
Abstract
Heterotopic pregnancy is rare. We report a 27-year-old lady with polycystic ovarian disease. She presented at our health facility with acute abdomen. Her evaluation revealed heterotopic pregnancy. High index of suspicion for heterotopic pregnancy in any woman with early pregnancy presenting with acute abdomen is crucial. Therefore, correct and early diagnosis allows appropriate management while it preserves the intrauterine pregnancy as in the index case.
Introduction
Heterotopic pregnancy occurs in multiple gestations, with one being present in the uterine cavity and the other outside the uterine cavity. It is a rare condition, estimated to occur in 1 in 30,000 pregnancies. 1 However, with the widespread use of assisted reproductive techniques (ART), the incidence has increased to 1 in 3900 pregnancies. 1 On the contrary, the incidence has been estimated to be 33/10,000 for patients who have been treated with ovulation induction medication. 2 The case described below is of a 27-year old lady with polycystic ovarian disease, who had presented at 8 weeks of gestation with heterotopic pregnancy characterized by intrauterine pregnancy and an unruptured ectopic pregnancy on the right fallopian tube.
Case report
A 27-year-old, Gravida 2 para 0 + 1, with polycystic ovarian disease (Figure 1) on Metformin and Pioglitazone for 4 years came to our facility with amenorrhea for 6 weeks. Trans-abdominal ultrasound was performed, and an intrauterine gestation sac was detected with mean sac volume corresponding to 5 weeks and 5 days without yolk sac or fetal poles and hence advised follow-up ultrasound after 2 weeks to assess fetal viability (Figure 2). She was admitted at 8 weeks of gestation with sudden onset of sharp lower abdominal pain radiating to the back without vaginal bleeding. Her assessment was indicative of 4-year history of primary infertility. She was on Letrozole till conception. There was no history of any surgical procedures, pelvic inflammatory diseases, or use of contraception.
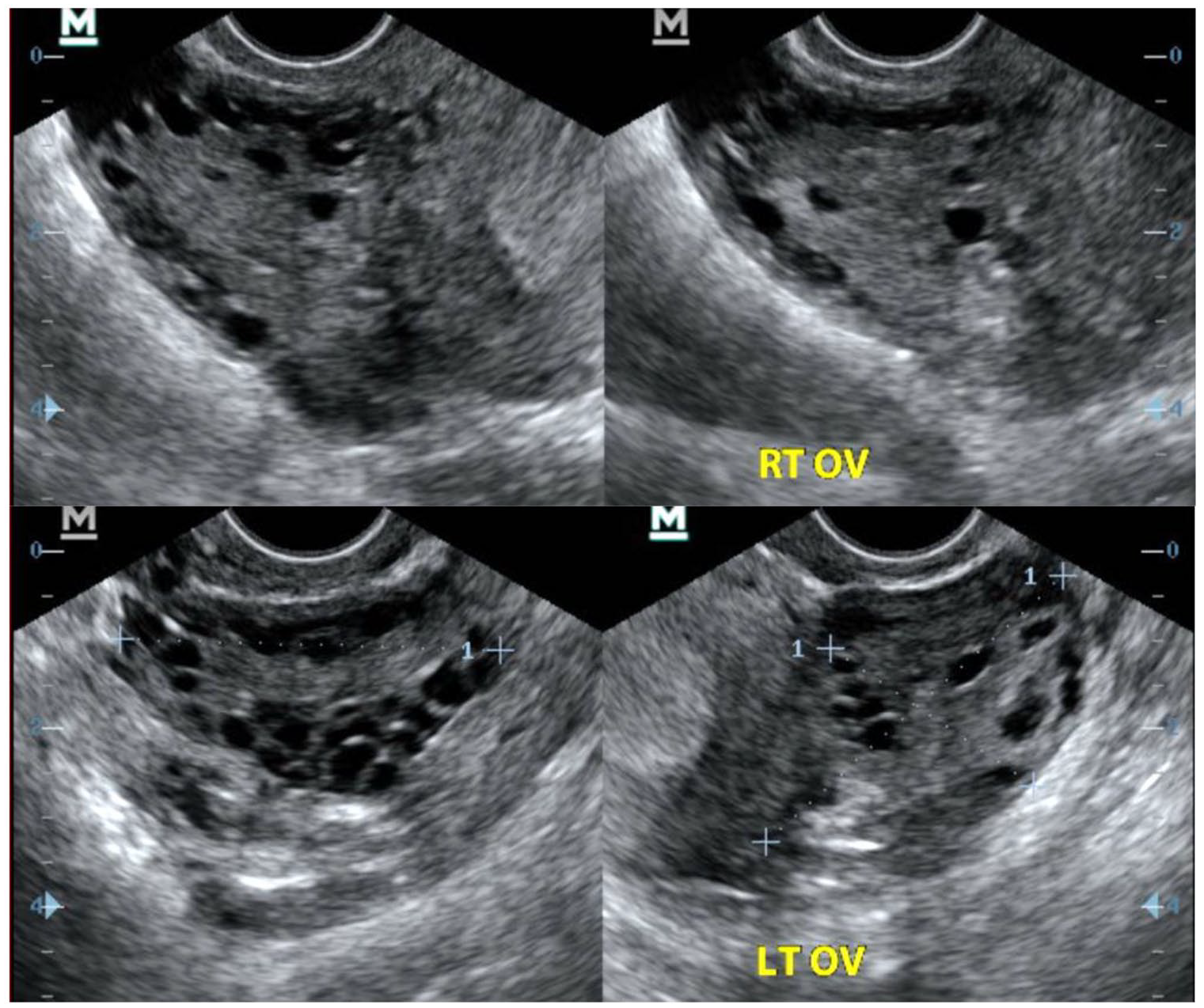
Transvaginal pelvic ultrasound transverse and sagittal images of right and left ovaries demonstrating enlarged ovaries with multiple sub-centimeter peripheral cysts.

Trans-abdominal pelvic ultrasound at 5 weeks and 5 days which shows an intrauterine gestation sac without yolk sac or fetal poles marked with (*) and normal adnexa as well as no free fluid in the pelvis.
On examination, she was clinically stable, alert, afebrile, with body temperature of 36.9°c, pulse rate of 85/min, and blood pressure at 108/54 mm Hg. She had beard and male pubic hair pattern (Ferriman-Galleway score of 6) 3 with no acne, nor galactorrhea or thyroid gland enlargement. Her abdominal examination revealed mild tenderness on the right iliac fossa with negative Rovsing‘s sign. Other systems examination was uneventful.
She underwent ultra-sonographic examination, which showed a viable intrauterine pregnancy corresponding to 7 weeks and 4 days gestational age, with normal trophoblastic tissues and fetal heart rate of 176 beats/min. In addition, an unruptured extra uterine gestational sac was found in the right adnexa with gestational age corresponding to 8 weeks, with cardiac activity seen and fetal heart rate of 146 beats/min (Figure 3).

Transvaginal pelvic ultrasound images revealing live intrauterine and extra uterine gestations on the right and left images, respectively.
She then underwent emergency exploratory laparoscopy, which revealed a slow leaking ectopic pregnancy with intact gestational sac seen in the right ampullary region of the fallopian tube (Figure 4). Right salpingectomy was then done. There was minimal hemoperitoneum seen of about 100 mL of blood. The uterus appeared bulky while the ovaries were of normal size and appeared healthy.

Laparoscopy image demonstrating the right adnexal gestation sac with a fetus within marked with (*).
Postoperative course was unremarkable. The patient was prescribed Progesterone injection 100 mg STAT with antibiotics for the first 72 h (prophylaxis for infections such as pelvic inflammatory disease post procedure). She was discharged home to continue follow-up as an outpatient.
Follow-up ultrasound which was taken 6 days post operation showed an 8 week and 5-day fetus with fetal poles, and fetal heart rate of 171 bpm (Figure 5). There was no peri sac bleed. She was also prescribed Duphastone (Dydrogesterone) 10 mg every 8 h and folic acid 5 mg daily. Anomaly scan done at 19 weeks gestation found a normal fetus. The patient continued taking junior aspirin, and multivitamin supplements too.

Transvaginal pelvic ultrasound 1-week post laparoscopic salpingectomy reveals live intrauterine gestation.
During the third trimester, she had bouts of mild pelvic pain that was managed by analgesics such as paracetamol. The junior aspirin was stopped at 32 weeks of gestation. She continued taking multivitamin supplements. The patient was counseled on the mode of delivery. She opted for cesarean section.
At 38 weeks and 5 days, cesarean section was done where a 3.16 kg male baby was delivered with APGAR 4 score of 9 at 1 min and 9 at 5 min. Intraoperatively there were no adhesions and the right adnexa had healed well. Post-delivery, patient recovered well. Both the mother and baby were reviewed 6 weeks after cesarean section and were found to be doing well with no complications.
Discussion
Heterotopic pregnancy is a relatively rare condition, hence it can be easily misdiagnosed because its symptoms mimic those of ectopic pregnancy, that is, abdominal pain, vaginal 1 bleeding However, some cases may be asymptomatic and others with vague symptoms. 5 In our case, the symptoms were mild in a stable patient. Luckily, our patient underwent transvaginal ultrasound immediately and both intrauterine and tubal pregnancies were clearly diagnosed. On the contrary, some cases may present with asymptomatic heterotopic pregnancy that is missed by an ultrasound because of either sonographer experience or less attention being given to adnexa after seeing an intrauterine gestational sac. Hence, high clinical suspiciousness as well as detailed sonographic survey are crucial.5–7
The etiology of heterotopic pregnancy is not known. However, a few theories have been postulated including pelvic inflammatory diseases, previous tubal surgery, ovarian stimulati on drugs, and ART.1,8 Moreover, polycystic ovary syndrome (PCOS) has been reported to be associated with complications during pregnancy with ectopic being one of them. 9 Besides the postulated risk factor, a sizable number have no such risk factors. Our patient had used ovulation induction drugs.
Identification of intrauterine gestation should not exclude the possibility of looking for extra-uterine gestation and so adequate evaluation of adnexa should be performed in all early pregnancy ultrasound.10,11 It has also been suggested that use of polycystic ovarian morphology (PCOM) can help in early diagnosis of ectopic pregnancy. 12 Therefore, in patients who had difficulty with conception leading to the use of ovulation drugs, their assessment should be comprehensive as it was in our case.
There has been no consensus on the management of heterotopic pregnancy. This is due to the rarity of the cases. However, the common methods are expectant management, surgical in form of laparoscopy or laparotomy, and sonographically guided embryo aspiration with or without embryo killing drugs such as potassium chloride and hyperosmolar glucose.8,13 There are some indications and contraindications to expectant management. In our case this could not be applied as the ectopic gestation was viable. The patient underwent emergency laparoscopy where right salpingectomy was done.
Conclusion
Although rare, heterotopic pregnancy should be considered in any woman with early pregnancy presenting with clinical features of acute abdomen and there should always be a high index of suspicion. Thorough investigation using ultrasound and, if necessary, pelvic magnetic resonance imaging (MRI) to exclude heterotopic gestation should be performed. Correct and early diagnosis would allow appropriate management preserving the intrauterine pregnancy as in the index case.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from The Ethical committee of The Aga Khan Hospital-Dar es salaam
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.