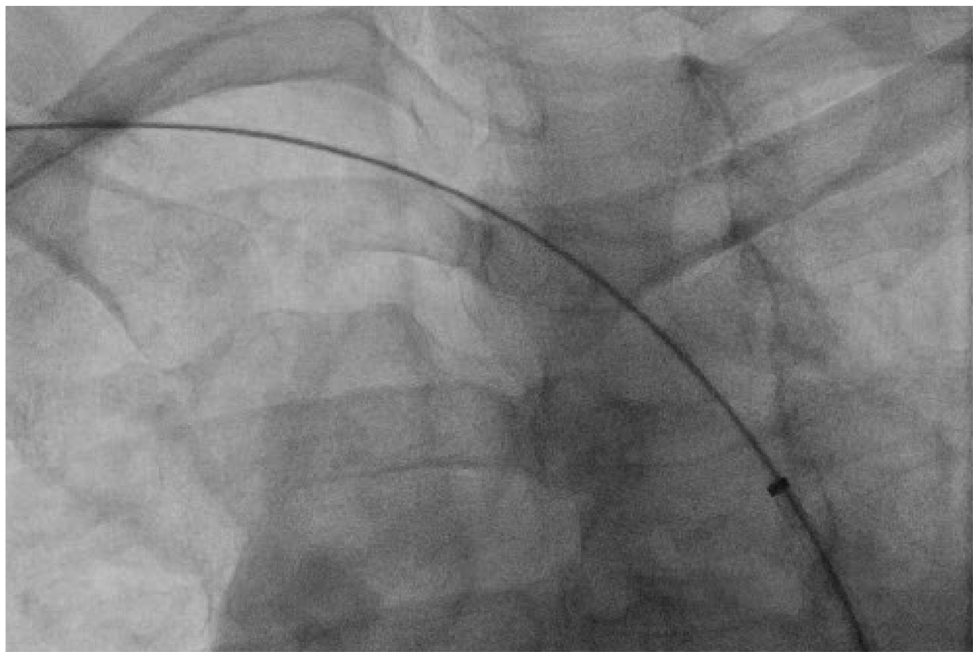
Retrograde wire passage from right brachial access, through the subclavian occlusion, and into the sheath placed from femoral access.

Final angiography demonstrating resolution of aberrant right subclavian occlusion by stent placement.
The patient has returned for routine follow-up for 7 years and has remained free of symptoms. Her radial pulse was normal on each follow-up visit. A chest computerized tomography (CT) was performed 5 years after the procedure, demonstrating a patent stent (Figure 7). Duplex ultrasonography at five and one-half years showed a patent stent, a normal triphasic subclavian artery waveform, and a peak systolic velocity of 129 cm/s.

CT angiographic image obtained at 5-year follow-up demonstrating a patent ARSA stent (white arrow).
Discussion
This case is unique in that percutaneous treatment of complete occlusion of ARSA has not been previously reported. It has been well-documented that complete occlusion of the subclavian artery is much more likely to result in an unsuccessful percutaneous revascularization attempt than is nonocclusive stenosis. For example, De Vries et al. 5 cited a 110 patient series with 100% success in stenotic lesions but only 65% in total occlusions. In addition, it is notable that clinical success in our patient has been maintained through long-term follow-up.
Percutaneous intervention is commonly performed for subclavian artery disease for individuals with normal vascular anatomy, 6 and is considered a viable alternative to surgical correction. In contrast, symptomatic patients with ARSA have customarily been treated with surgery, with the first successful procedure performed in 1945. 7 Standard surgical treatment for adults with occlusive disease is subclavian to right common carotid artery transposition.4,8 There are only three case reports of percutaneous management of ARSA stenosis. In 1998, Azakie described successful treatment of a symptomatic focal mid-vessel stenosis with self-expanding stents. 9 The patient was asymptomatic at 9-month clinical follow-up. No additional imaging was performed. In 2003, Basile reported self-expanding stent placement for a discrete ostial stenosis in a symptomatic patient. 10 The patient was asymptomatic at 6 months with CT evidence of vessel patency. Taha reported prophylactic treatment of a 22-mm long 58% ostial stenosis in a patient without arm symptoms who was being prepared for coronary artery bypass surgery using a right internal mammary artery graft. 11 Follow-up was limited to immediate postoperative observation. There are no prior reports of treating total occlusion, long-segment disease, or with long-term follow-up, including ultrasound imaging, all of which were present in this case. Thus, this case presented a greater challenge to treat and had substantially more follow-up. A similarity between our case and the three prior reports was that in all four instances, there was no associated Kommerell diverticulum (KD). As a result, there was no need to treat aortic pathology.
In addition to ARSA, our patient also had an anomalous origin of the right vertebral artery from the right common carotid artery, as has been reported previously. 8 This enhanced the safety of percutaneous treatment, in that it effectively eliminated the risk of embolization to the posterior cerebral circulation. As in any case of complete occlusion of the subclavian artery, percutaneous treatment carried the risk of vessel rupture with potentially disastrous hemorrhage. Should that have occurred, the treatment strategy was balloon tamponade followed immediately by covered stent placement. Another possible outcome was failure to cross the occlusion, leading to an unsuccessful procedure. Had that happened, a discussion would have been undertaken with the patient about continued conservative management versus carotid-subclavian bypass. Although surgical repair would have been a reliable means to revascularize the limb, the choice to pursue an endovascular first approach was based to a large degree on the known complications of surgical repair. A recent surgical series cited phrenic nerve palsy in 25%, recurrent laryngeal nerve palsy in 5%, axillary nerve palsy in 2%, and neck hematoma requiring re-exploration in 1%. 12
ARSA is frequently accompanied by KD, which increases management complexity. KD can produce symptoms of dysphagia, wheezing, and stridor as described above. In addition, it predisposes to aortic rupture and dissection. 12 There is widespread agreement that symptomatic KD merits repair, whereas the management in the absence of symptoms is less clear. A standard surgical approach has been subclavian-common carotid artery transposition or bypass in conjunction with KD resection and interposition aortic grafting. A modification of this technique involves a subclavian interposition graft connecting the aortic graft to the distal ARSA. 12 An endovascular approach is often precluded by the absence of an adequate landing zone for stent graft placement.13,14 A variety of hybrid approaches has been reported. 15 Total arch repair using median sternotomy has been described. 16 The management of our case was greatly simplified by the absence of KD.
Recognition and management of upper extremity arterial vascular anomalies have gained significantly more importance in recent years as radial artery access for coronary artery angiography has grown in popularity. A convincing body of the literature has demonstrated a reduction in mortality, major acute cardiovascular events, and cost associated with radial versus femoral access. 17 Most procedures are performed from the right arm, ensuring that ARSA will be encountered when present. This anomaly can be easily missed in femoral access cases.
Conclusion
ARSA is the most common congenital anomaly of the aortic arch, and is likely to be recognized more commonly in the current era of radial artery access. This case demonstrated that percutaneous treatment of symptomatic long-segment total occlusion may provide a safe and durable alternative to surgical repair in selected patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.