
Abstract
Linear porokeratosis is a rare variant of porokeratosis that most often presents in newborns and children; development of this porokeratosis variant in adulthood is far less common. We report the case of a 25-year-old female who presented with a progressive eruption on the proximal upper extremity of 6-year duration, which was ultimately diagnosed as adult-onset linear porokeratosis and safely treated with oral isotretinoin. We propose that a sporadic mutation resulting in mosaicism after birth may explain the development of linear porokeratosis in adulthood, although the exact trigger of such a somatic mutation is not known. This case also describes a unique clinical presentation, with linear porokeratosis lesions originating on the proximal extremity rather than on the more common distal extremity. This demonstrates a distinctive clinical presentation not seen in the pediatric forms of disease.
Introduction
Linear porokeratosis is a rare variant of porokeratosis that presents with raised, cornoid lamellae identical to the Mibelli morphology but in a unique unilateral distribution, often following the lines of Blaschko. Linear porokeratosis is thought to be due to inherited forms of mosaicism during embryogenesis; therefore, this disease most often presents in newborns and children. Development of this porokeratosis variant in adulthood is far less common. We report a 25-year-old female who presented with a progressive eruption on the proximal upper extremity of 6-year duration, which was ultimately diagnosed as adult-onset linear porokeratosis and safely treated with oral isotretinoin. Furthermore, we review the likely genetic causes of this rare presentation and present management options.
Case presentation
A healthy 25-year-old female presented with a pruritic eruption on the right upper extremity of 6-year duration. There was no disease in childhood. The lesions appeared to follow lines of Blaschko, with progression to the shoulder and mid-scapula during 5 months of observation (Figure 1(a) and (b)). The patient described worsening of symptoms with sun exposure. Physical examination was significant for linear, scaly, clustered plaques involving the right proximal upper extremity, shoulder, and upper back. The remainder of her examination was normal. No acantholysis was noted. The differential diagnosis included inflammatory linear verrucous epidermal nevus (ILVEN), lichen striatus, linear keratosis follicularis (Darier disease), linear lichen planus, and porokeratotic eccrine ostial and dermal duct nevus (PEODDN). Syndromes such as craniosynostosis–anal anomalies–porokeratosis (CDAGS) were also considered in the differential diagnosis. 1
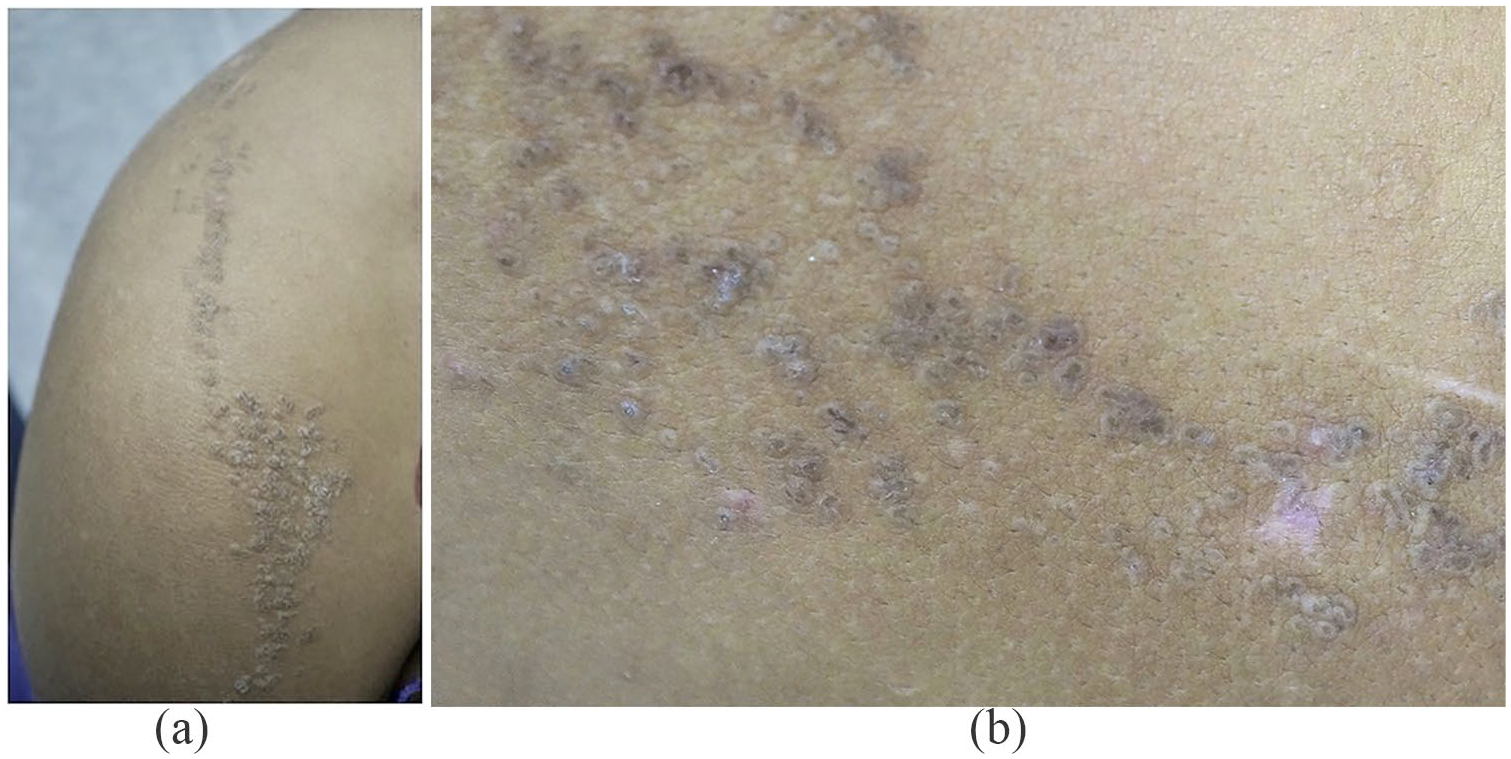
(a) Clinical photograph. Hyperpigmented papules coalescing into plaques surrounded by distinctive keratotic ridges may be appreciated in a linear distribution on the right upper extremity and shoulder. (b) Clinical photograph. Keratotic ridges with central grooves are evident on closer examination.
A skin biopsy revealed distinctive cornoid lamellae comprising thin, columnar, closely stacked, parakeratotic cells extending through the stratum corneum with a minimal granular layer (Figure 2). A diagnosis of linear porokeratosis was established based on clinical and histologic features. A therapeutic trial of isotretinoin 1.5 mg/kg for 24 weeks (6 months) and 1.7 mg/kg for 8 weeks (2 months) resulted in dramatic regression of hyperkeratotic changes, although mild local hyperpigmentation remained at the 2-month follow-up (Figure 3). The patient provided informed consent to publish her unique case findings.

Hematoxylin and eosin stain, original magnification. Keratin-filled epidermal invaginations with angulated, parakeratotic tiers (cornoid lamellae) can be appreciated.

Clinical photograph. Dramatic regression of hyperkeratosis was noted at the 2-month follow-up visit, although mild local hyperpigmentation remained.
Discussion
Porokeratosis is a disorder of keratinization, due to aberrant terminal differentiation of keratinocytes with unique clinically raised margins, called cornoid lamellae. 2 Porokeratosis is histologically characterized by parakeratotic cells within central grooves of the epidermis, called cornoid lamellae. Numerous variants of porokeratosis have been described, including classic porokeratosis of Mibelli, disseminated superficial (actinic) porokeratosis, porokeratosis palmaris et plantaris disseminata, punctate porokeratosis, and linear porokeratosis. 3 Linear porokeratosis is a rare, unilateral variant that most often presents with small, hyperpigmented, brown, keratotic papules that slowly enlarge to form irregular annular plaques with well-demarcated, raised borders. 4 The center of the lesions may be anhidrotic with alopecia. 5 Linear porokeratosis most often presents on the trunk and distal extremities, in a segmental pattern following the lines of Blaschko. 4 The current case highlights a rare presentation of linear porokeratosis involving the proximal right upper extremity.
The etiology of this porokeratosis variant appears to be manifold. Linear porokeratosis is thought to develop as a nonhereditary trait; however, it has been reported to occur in families with disseminated superficial actinic porokeratosis (DSAP). 6 Because of the few familial reports of linear porokeratosis overlapping with DSAP, a genetic variant in chromosome 12, 15, or 18 has been postulated. 7 Somatic recombination of the DSAP locus in early embryonic development may result in an abnormal precursor clonal cell, which subsequently grows in a linear fashion. 8 A sporadic mutation resulting in mosaicism could explain the development of linear porokeratosis in adulthood. Other genetic variants have also been associated with the development of linear porokeratosis. For example, one study found an overexpression of p16 (INK4a) protein, a cyclin-dependent kinase inhibitor in patients with congenital, unilateral linear porokeratosis. 9 The exact triggers responsible for sporadic somatic mutations likely underlying adult-onset linear porokeratosis remain unknown, but ultraviolet radiation, herpes simplex virus infection, and hepatitis C infection have been reported to elicit the onset of other porokeratosis variants. 10
Treatment options include topical 5-fluorouracil, topical calcipotriene, cryotherapy, surgical excision, as well as topical and oral retinoids. While numerous treatments have been used, recent studies suggest topical and systemic retinoids are the most efficacious agents. 11 Proper diagnosis and management is crucial, as ultraviolet exposure and immune suppression are reported to worsen symptoms or promote subsequent development of malignant transformation in these lesions. Squamous cell carcinoma in particular has been reported in cases of linear porokeratosis as well as other variants. 12
In summary, we report a rare case of new-onset linear porokeratosis presenting in an adult and safely treated with isotretinoin. We describe a unique clinical presentation, with linear porokeratosis lesions originating on the proximal extremity rather than on the more common distal extremity. Further studies are necessary to characterize the underlying genetic etiology of linear porokeratosis developing beyond infancy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient gave consent for use of her case for presentation in this manuscript.
Prior presentation
The authors have not presented this work elsewhere.