
Abstract
Objectives:
A short birth interval is a universal public health problem resulting in adverse maternal, neonatal, and child outcomes. Therefore, the aim of this study was to identify determinants of short birth interval among ever married reproductive age mothers who live in Jigjiga city administration, Eastern Ethiopia, 2020.
Methods:
A community-based unmatched case–control study was used among 194 cases and 194 controls in Jigjiga city administration from September to December 2020. Cases were women with short birth interval (less than 3 years) and controls were women with optimum birth interval (3–5 years). Simple random sampling technique was employed to select cases and controls. Data were entered into Epi data version 4.2 and analysis with SPSS version 22. Binary logistic regression with 95% confidence interval at p < 0.05 is used to declare significantly associated predictors of short birth interval.
Result:
This study reported that women who have not attended formal education (adjusted odds ratio = 5.28, 95% confidence interval: (2.25–12.36)), attended primary education (adjusted odds ratio = 2.79, 95% confidence interval: (1.46–5.34)), women who married to a polygamous husband (adjusted odds ratio = 3.69, 95% confidence interval: (1.80–7.58)), having a history of neonatal death (adjusted odds ratio = 2.15, 95% confidence interval: (1.07–4.32)), preceding child being female (adjusted odds ratio = 3.69, 95% confidence interval: (2.02–6.72)), and never used contraceptive methods (adjusted odds ratio = 3.69, 95% confidence interval: (2.02–6.72)) were identified as determinants of the short birth interval.
Conclusion:
Short birth intervals were associated with educational level of the women, sex of the baby, husband marriage types, history of neonatal death, and contraceptive utilization. Strategy should be engaged to enhance women education, contraceptive uses, and to decrease neonatal death.
Introduction
The birth interval is defined as the time interval between a live birth and the birth of the next child. The World Health Organization (WHO) recommends waiting at least 24 months before trying to conceive again. There is consistent evidence that a 2-year interval between births increases the chances of survival for newborns and children; on the contrary, new confirmation from WHO shows that 3–5 years is the best interval between births and can minimize the risk of adverse consequences for the mother, child, and neonatal period.1,2
There are four ways to determine the birth spacing or birth interval: the first method is the birth and birth interval of the live-born baby; the second method is the outcome interval, that is, the time interval between the result of this pregnancy and the result of the last pregnancy; the third method is the interval from birth to conception. This represents the time lapsed from the conception of the current pregnancy to a live child in the last pregnancy. The fourth method is the inter-pregnancy interval, that is, the time interval between two consecutive pregnancies. 2
Short birth spacing is a global health problem and it is a main hindrance to achieve the Sustainable Development Goal of eliminating preventable infant and maternal deaths. 3 There are disreputable adverse outcomes for mothers, newborns, and child due to a short birth interval.4,5 Likewise, adverse pregnancy outcomes associated with shorter pregnancy intervals can be explained by a variety of mechanisms, including hypothetical maternal malnutrition (nutrition stress due to prolonged pregnancy and lactation) and possible maternal folate deficiency, which means that a short birth interval will affect the recovery of women after pregnancy. 6 Also women with short birth intervals experience increased likelihood of complications like pregnancy-induced hypertension, 7 gestational diabetes, 8 placenta abruption, 9 anemia, obstructed labor, and uterine ruptures.10,11
Similarly, newborns and children born following short birth intervals are negatively impacted. As the interval between births gets shorter, the baby becomes weaker and withered.12,13 In addition, it has been found that babies born to mothers with shorter birth intervals are at high risk of small for gestational age,14,15 stillbirth, 16 low birth weight, 17 preterm delivery,18,19 and birth defects.20,21
Global countries attempt to slow population growth, but it continues to grow rapidly. This is mainly due to the high birth rate and closely spaced births. Empirically, short birth intervals have had a great contribution to population growth, besides overwhelming countries’ growth efforts. In addition, there are several factors that contribute to high birth rates and short birth intervals at the individual, family, and community levels, such as illiteracy, early marriage, and lack of family planning methods. Ultimately, formulating an effective family planning strategy requires an understanding of reproductive patterns and behaviors to ensure optimum birth spacing. 22
In Ethiopia, increasing the birth interval to at least 2 years reduced infant mortality by half. 23 Over the last 20 years, there has been no substantial change in the median birth interval, whereas the average birth interval has grown slightly but steadily. According to the Ethiopian Demographic and Health Survey (EDHS), the median birth intervals were 33.6, 33.8, 33.9, 34.5, and 35.8 months in 2000, 2005, 2011, 2016, and 2019. The median birth interval varies by region in the most recent EDHS, ranging from 26.0 months in Somali to 48.6 months in Amhara.24,25
Although there have been studies on short birth interval in Ethiopia, most previous studies were cross sectional which may not show real associations and they did not compare cases with controls. The few case–control studies done in Ethiopia had small sample sizes, which can lead to statistical imprecision. Furthermore, there is no available evidence of short birth interval in Somali regional. The aim of this study was to identify determinants of a short birth interval among ever married women live in Jigjiga city administration Eastern Ethiopia.
Methods and materials
The study was conducted in the Jigjiga city administration, the capital city of the Somali regional state, at the eastern Ethiopia from September to December 2020. The city is located at 635 km away from Addis Ababa. The city has 21 urban kebeles. The population of Jigjiga town is estimated to be 250,000, from which 123,422 are males and 126,578 are females. 26 There is one referral hospital, one general hospital, three health centers, 20 health posts, and 20 private clinics.
Study design
A community-based unmatched case–control study was conducted.
Study population
The study population were ever married reproductive age women living in chosen kebeles in Jigjiga who have at least two consecutive live births, the last delivery being within the past 5 years prior to the survey.
Inclusion criteria
Exclusion criteria
Not remember date of birth for the last successive two live births with a child having no birth certificate or immunization card.
Unable to speak or unable to response and could not make logical judgment were excluded.
Women with intervening pregnancy loss or termination were excluded.
Sample size determination
Sample size was determined using double population proportion formula for unmatched case–control study using Open EPI INFO version 7 software. Among several exposure variables, selection of the appropriate exposure variables in controls was done based on the main interest variables of cases of determinant for short birth interval. Consequently, the smallest detectable odds ratio (OR) of 1.8, a 5% level of precision, 95% confidence interval (CI), a power of 80%, and a one-to-one allocation ratio of optimum birth interval (controls) to short birth interval (cases) were supposed. In the control group, the proportion of women who did not attend antenatal care (ANC) prior to their last pregnancy was estimated to be 43%. 27 A non-response rate of 5% was taken into consideration. Under the above assumptions, the sample size was 388 (sample size 194 for cases + 194 for controls).
Sampling techniques and procedure
Four urban kebeles were selected from 20 kebeles of the Jigjiga City administration by means of simple random sampling. Hence, a preliminary assessment of reproductive age women live in each selected kebele was conducted to identify households with cases and controls along with their corresponding household identification numbers. Using respective household identification number, frames of households containing study participants defined as cases and controls was prepared. Then sample size was proportionally distributed for each selected kebele depending on the number of cases and controls identified during preliminary study. Finally, cases and controls were carefully chosen using simple random sampling techniques from a frame containing the respective source of population. Whenever more than one eligible respondent was found in the same household, only one was included in the study by lottery method.
Data collection methods
The data were collected using pretested structured interviewer administered questionnaire that was modified after reviewing different literatures. The questionnaire was initially prepared in English and then translated to local language (Af-Somali) and back to English by experts to possess its uniformity. The data were collected by eight BSc female Midwifes who were fluent in local language and two MSc supervisors. Two days training was given for data collectors and supervisors on data collection procedures, interview techniques, and confidentiality of the information obtained from the study participants.
Variables
Dependent variables
Birth interval (short/optimal spacing)
Operational definition
Independent variables
Socio-demographic factors such as age, ethnicity, religion, type of marriage, educational level of the mother, educational level of the husband, and occupational status of the husband;
Obstetrics and birth history–related factors such as regularity of menstruation, ANC visited preceding last birth, place of delivery, postnatal complication, history of infertility, had history of neonatal death, sex of preceding child, and husband perception regarding birth spacing.
Contraceptive and breast feeding–related factors like preceding to last child was exclusive breast feeding (EBF), during preceding to last birth breast feeding (BF), ever used contraceptive, using family planning (FP) is important for birth spacing, and husband perception on FP.
Data quality controls
Data quality was ensured during tool development, collection, and analysis. To ensure quality, questionnaire initially drafts in English language and then translated to local language. Before actual data collection began, training was given for data collectors and supervisors. Five percent of the questionnaires were pretested, and possible modification was made. The principal investigator and supervisors closely supervised throughout data collection period.
Data processing and analysis
After proper coding, the data were entered to Epi-data version 3.1 and exported to SPSS version 22 for analysis. Descriptive statistics was done for both cases and controls. Bivariate logistic regression analysis was carried out. A predictor which have p-value less than 0.25 on bivariate analysis was selected as a candidate for multivariable logistic regression analysis. Finally, the strength of associations between short birth interval and independent variables was assessed using adjusted odds ratio (AOR) and 95% CI. A p-value < 0.05 was used to determine the statistical association in the multivariable analysis.
Results
Sociodemographic characteristics
A total of 388 women have participated in this study. In this study, mean age for cases was 30.84 SD ± 6.37 and controls 28.87 ± 6.62. About 119 (61.3%) cases and 114 (58.8%) controls were between the age of 19 and 34. About 166 (85.6%) cases and 182 (93.8%) controls were Somali in ethnicity. Regarding educational status, 45 (23.2%) cases and 18 (9.8%) controls have not attended formal education. This research revealed 40 (20.6%) cases were married to husbands with polygamy in marital types (Table 1).
Sociodemographic characteristic of study participant in Jigjiga city, Eastern Ethiopia, 2021.

Obstetrics and birth-related factors
The mean duration of the birth interval for this study was 34.17 ± SD 14.178 months and the mean birth interval for cases is 21.09 ± SD months, and mean age of birth interval for controls was 47.21 months with ±7.27 SD. The minimum birth interval for cases was 10 months and maximum was 35 months. In the study, 34 (17.5%) cases and 17 (8.8%) controls had a history of neonatal death. It is also found that 73.2.8% of cases and 60.8% of controls proceeding to the last baby were female (Table 2).
Table obstetrics and birth characteristics of the participant in Jigjiga City administration, Eastern Ethiopia, 2020.
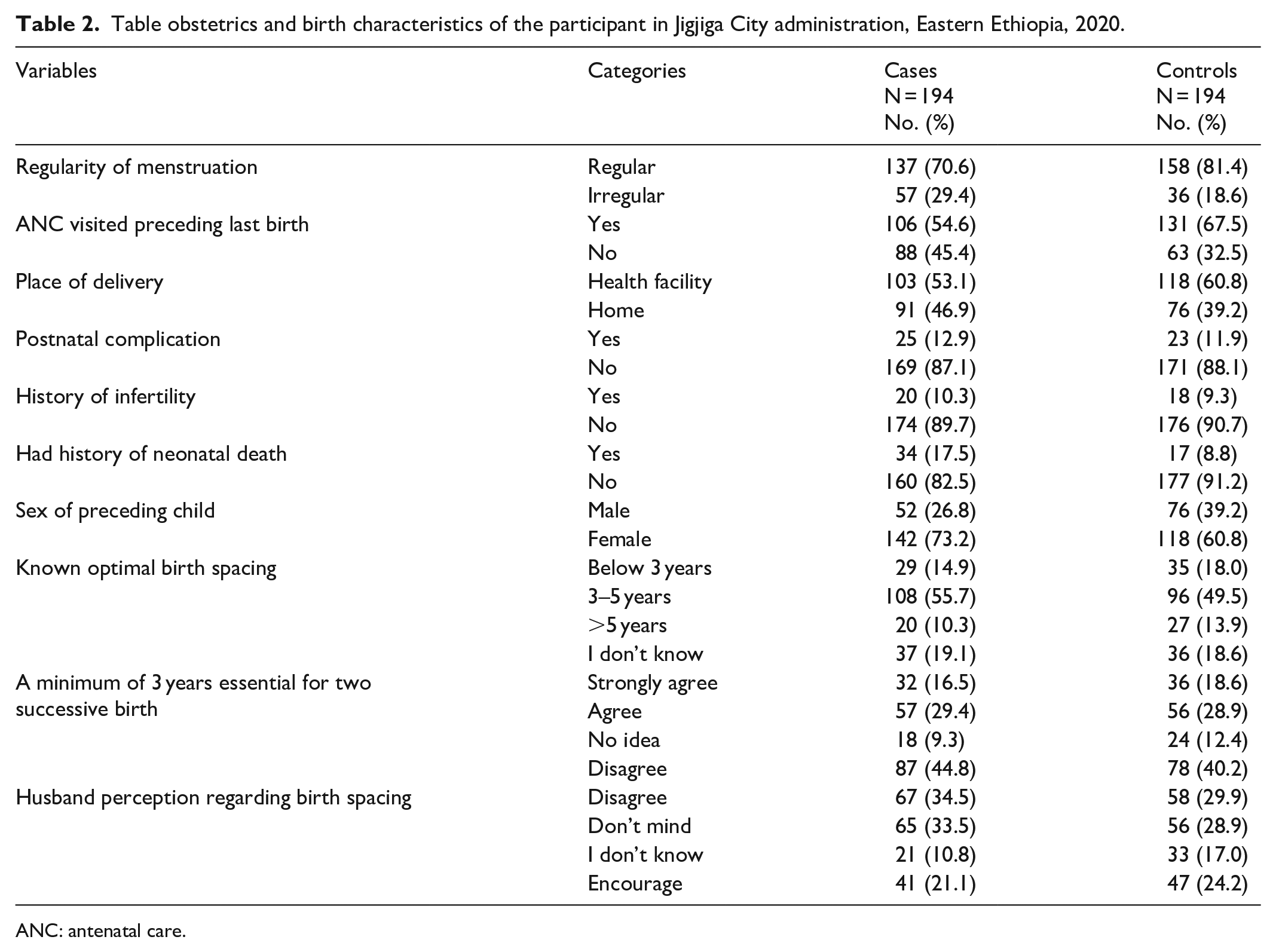
ANC: antenatal care.
Breast feeding and contraceptive-related factors
In the current study, 91 (46.9%) cases and 99 (51%) controls had practiced exclusive breast feeding proceeding to the last child. Only 33 (17%) cases and 50 (25.8%) controls ever utilized modern contraceptive methods. This study found that 68 (35.1%) cases and 63 (33.5%) controls mention that their husbands strongly disagree with family planning (Table 3).
Contraceptive and breast feeding–related characteristics of participants in Jigjiga city administration, Eastern Ethiopia, 2020.

BF: breast feeding; EBF: exclusive breast feeding; FP: family planning.
Determinants of birth interval (multivariate analysis)
In this study, education level of the mother, husband marital types, history of neonatal death, contraceptive uses, and sex of the preceding baby were predictors that exhibited associations with short birth interval.
The educational level of the mother was significantly associated with a short birth interval. Those women who had not attended formal education were 5.28 times (AOR = 5.28, 95% CI = (2.25–12.36)) and who attended primary education were 2.79 times (AOR = 2.79, 95% CI = (1.46–5.34)) more likely to have short birth interval than those who attended higher education. Husband polygamous marital status were among predictors that show association with a short birth interval. The odds of short birth interval were 3.69-fold greater (AOR = 3.69, 95% CI = (1.80–7.58)) among women whose husbands’ marital status were polygamous than their counterparts. Having a history of neonatal death was significantly associated with short birth interval. Women who had a history of previous neonatal death were 2.15 times (AOR = 2.15, 95% CI = (1.07–4.32)) more likely to experience a short birth interval compared with women had no history of neonatal death. The sex of preceding baby was found to be a strong predictor associated with short birth interval. Women whose preceding birth was a female were 3.69 times more likely (AOR = 3.69, 95% CI = (2.02–6.72)) to have a short birth interval than those whose child was male. Modern contraceptive utilization was among strong predictors of short birth interval. Those women who never used a contraceptive method had 2.44 times greater (AOR = 2.44, 95% CI = (1.30–4.58)) chance to have short birth interval compared with those who had ever used contraceptive method (Table 4).
Bivariate and multivariable analysis of determinants of short birth interval in Jigjiga city administration, Eastern Ethiopia, 2020.
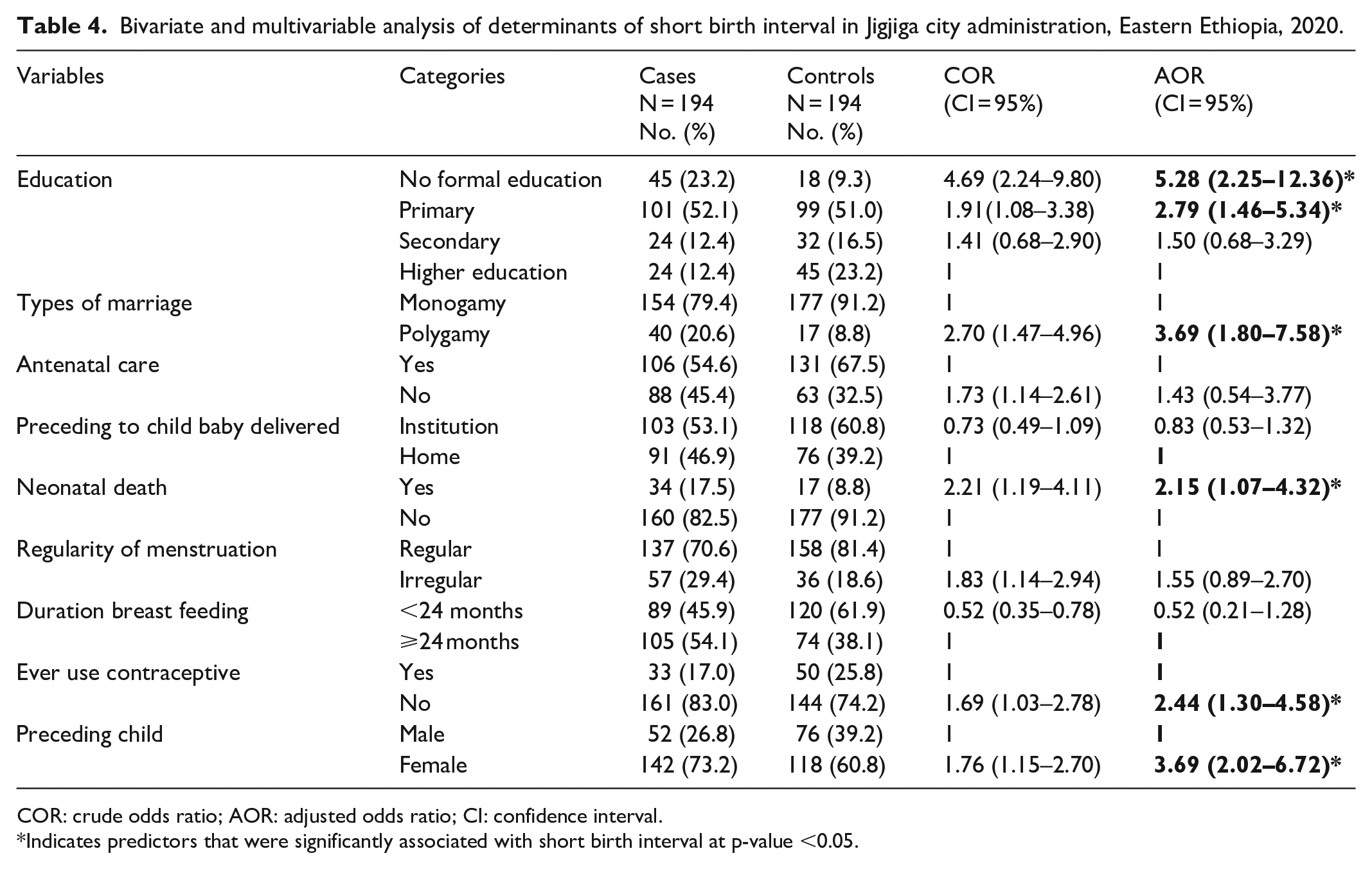
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Indicates predictors that were significantly associated with short birth interval at p-value <0.05.
Discussion
In this study, women’s education level, marriage type, neonatal death history, contraceptive use, and the sex of the previous child were significantly correlated predictors of short birth spacing in Jigjiga.
The education level of a woman is an important factor in determining the interval of birth. In the current study, women who have attended elementary school and women who have not received a formal education are more likely to be associated with shorter birth intervals than women attended higher education. Different studies done in Ethiopia and Iran agree with the present study.28,29 This might be due to the fact that illiteracy restricts women’s ability to make independent decisions and makes them less autonomous in terms of maternal health usage. Many studies have shown that women with less education have less autonomy in accessing high-quality health care, such as family planning, and birth spacing.30 –32 Furthermore, women with a lower level of education are more likely to be unaware of the negative consequences of short birth intervals. However, in the current study, there was no difference in birth spacing knowledge responses between cases and controls. This might be due to the fact that health care practitioners taught their clients during the latter pregnancy’s antenatal visit, since data collection took place after the latter pregnancy.
In contrast with other studies, the current study found that husband marriage types were associated with short birth intervals. According to current study, women whose husband marriage types were polygamous were about threefold more likely to have short birth intervals as compared with women married to monogamous husbands. This may be due to the cultural influence of the society; it may also be due to the husbands’ perception toward getting so many children. Another possible explanation might be a competition related to fertility, which encourages wives to give birth quickly and have multiple children.
The other predictor found to be associated with the duration of birth spacing was sex of preceding child. Those women whos’ proceeding to last baby birth was females were about four times likely to have short birth interval. This is also supported by other case–control studies conducted in southern Ethiopia and middle- and low-income countries.33 –35 Societies usually prefer boys for social, cultural, and religious reasons and having many boys may economically benefit the family. This could be the underlying reason that put pressure on fertility as couples continued to have children until they had their desired number of sons.
Neonatal death has shown an association with a short birth interval. Women who ever had neonatal loss were more likely to have a short birth interval. Other studies conducted in Ethiopia, Bangladesh, and middle- and low-income countries support this finding.36 –38 This may be because the couple desires to replace the dead neonate immediately. It is also due to the fact that once a newborn dies, no more breast feeding is practiced, making women more susceptible to pregnancy without another form of contraception.
Contraceptive use has been shown to be related to closed birth intervals. Compared with their counterparts, women who have never used contraceptive methods are significantly associated with shorter birth intervals. This is also reported by several studies conducted in Ethiopia and Nigeria.39 –42 It might be due to the fact that contraceptive usage delays a birth interval and limits the total fertility rate as it influences the reproductive process. Women who never use the contraceptive may also miss the opportunity to contact a healthcare provider, leading to reduce awareness related to outcome of short birth interval.
Limitation
This research, like many others, may have certain limitations, such as random error in reporting. The selection method may have resulted in unintentional matching on neighborhood setting, making selected controls appear more similar to cases. Characteristics of cases may be even more dissimilar from controls than they appeared in this study. The ascertainment of predictors occurred following the latter pregnancy. It is possible that some values (such as maternal age and knowledge regarding optimal birth spacing) changed after the interval. Ideally, to understand which values are the strongest predictors of short intervals, the variables would have been ascertained at the end of the prior pregnancy, before the start of the interval. This timing also coincides with the window when intervention to lengthen the interval would be possible. The strongest associations between short intervals and adverse pregnancy outcomes have been observed with intervals of <6 to <18 months, whereas this study focused on intervals of <3 years. The predictors of very short intervals may be different or more extreme than those reported in this study.
Conclusion
According to current study, women educational level, husband polygamous marriage, sex of the baby, neonatal death, and contraceptive were found to be determinants of short birth interval in Jigjiga city. Therefore, community health offices and other concerned bodies should establish comprehensive maternal and neonatal health care to prevent neonatal deaths and increase contraceptive utilization. Local administration should give emphasis on polygamous marital types. In addition, further study should be conducted using different setting and design.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211067870 – Supplemental material for Determinants of short birth interval among ever married reproductive age women living in Jigjiga, Eastern Ethiopia 2020 (unmatched case–control study)
Supplemental material, sj-docx-1-smo-10.1177_20503121211067870 for Determinants of short birth interval among ever married reproductive age women living in Jigjiga, Eastern Ethiopia 2020 (unmatched case–control study) by Abdurahman Kedir Roble, Mohamed Omar Osman, Ahmed Mohamed Ibrahim, Girma Tadesse Wedajo and Seid Abdi Usman in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121211067870 – Supplemental material for Determinants of short birth interval among ever married reproductive age women living in Jigjiga, Eastern Ethiopia 2020 (unmatched case–control study)
Supplemental material, sj-docx-2-smo-10.1177_20503121211067870 for Determinants of short birth interval among ever married reproductive age women living in Jigjiga, Eastern Ethiopia 2020 (unmatched case–control study) by Abdurahman Kedir Roble, Mohamed Omar Osman, Ahmed Mohamed Ibrahim, Girma Tadesse Wedajo and Seid Abdi Usman in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Jigjiga University and Jigjiga city administration. Also we thank all data collectors who participated in this study.
Author contributions
All authors have made a significant contribution to the conception, study design, acquisition, data analysis, and interpretation of the result. They also took part in drafting the manuscript, critically reviewed and agreed on the journal to which the article has to be submitted. All authors read and approved the final version of the manuscript and agreed to be accountable for all contents of the manuscript.
Data sharing statement
The datasets used for analysis are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study “Determinants of Short Birth Interval among Ever Married Reproductive Age Women Living in Jigjiga, Eastern Ethiopia 2020 (Unmatched Case–Control Study)” was obtained from Jigjiga University Institution of Research and Ethics Review Board (JJURERB0030/2020).
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of, Jigjiga University. Support letters were written to Jigjiga city administration where the study was actually conducted. The informed, voluntary, written and signed consent was obtained from each study participant. Study participants were clearly informed about their right to withdraw/refuse at any stage of the study if they did not want to participate and confidentiality of the information was assured. In addition, written informed consent was also obtained from legally authorized representative of the minor (aged less than 18 years) subjects included in the study. The data collectors interviewed the participants in separated areas. Confidentiality of information and privacy of participants were respected. This study was conducted in accordance with the Declaration of Helsinki. the written informed consent was also obtained from legally authorized representative of the minor subjects included in the study
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Jigjiga University. The funding organizations had no role in the study design, data collection, data analysis, and writing up of the manuscript.
Informed consent
Written informed consent was obtained from all subjects before the study. Verbal and write informed consent was obtained from all subjects before the study. In addition, written informed consent was also obtained from legally authorized representative of the minor (aged less than 18 years) subjects included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.