
Abstract
Edentulous patients with history of cleft palate and severe maxillary atrophy are challenging patients to rehabilitate through an oral approach. The difficulty of rehabilitating these patients lies in the unusual anatomy they present and the alteration of the vascular supply of local tissues caused by the previous performed surgeries, along with other causes. This report describes the successful dental rehabilitation with zygomatic implants of a patient with complete bilateral cleft palate who was edentulous and had severe maxillary atrophy.
Introduction
Cleft lip and palate is the most frequent craniofacial malformation in the world, with an incidence of 1:700 live births in Europe. 1 The origin of this malformation is unknown, with a genetic influence described in one-third of the cases. However, it is suspected that the majority of cases may have external agents that could be associated with the development of this malformation. 2 Although many risk factors that predispose to its development are described, such as drugs or infections, this cause–effect relationship is not clear. 3 Cleft lip and palate can affect the upper lip, nose, alveolar process, hard and soft palate in a variable way, from exclusively involving the lip or the uvula, to its complete form with the ful fissure of the lip and the palate (unilateral or bilateral). 4
Zygomatic implants are 30–52.2 mm long threaded implants that go from the alveolar process to the malar bone. Initially, they were developed for dental rehabilitation in oncological patients undergoing large maxillary resections who had sufficient remaining malar bone. 5
Due to its success, they began to be used in cases with severe unilateral or bilateral maxillary atrophy which made the placement of conventional implants impossible.6,7
Patients with bilateral cleft lip and palate, very frequently present significant bone defects in the alveolar process, either due to the cleft itself that causes a defect in the premaxilla, or due to failure of the bone graft in the alveolar fissure 8 ; in fact cleft patients have unpredictable results in bone graft treatments due to their vascular alterations in the upper jaw. 9 In addition, adult patients frequently present reabsorbed premaxilla, usually due to the lack of care of their oral cavity by the appropriate specialists, which are the reason why we usually find a large part of these patients with resorbed jaws and large scarring sequelae. Therefore, these patients are not good candidates for bone grafting due to already disrupted local vascularity, poor tissue elasticity, and compromised oral opening. 10 Consequently, due to the incapacity for oral rehabilitation with conventional implants, the proposal for zygomatic implants is an excellent alternative.11–13
There are very few reports in the literature regarding patients with cleft lip and palate who have undergone zygomatic implant surgery for oral rehabilitation. Some studies describe the application of zygomatic implants in cases involving compromised maxillae, 14 such as those following maxillectomy. The aim of this case study was to report the outcomes of zygomatic implant insertion without any graft placement for the aesthetic and functional oral rehabilitation of a patient with bilateral cleft lip and palate and a severely atrophic maxilla.
Case report
Fifty-one-year-old white male was referred to our Oral and Maxillofacial Surgery unit in 2016 due to difficulty in eating. He had undergone several surgical procedures because of complete bilateral cleft lip and palate during childhood including a tongue flap for close a big palate fistula. He has paranoid schizophrenia and was a smoker of 1 pack/day.
The patient presented with severe maxillary hypoplasia that caused a skeletal class III with anterior crossbite. Advanced periodontal disease in both upper and lower dentition and partial edentulism in the first maxillary quadrant were present. He wore a removable upper and lower partial denture and he showed a short upper lip and absence of upper vestibule. Likewise, as a sequel to the intervention of the palatal fissure, he presented a midline oronasal fistula (Figure 1).

Oronasal fistulae, and its correction with prosthesis after surgery, resulting in improved vocal function and preventing the passage of fluids from the mouth to the nasal cavity.
Panoramic radiography and computed tomography (CT) scan were performed prior to placing the implants, which showed severe atrophy of the upper jaw, significant oroantral communication, and partial absence of the premaxilla (Figure 2).
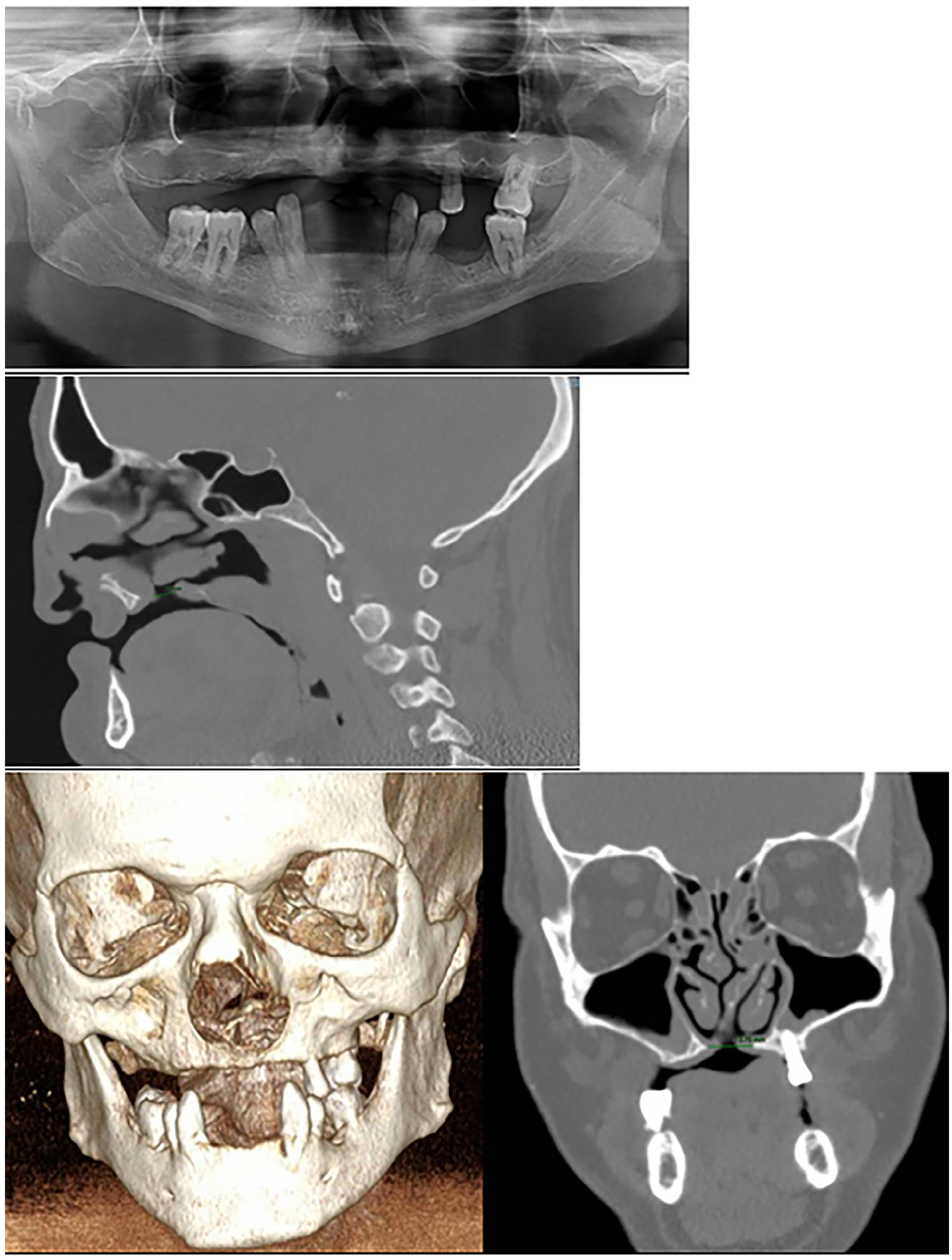
Panoramic radiography and CT scan were performed prior to placing the implants, which showed severe atrophy of the upper jaw, significant oroantral communication, and partial absence of the premaxilla.
We decided to perform a superior vestibuloplasty at first with a second time, 6 months later, placement of zygomatic implants to rehabilitate the patient. We placed four zygomatic implants according to ZAGA technique,15–17 enough to safely support a fixed prosthesis. The zygomatic implants were then positioned with an extraoral screwdriver. Further details on this technique can be found in a previous publication by Goker et al. or Aparicio et al. As required by this technique, 17 a CT scan was obtained to study the anatomy of the sinus and the alveolar crest to determine the optimal placement of the zygomatic implants (Figure 3). The patient decided not to use a provisional prosthesis until a definitive prosthesis was made. After 6 months, final metal-ceramic prosthesis was delivered. The patient decided to use a lower removable partial denture once the maxilla was rehabilitated. The lower teeth were managed periodontally.

CT imaging in the coronal perspective is essential for planning zygomatic surgery using the ZAGA technique, as it allows for precise determination of implant entry points to avoid the maxillary sinus.
A panoramic radiograph was obtained postoperatively (Figure 4). A CT scan was performed 6 months after the surgery (Figure 5) to evaluate the integration of the implants and the condition of the maxillary sinus, and after that, a new panoramic radiograph was obtained with the definitive prosthesis (Figure 6). The patient was recalled for clinical follow-up after 1 month and every 3 months for the first year, and then twice a year. To this day, the patient presents a good result functionally and aesthetically. No complications such as sinusitis, difficulty in hygiene maintenance, speech impairment, or mobility of the implants were detected. Masticatory function was restored, and the patient was satisfied with his appearance (Figure 7). Follow-ups are performed periodically. Currently, after 5 years, the situation of the implants is very good, despite poor maintenance by the patient (Figure 8).
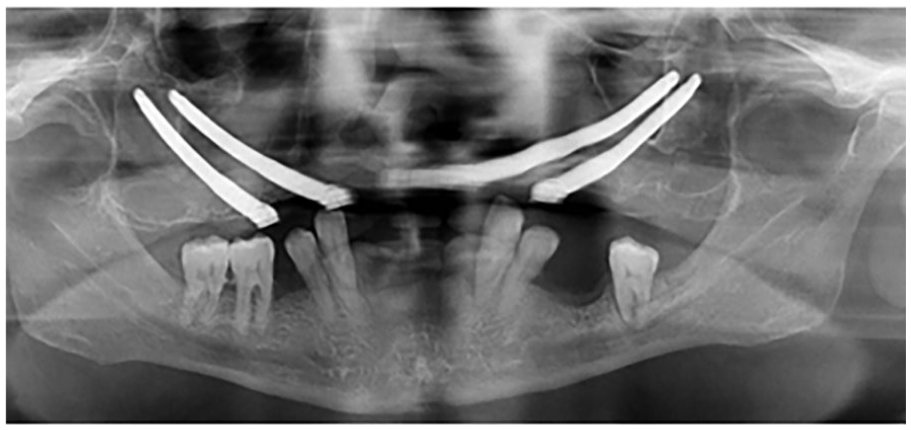
A panoramic radiography was performed postoperatively.

A CT scan was performed 6 months after surgery to assess the implants and the health of the sinus before proceeding with the definitive prosthesis.

Panoramic radiography at 6 months with definitive prosthesis.

The patient was satisfied with his appearance.

The current prosthesis and oral condition of the patient show healthy gums and implants, despite poor hygiene and inadequate patient care. This indicates that, despite suboptimal maintenance, the implants remain stable.
Discussion
Edentulous patients with history of cleft lip and palate and severe maxillary atrophy are challenging patients to rehabilitate through an oral approach. In this case, we have verified that dental rehabilitation with zygomatic implants was the best option since it could not be rehabilitated in any other way. Zygomatic implant surgery is a valid and successful option to grafting procedures in the rehabilitation of edentulous atrophic maxilla due to degeneration, malformation or oncological causes. 12
Initially, due to the multiple scar sequelae such as synechiae and adhesions after previous interventions, it was necessary to create a non-existent vestibule where the prosthesis could be carried afterwards. Besides, this patient was not a good candidate for rehabilitation with bone grafting due to the poor vascularization of the scarred tissue and the presence of an oroantral communication which would make the bone graft technique fail. 9 In fact, zygomatic implants were designed to avoid grafts in the atrophic jaws, initially used in oncological and large trauma patients who exclusively present a remnant of malar bone 5 and later introduced in cases of atrophic jaws of other nature, obtaining very good results. 18
Multiple studies demonstrate that the use of zygomatic implants is safe and yields very good long-term results,19,20 although outcomes are highly dependent on the surgeon’s experience. However, we contend that surgeons who are willing to treat patients of this complexity—often due to a history of multiple surgeries and various sequelae—are typically experts in managing complex cases and their treatments. Although recent publications have begun to outline guide zygomatic implant approach,21,22 the need for experienced surgeons remains paramount, as few cases have been described and further improvements to the technique are still necessary.
When considering using zygomatic implants as the rehabilitation method in a patient, we must bear in mind that this is a technique with difficult reversibility, so there are other alternatives we should also first consider like using a removable prosthesis or perform bone regeneration techniques to place convencional implants. In this specific case, the patient did not have many more options due to the limited basal bone availability and the scarring sequelae in the upper jaw. In addition to the lack of other options, the future use of a hybrid prosthesis, which zygomatic implants will require, improves the obturation of the oronasal fistula. This way we also treat a complication that contraindicated both the use of conventional implants and reconstruction with bone grafts because they both need a watertight seal. 23
In this case, the use of a removable prosthesis was also rejected as a treatment option due to his lip deficiency and his shortage of vestibule, despite having increased it with a previous vestibuloplasty. He was neither a candidate for an overdenture which also required the placement of conventional implants as well as the need for bone regeneration with bone grafts previously ruled out. 23
For all these reasons, and given the good results obtained from both a functional and aesthetic point of view, we believe that the option chosen in this patient is the ideal one.
Conclusion
The use of zygomatic implants in the rehabilitation of the atrophied maxilla seems to provide an excellent support to dental rehabilitation, both functionally and aesthetically, in patients with facial deformities and especially in this particular type of patient with cleft lip and palate who has undergone many previous surgeries on their maxilla. Despite the challenges presented by a patient with hygiene deficiencies and unique anatomical and vascular considerations, zygomatic implants have proven to be a reliable and stable system over the years, even in extreme cases such as this.
We are aware of the limitations of the case: the patient’s mental illness and his microstomia did not allow us to use splints to carry out guided surgery or carry out immediate loading in prosthetic rehabilitation. Additionally, the implants were inserted 5 years ago, at a time when guided surgery for implants was not sufficiently developed for zygomatic implant cases. Even today, this technique remains novel, with limited experience and ongoing development.21,22
Footnotes
Acknowledgements
The authors thank Department of Oral and Maxillofacial Surgery, Hospital Puerta del Mar, Cádiz.
Author contributions
T.C.-M.: conceptualization, methodology, and supervision of the study; performed the surgical procedures and contributed to the writing of the manuscript; literature review. M.C.: data collection, analysis, and interpretation; prepared the figures and tables; assisted in the writing and revision of the manuscript. A.S.-S.: translated the paper. M.C.-Z.: writing the initial draft of the manuscript and editing for language and content; provided critical revisions and final revision and approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.