
Abstract
Porokeratosis is a condition characterized by abnormal epidermal keratinization with a unique morphology of papules or plaques surrounded by a thread-like border of scale corresponding to the cornoid lamella on histology. Many established subtypes have been described; however, genitogluteal porokeratosis is a rare entity. We present the case of a 58-year-old male with pruritic reddish lesions affecting the genitals and thighs, diagnosed with genital porokeratosis. This case highlights features of this rare and diagnostically challenging subtype of porokeratosis.
Introduction
Porokeratosis (PK) is an idiopathic disorder caused by abnormal clones of epidermal keratinocytes that can be acquired or hereditary.1,2 Clinically, PK presents as reddish papules and annular plaques with thread-like elevated scaly borders that correspond to cornoid lamellae on histology. 2 Cornoid lamellae can be sparse and difficult to detect, or multiple. 1 The course is unpredictable, and lesions can enlarge centrifugally. 3 Risk factors for the development of PK include genetic predisposition, ultraviolet light exposure, immunosuppression, internal malignancy, and skin trauma though many cases are sporadic.3–5 Many subtypes of PK exist, with some being very rare. It is unusual, but possible, to manifest more than one type. 6 The more established types of PK include classic plaque PK of Mibelli, disseminated superficial actinic PK, disseminated superficial nonactinic PK, linear PK, and palmoplantar/punctate PK. 7 Involvement of the genital and adjacent areas (buttocks, perineum, groin, and proximal thighs) can be part of generalized PK2,8 occurring elsewhere on the body, but isolated genitogluteal PK is rare.
Case report
A 58-year-old male was referred to Dermatology for evaluation of pruritic keratotic reddish lesions affecting the medial thighs, penis, scrotum, and hips for the last 4 years. The patient described irritation of these lesions with heat and sweating. He had previously been treated for presumed recurrent intertrigo/inguinal candidiasis in the context of his diabetes and recent empagliflozin use; however, he experienced no improvement with oral fluconazole and topical clotrimazole/betamethasone dipropionate. Otherwise, the patient had a past medical history of hypertension, and dyslipidemia. His medications included metformin, semaglutide, insulin degludec, and rosuvastatin.
On examination, many dull-red warty papules were seen on the mons pubis, penis, scrotum, pubis, groin, and thighs, some displaying thin rims of scale at the periphery (Figure 1). A skin biopsy was performed and showed epidermal acanthosis with several mounds of parakeratosis typical of cornoid lamellae (Figure 2). Additionally, nonspecific lymphocytic infiltrate in the adjacent dermis with occasional eosinophils was observed. Given the clinical presentation and histopathology, he was diagnosed with the rare entity of genital porokeratosis. Some of the larger, more irritated lesions were treated with liquid nitrogen cryotherapy. He was also treated with a pathogenesis-targeted treatment through use of compounded topical 2% lovastatin/2% cholesterol ointment and cream. With daily applications of these compounds, he has noticed a considerable difference in the height of his lesions as well as a reduction of his symptoms including itch and irritation.

Dull-red warty papules seen on the mons pubis, penis, scrotum, and thighs, some displaying thin rims of scale at the periphery.
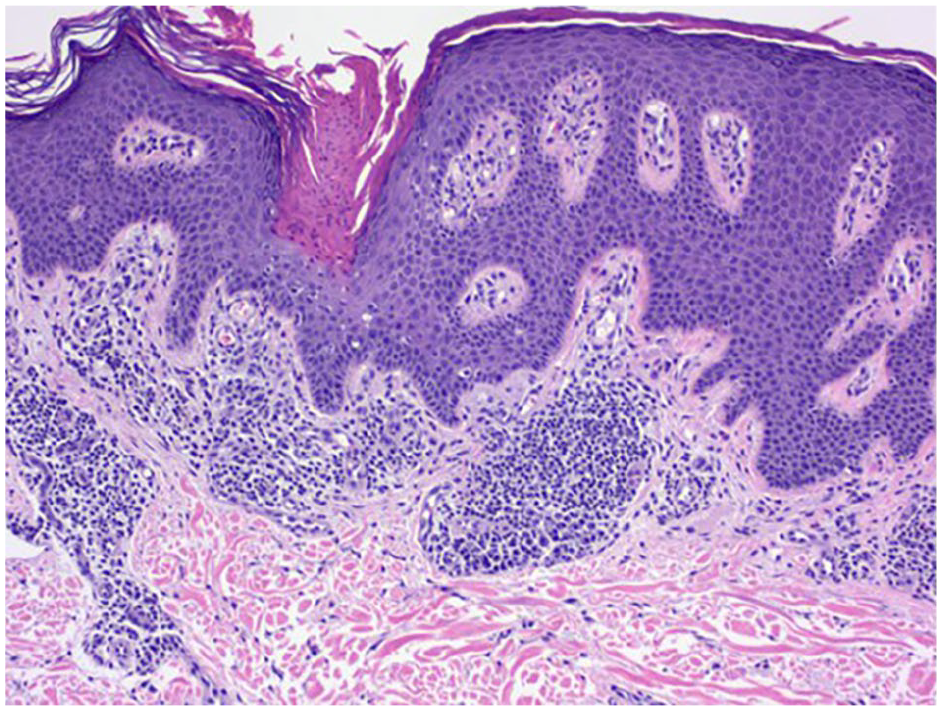
Histology sample demonstrating epidermal acanthosis and mounds of parakeratosis typical of cornoid lamellae seen in porokeratosis.
Discussion
Here, we present a rare case of genital porokeratosis. Since it was originally described by Helfman and Poulos in 1985, 9 more than 50 reports of isolated genitogluteal PK have been published, most of which have been in men. 6 The terminology of this group can be fluid and confusing, with overlapping features making distinction difficult. Nevertheless, three other subtypes of genitogluteal PK have been mentioned including Mibelli PK in the genital region, ptychotropic PK, and penoscrotal PK. 6
In our case, the patient had findings most in keeping with a diagnosis of classic Mibelli PK in the genital region. This subtype remains a rare entity, with diverse phenotypes. 6 Most patients are middle-aged males who have had lesions for more than a year prior to diagnosis and is exceedingly rare in women.4,6 The mean age at initial diagnosis is 39 years. 6 Most common sites include the scrotum, penis, buttocks, and adjacent thighs. Cornoid lamellae seems to be less apparent in this variant. 6
Ptychotropic PK was initially described by Lucker et al. in 1995. 10 The term is derived from the Greek ptyche (fold) and trope (turning), highlighting the flexural location of the lesion. 10 Most cases are itchy, symmetric, verrucoid, lichenified plaques in the natal cleft and it has also been termed “perianal inflammatory verrucous porokeratosis.” 11 The lesions typically lack the classic thread-like border, leading to misdiagnosis as condylomas, inverse psoriasis, and lichen simplex chronicus.6,11 Ironically, histology tends to show multiple cornoid lamellae and in rare cases, 6 amyloid deposits have been found on histology in the upper dermis. 12
The penoscrotal PK variant has been reported to affect men in their third decade and presents as poorly defined plaques on the ventral surfaces of the penile shaft and anterior scrotum associated with severe pruritus and burning sensation.13,14 Histology differs from other genitogluteal PK subtypes and has shown multiple adjacent cornoid lamellae arising from follicular or eccrine structures.13,14
The pathogenesis of porokeratosis is thought to involve mevalonate pathway gene mutations whereby the end-product is cholesterol. 15 Decreased levels of cholesterol are thought to increase apoptosis of keratinocytes, a phenomenon that has been observed in many types of PK. 15 Accumulation of toxic metabolites from the mevalonate pathway are also thought to play a role. 15 More recent discoveries into the role of this pathway and genetics have helped direct treatments to more pathogenesis- and mechanism-directed approaches such as compounded lovastatin and cholesterol with promising results, as seen in this case. 15
Most subtypes of PK have been associated with malignant transformation leading to the formation of skin cancers such as squamous cell carcinomas, basal cell carcinomas, and rarely melanomas.4,15 Large, linear, and long-standing PK lesions are associated with a higher risk of malignancy. 15 Despite these findings, malignant change has not been reported in genitogluteal PK 4 but remains a theoretical concern; therefore, regular follow-up is recommended. Finally, it is important to consider genital PK in the differential diagnosis for keratotic plaques and papules isolated to the genitogluteal region as misdiagnosis can lead to inappropriate treatment and inadequate follow-up.
Footnotes
Acknowledgements
The authors would like to thank Dr. Quentin Nakonechny for his contributions to the histology images and pathology report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The patient provided informed consent for publication of the case report and images.