
Abstract
Introduction and Objective:
Postdural puncture headache is one of the most frequent late complications of spinal anesthesia. There are different factors that might predispose for postdural puncture headache. Therefore, the main aim of this study was to assess the incidence of postdural puncture headache and its associated factors for parturients who gave birth by cesarean section under spinal anesthesia.
Methods:
Hospital-based longitudinal study was conducted on mothers who underwent cesarean section with spinal anesthesia. Descriptive analysis and chi-square test were employed. Bivariable and multivariable logistic regression were used to measure the association of factors with the presence of postdural puncture headache. A p-value of ⩽0.05 was used to decide statistical significance for multivariable logistic regression.
Result:
A total of 119 parturients were participated in this study. The incidence of postdural puncture headache was 20.2%. According to multivariable logistic regression, having previous spinal anesthesia (adjusted odds ratio = 7.028; 95% confidence interval = 2.377–20.781; p = 0.0001), using 20- and 22-gauge needle (adjusted odds ratio = 4.206; 95% confidence interval = 1.247–14.187; p = 0.021), and repeated attempt (adjusted odds ratio = 4.699; 95% confidence interval = 1.594–13.872; p = 0.05) had statistically significant association with postdural puncture headache.
Conclusion:
Larger gauge needle size, repeated attempt, and previous spinal anesthesia might increase the incidence of postdural puncture headache.
Introduction
Spinal anesthesia is widely used for cesarean section currently for its safety, low cost, reliability, easiness to administer, immediate effect, and well-operating conditions.1–3 This technique is not free from complications. Postdural puncture headache (PDPH) is one of the most frequent complications of spinal anesthesia which usually occurs within 1–2 days after dural puncture and commonly resolves spontaneously or with simple analgesia.1,4–7 The differential diagnosis of PDPH is broad and includes other complications of dural puncture as well as headaches attributable to the condition which leads to the procedure. The patterns of development of PDPH depend on a number of procedure- and non-procedure-related risk factors.4,8 Parturients are at great risk to develop PDPH because of sex, young age, and the widespread application of regional anesthesia. 5 According to literature, the incidence of PDPH after spinal anesthesia ranges from 0.3% to 40% and is affected with factors such as age, gender, needle size and type, multiple attempt of spinal performance, and previous PDPH.1,2,5,7,9,10 Performing spinal anesthesia at sitting position is more risky for the occurrence of PDPH than in lateral position. 2 Being female, young age, and having lean body weight are the risk factors to develop PDPH after spinal anesthesia. Pregnant mothers are considered at increased risk of PDPH due to high levels of estrogens which can influence the tone of the cerebral vessels, thus increasing the vascular distension response to cerebrospinal fluid (CSF) hypotension.5,11 A diagnostic hallmark of PDPH is that it worsens in upright position and improves with lying down. Conservative therapies such as bed rest, hydration, and caffeine are commonly used as prophylaxis and treatment for this condition; however, no substantial evidence supports routine bed rest and aggressive hydration. 6 According to the International Classification of Headache Disorders criteria, PDPH is a headache develops within 5 days after dural puncture and disappears spontaneously within 1 week, or up to 48 h after an epidural blood patch which might be accompanied by neck stiffness, tinnitus, hypoacusia, photophobia, and nausea. 6 This phenomenon affects the mother to be safe to care for her newborn and breastfeed. PDPH varies based on different sociodemographic factors. Therefore, the population in this setup or this study area was not investigated before for the magnitude and possible associated factors of PDPH. So the principal aim of this study was to know the incidence of PDPH and its associated factors for parturients undergoing cesarean section under spinal anesthesia.
Methods
Study setup
Institutional-based longitudinal study was conducted on parturients who gave birth with cesarean section under spinal anesthesia in a public general hospital from 10 January to 15 June 2019. The STROBE checklist was prepared and submitted. 12
Study participants
The study was conducted on all ASA II parturients who gave birth with cesarean section under spinal anesthesia within the study period. But mothers who need general anesthesia in between the procedure, have complications like active bleeding, have pre-existing chronic or recurrent headache, and had previous diagnosis of migraine headache were excluded.
Sample size determination and sampling technique
Sample size was determined by taking the following assumption: the magnitude of PDPH is 38.8%, 11 confidence interval is 95%, and margin of error is 0.05. The sample size was determined using the following single population proportion formula

where n = sample size, Z = Z statistics for 95% level of confidence (1.96), P = prevalence of the outcome (0.388), and d = margin of sampling error to be tolerated (0.05). To get the sample size with confidence interval of 95% and margin of error 5%

Since the population is less than 10,000, a sample size was adjusted with a finite population correction formula, the final sample size was calculated as follows

where NF = the minimum sample size, n = sample size (365), and N = total number of cesarean sections done in the study area in the past 3 months retrospectively (150)

and, by adding 10% non-response rate, the final sample size was 119.
Then, systematic random sampling technique was used to select study participants on daily operations that satisfy inclusion criteria, the first participant was selected using lottery method, and then every two patient was involved from three patients.
Study variables
The dependent variable of this study was PDPH (yes/no) with the independent variable of age, educational status, residency, body mass index (BMI), number of attempts, position during spinal performance, type and size of spinal needle, type of cesarean section, previous spinal anesthesia, previous PDPH, and performer of the anesthesia.
Data collection tool and techniques
Data were collected using structured questionnaires prepared in English and then translated to Amharic. Data were collected by trained anesthetists. The participants were assessed for PDPH 2 times in the postoperative period within the first 3 days. The first visit was done at 12 h and the second was done at 72 h postoperatively. Parturients who develop positional headache within 72 h were labeled as having PDPH.
The quality of data was managed with adequate training for the data collectors and pretest was done on 5% of the populations (six participants). The daily data collection was supervised for the quality and fullness of the data.
Statistical analysis and data interpretation
The data were coded and entered into Epi Info and exported to statistical package for social sciences (SPSS) version 23. Data were summarized and presented by tables. Independent variables were analyzed using binary and multivariate logistic regression with the dependent variable PDPH. Variables with a p-value of ⩽0.2 form bivariable analysis were fitted to a multivariable logistic regression to check their association with PDPH. Adjusted odds ratio (AOR) with 95% confidence interval (CI) and p-value of ⩽0.05 were considered to determine factors which had association with PDPH.
Ethical consideration
The proposal was reviewed by the ethical reviewing committee and permission to conduct this research was obtained from the research and community service coordinator office of Debre Tabor University with the reference number of CHS/1011/2019. Written informed consent was presented and obtained from each study participant according to the principles of Helsinki declaration. Declaration of Helsinki was considered and principles and recommendations have been used.
Result
Sociodemographic characteristics of the participant
The study was conducted on a total of 119 parturients who underwent cesarean section by spinal anesthesia. In this study, the age classification was done based on the mean age of the participants and the distribution was almost equal above and below the mean value (51.3% and 48.7% respectively). Most parturients (62.2%) come from the urban area and had BMI of <35 kg/m2 (70.6%) (Table 1).
Demographic characteristics of parturients who gave birth with cesarean section under spinal anesthesia at the General Hospital, 2019.
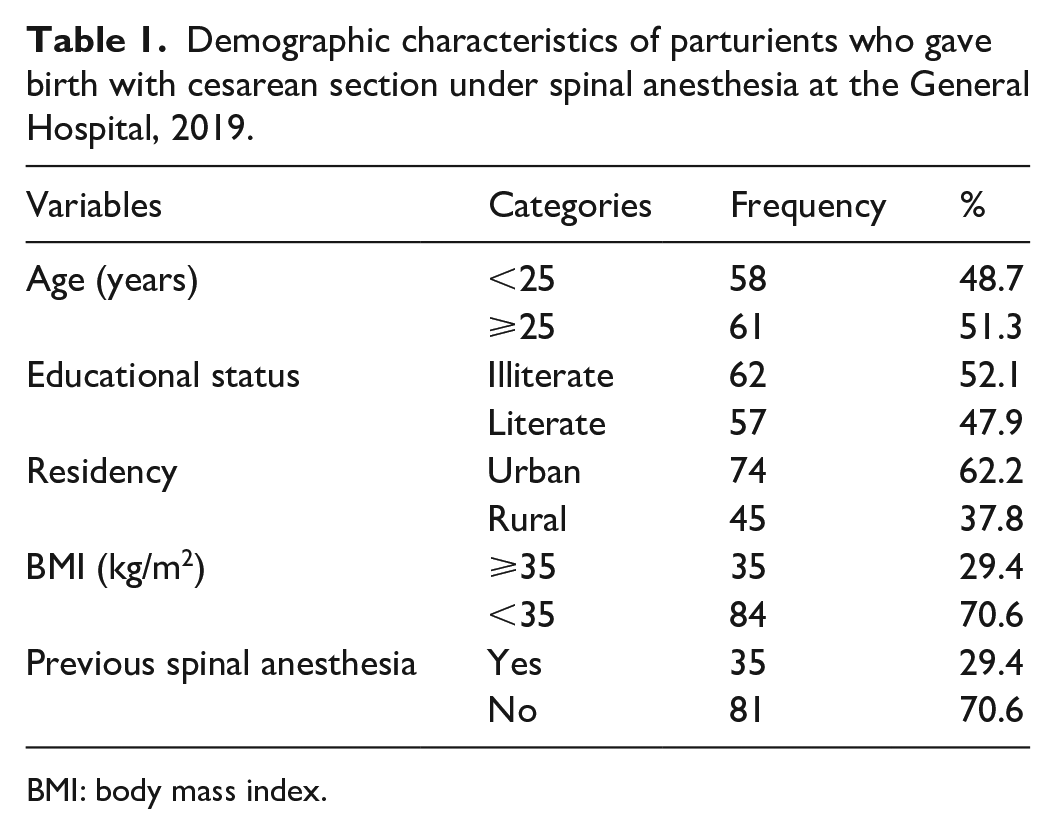
BMI: body mass index.
Clinical characteristics of the participant
A similar spinal needle type, Quincke type, was used in all participants and 24- and 25-gauge needle were used in 81.5% of them. Of those having previous spinal anesthesia (35 parturients), six (16.7%) respondents explained previous PDPH. Most cesarean sections (75.6%) were done by emergency type of operation. About 27% of the spinal anesthesia procedure was performed by qualified anesthetist, whereas the remaining was by anesthesia practitioners. About 38.7% of spinal anesthesia required repeated attempt to succeed for the planned procedure (Table 2).
Clinical- and anesthesia-related characteristics of parturients who gave birth with cesarean section under spinal anesthesia at the General Hospital, 2019.

From all participants (119), 24 respondents (20.2) developed PDPH (the outcome variable).
Factor distribution among the dependent variable (PDPH)
Factors were contributed for the occurrence of PDPH differently with variable magnitude. The chi-square test showed there was no significant difference between the groups of age, residency, BMI, type of cesarean section, and the performer of the spinal anesthesia (Table 3).
Incidence of PDPH in related with different risk factors of participants (n = 119; with χ2 test), 2019.

PDPH: postdural puncture headache; BMI: body mass index.
Factor analysis
During factor analysis, educational status, previous spinal anesthesia history, position of the mother, needle size, and number of attempts were found significant for bivariable analysis with p-value of ⩽0.2. After collinearity diagnosis, multivariable analysis was done and previous spinal anesthesia, needle size, and number of attempts were found to have significant association with PDPH with p-value of ⩽0.05 (Table 4).
Factors associated with PDPH for parturients who underwent cesarean section with spinal anesthesia at the General Hospital (multivariable logistic regression), 2019.

PDPH: postdural puncture headache; COR: crude odds ratio; CI: confidence interval; AOR: adjust odds ratio.
Discussion
PDPH is the most frequent and discomforting late complication of spinal anesthesia.6,13 This is an important cause of iatrogenic maternal comorbidity and can be a factor for maternal dissatisfaction. 14 Prolonged or severe PDPH can be complicated with cerebral venous thrombosis, subdural hematoma from traction on dural veins, seizures, hypopituitarism, syringomyelia, herniation, coma, and death. 15 It is also a principal risk factor of PDPH for the future dural puncture. This complication is most commonly resolved spontaneously and with routine simple analgesia. Caffeine and bed rest are possible strategies to manage it.16,17
The incidence of PDPH in our study was 20.2%. According to different literatures, incidence of such complication has been estimated to be quite variable, but may be approximately 10%–40% of different lumbar puncture procedures, but can be as low as 2% when ⩽24-gauge non-cutting needles are used. 15 A review article by Ebrahim Alijanpour et al. showed that the magnitude of PDPH after an intentional dural puncture ranges from 0.1% to 36% which incorporates the result of this study in this range. 10 A study done in Kasr El aini Teaching Hospital, Cairo University, found that the magnitude of PDPH was 32.8% 1 and a study in Mulago National Referral Hospital showed 48.8%. 13 These results are higher when compared with the result of this study which might be explained by difference in demographic characteristics and type and size of spinal needle. A systematic review and meta-analysis study reveal the pooled incidence of PDPH was 4.6% 10 and it was at 10.8% according to Sinikoglu et al. 18 which is much lower than this study. Study method, population, and clinical setup difference may be the possible reasons for this difference.
According to a study done by Tarekegn et al., the incidence of PDPH was 42.6%. Among those participants with PDPH, big needle sizes (AOR = 8.6; 95% CI = 0.06–0.46) and repeated number of attempts (AOR = 4.54; 95% CI = 0.52–39.14), were found to be significantly associated with PDPH on the multivariate logistic regression. This is in agreement with our study. 19
The incidence of PDPH may vary with different needle size and types.6,20–22 The use of a large caliber or cutting needle may associate with high incidence of PDPH. 15 The incidence of headache after spinal anesthesia varies greatly among the previous studies with different factors. The incidence is 40% with a 20-gauge needle, 25% with a 25-gauge needle, 2%–10% with a 26-gauge needle, and less than 2% with a 29-gauge needle.7,10 The type of needle in our study was similar, which was Quincke type with size variation between 20 and 25 gauge. In our study, the incidence of PDPH with needle size of 20 and 22 gauge and 24 and 25 gauge was 12.6% and 7.5%, respectively.
Different factors are responsible for the development of PDPH. In our study, needle size, previous spinal anesthesia history, and number of attempts were significantly associated with PDPH. Using needle size of 20 and 22 gauge was 4.2 times more risky to develop postspinal anesthesia PDPH (AOR = 4.206; 95% CI = 1.247–14.187; p = 0.021). A study done in Gondar showed that parturients who received SA using bigger spinal needles were more than 5 times more likely to develop PDPH than patients who received SA using smaller needles (AOR = 5.3, 95% CI = 1.66–16.93) which is nearly in agreement with our study. 11 According to a meta-analysis study, pencil-point needle is helpful to reduce the risk of PDPH (risk ratio (RR) = 0.33, 95% CI = 0.25–0.45). 20 A study done to compare 25- and 27-gauge needle showed that 14.5% of 25-gauge needle experienced PDPH compared with 3.2% of 27-gauge needle with statistically significant difference (p = 0.027).3,23 Another study comparing 22-, 25-, and 26-gauge spinal needles on the incidence of PDPH revealed that 33%, 4%, and 5% of the participants develop PDPH, respectively, with the overall incidence of 8.3% (p = 0.003). 24
Having previous anesthesia history was another factor which has statistically significant association with PDPH in our study. Mothers with previous spinal anesthesia were more likely to develop PDPH (AOR = 7.028; 95% CI = 2.377–20.781; p = 0.0001). Based on a study by Philo Nambooze et al., PDPH was strongly associated with history of previous spinal anesthesia (AOR = 1.3; 95% CI = 1.0–1.6; p = 0.04), 13 which is in agreement with our study.
Having repeated attempt for spinal anesthesia was around 4.7 times more likely to develop PDPH after spinal anesthesia (AOR = 4.699; 95% CI = 1.594–13.872; p = 0.05). There are different studies which agree with the findings of the recent study. Increased risk of PDPH is a disadvantage of performing a second subarachnoid injection of local anesthetics after a failed spinal anesthesia. This could be suggested with the leakage of CSF through the dural tear. 25 In agreement with our study, a study in Gondar showed that single attempts had less likely to develop PDPH (AOR = 0.22; 95% CI = 0.09–0.54). 11 Another study done in Jordan showed that repeated puncture attempt had significant association which increased the risk of PDPH by 2.55-fold (AOR = 2.55; 95% CI = 1.09–5.93; p < 0.01). 7
As the limitation, the study was conducted on small sample sizes and single center. Possible predisposing factors of PDPH such as hydration status and some comorbidity that may cause headache were not investigated. The treatment strategies and long-term complications or effects of PDPH were not studied in this study.
Conclusion
The result of our study showed that the overall incidence of PDPH was 20.2%. Needle size of 20 and 22 gauge, repeated attempt, and previous spinal anesthesia were the associated factors with the outcome variable PDPH. Therefore, it is better to perform spinal anesthesia with smaller gauge spinal needles by minimizing the number of attempts.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211051926 – Supplemental material for Incidence and associated factors of postdural puncture headache for parturients who underwent cesarean section with spinal anesthesia at Debre Tabor General Hospital, Ethiopia; 2019
Supplemental material, sj-docx-1-smo-10.1177_20503121211051926 for Incidence and associated factors of postdural puncture headache for parturients who underwent cesarean section with spinal anesthesia at Debre Tabor General Hospital, Ethiopia; 2019 by Basazinew Chekol Demilew, Aragaw Tesfaw, Alemitu Tefera, Bekalu Getnet, Keder Essa and Agazhe Aemero in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Debre Tabor University for the support. The authors’ gratitude extends to the hospital managers and unit team leaders for their cooperation during data collection. The authors would like to express their heartfelt thanks to their data collectors and friends who supported them in this research work.
Author contributions
All authors of this manuscript made a substantial contribution to the concept or design of the article, or the acquisition, analysis, or interpretation of data for the article; drafted the article or revised it critically for important intellectual content; approved the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research was conducted after we obtained ethical approval from the research and community service coordinator office of Debre Tabor University with the reference number of CHS/1011/2019.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Both verbal and written informed consent were presented and had taken from each study participant. Confidentiality was ensured by removing identifiers and locking the questionnaires after data collection in a secured area.
Availability of data
All the necessary data will be provided for reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.