
Abstract
We present a case of a 7-year-old girl with a congenital melanocytic nevus exhibiting a unique follicular pigmentation pattern. The lesion was present since birth and was largely asymptomatic. Regular dermatological follow-ups and patient education on self-screening and sun protection were recommended. This case highlights the wide-ranging morphological appearance of congenital melanocytic nevus and underscores the recommendations of monitoring for potential malignancy and addressing psychosocial impacts.
Introduction
Congenital melanocytic nevi (CMN) are benign and result from abnormal melanoblast growth during gestation, appearing between weeks 5 and 24. 1 They are present at birth or become noticeable within the first year of life. in the general population CMN are common, occurring in 1%–6% of newborns.1,2 They can vary greatly in size, texture, and appearance, and often grow proportionally with the individual. 1 These lesions may become more pigmented, raised, and coarse, with some acquiring coarse hairs.2,3 Although typically asymptomatic, they can cause pruritus, as seen in our patient. 4
Histologically, CMN are distinguished from acquired nevi by the depth of melanocyte extension, reaching deeper into the dermis, subcutaneous fat, or muscle. 5 CMN are classified by size: small (<1.5 cm), medium (1.5–19.9 cm), and giant (>20 cm). 6 While most CMN are benign, larger lesions have a higher risk of malignant transformation into melanoma. The estimated risk of melanoma is <1% in small and medium CMN, but ~5% in giant CMN. 2 Due to this risk, it is important to be aware of the various morphological appearances of CMN. This included the less common morphologies such as our patients follicular-based pigmentation pattern.
Case report
A 7-year-old girl with an unremarkable past medical history was evaluated for a significant pigmented plaque on her left thigh. The lesion was present since birth and had increased in size in proportion to her growth. The patient reported that the lesion had become thicker and rougher but was largely asymptomatic, with mild intermittent pruritus. There was no family history of similar lesions or cutaneous malignancy.
On physical examination, the lesion was identified as a well-defined, dark brown plaque measuring 14 × 4 cm. It consisted of multiple grouped pigmented follicular papules with occasional terminal hairs and a rim of light brown papules at the edge. Dermoscopy revealed homogeneous follicular brown pigmentation with a reticular network. No other concerning lesions were noted.
Discussion
Our patient’s CMN displayed a rare follicular-based pigmentation pattern, differing from the more commonly observed perifollicular hypopigmentation. 7 The presence of follicular papules is less typical but highlights the variability in CMN presentations to be aware of when assessing pigmented lesions.
Management of CMN depends on lesion characteristics, including size, location, and cosmetic considerations. Options include observation, dermabrasion, laser ablation, and surgical excision. 1 Smaller nevi are often monitored, while more aggressive treatments such as surgery are reserved or larger CMN. Regular dermatological screenings and self-surveillance are generally recommended for larger lesions. Clinicians should also be aware that CMN can have significant psychosocial impacts, particularly for individuals with larger nevi or those located in visible areas such as the face. 8 It is important to be aware and sensitive of these factors when assessing patients, especially in a pediatric population. For our patient, we advised annual dermatological evaluations, self-screening, photoprotection, and monitoring for changes suggestive of malignancy. Additionally, we recommended topical medium-potency steroids and moisturization to manage pruritus.
This case illustrates a rare variant of congenital melanocytic nevus with follicular pigmentation. While CMN are generally benign, they require careful monitoring to detect potential malignant changes. Early detection, regular follow-ups, and appropriate management are crucial in addressing the potential for melanoma and the psychosocial impact of CMN (Figures 1 and 2).

Photograph of CMN on the left medial thigh taken at most recent visit.
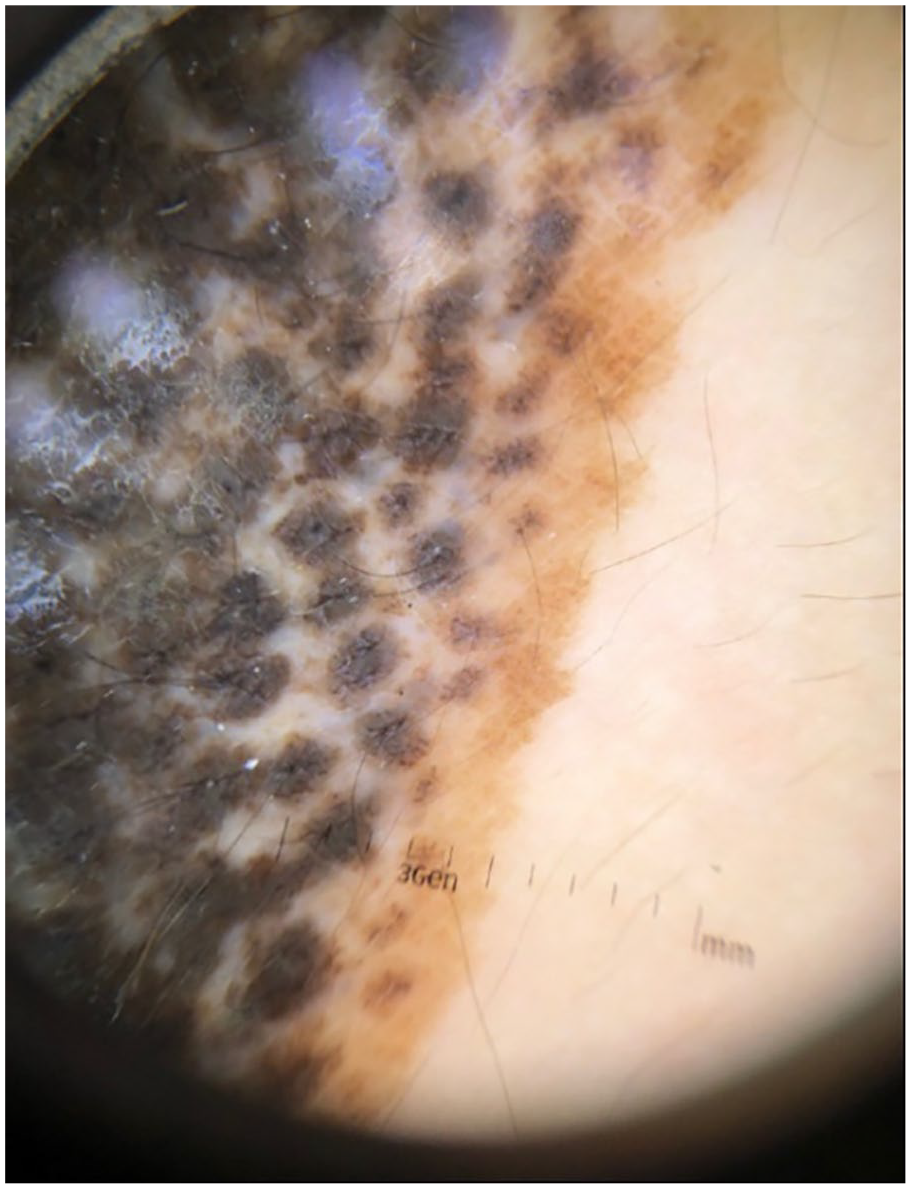
Dermoscopic photograph of the edge of the patients CMN.
Footnotes
Consent for publication
The authors obtained written consent from patients for their photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.