
Abstract
Background and objective:
This study focuses on children aged 8–12 with cleft lip and palate, a critical period for surgical and orthodontic interventions that can significantly impact facial development and psychosocial well-being. Assessing the satisfaction and quality of life of patients and their parents during this stage can provide valuable insights to optimize care and support outcomes.
Methods:
A cross-sectional study was conducted among parents and 32 patients with unilateral and bilateral complete cleft lip and palate who received continuous treatment at the Tawanchai Center during the year 2024. Data were collected using a general information questionnaire, the THAICLEFT quality of life Questionnaire, and a patient self-assessment. Data were analyzed using descriptive statistics, including percentage, mean, and standard deviation. Psychosocial satisfaction was compared using the Mann–Whitney U test.
Results:
Among 32 participants, patients (68.75% male, mean age 10.38 ± 1.52 years) with predominantly unilateral cleft lip and palate (68.75%) reported high satisfaction across five psychosocial domains (mean 4.00 ± 1.26). Parents reported highest satisfaction with service quality (4.65 ± 0.52) and moderate-to-high satisfaction across medical, cost, and psychosocial domains (means 3.54–4.21). Family impact remained low (2.25 ± 1.71). Communication ability showed significant between group differences (p = 0.02).
Conclusion:
Parents reported high satisfaction in three domains, while patients showed high satisfaction in five psychosocial aspects. The findings from this study will be used to improve patient and family care, enhancing their overall quality of life.
Introduction
Cleft lip and palate (CLP) is a congenital condition characterized by a cleft in the upper lip, which may extend to the nose or the anterior palate in some cases. The primary causes are multifactorial, involving both genetic and environmental factors. 1 This condition can lead to difficulties with sucking, speaking, swallowing, and dental occlusion. Additionally, the distinct facial appearance can impact the patient’s physical, psychological, social, and economic well-being, affecting both the family’s quality of life (QoL) and the country’s overall societal welfare.2,3 The incidence of CLP is highest in Northeastern Thailand, with a rate of 2.28 cases per 1000 live births, which exceed the national average of 2.14 cases per 1000 live births. 4
The treatment of patients with CLP requires a multidisciplinary team to provide comprehensive care. Surgical interventions and rehabilitation are age-specific and require long-term follow-up, from infancy through adulthood, around the age of 20. Each stage of development involves different treatment priorities. For instance, from birth to age 5, the focus is on feeding, nutrition, and primary surgery. Between the ages of 8 and 12, treatment emphasizes oral preparation, alveolar bone grafting, and orthodontic care. By the ages of 16–20, the treatment focuses on the completion of orthodontic care, corrective surgery for residual deformities, and quality-of-life assessments. The World Health Organization (WHO) has recommended evaluating the QoL in CLP patients at three key age groups: 4–6, 8–12, and 16–20 years.5 –7 The findings from these evaluations can guide improvements in patient care, ensuring effective treatment outcomes, increased satisfaction, and better overall QoL. This study specifically focuses on children aged 8–12, known as middle childhood, which marks a period of structured learning. During this stage, children develop advanced social interactions with peers, show greater interest in physical activities, and begin to think more logically, concretely, and mathematically. 8
A review of the literature on QoL reveals three primary dimensions: (1) physical health, (2) psychological health, and (3) social health. 9 This comprehensive understanding is essential when evaluating the impact of chronic pediatric conditions, such as cleft lip and/or palate (CLP), on the parents or caregivers responsible for the child’s care. Parents of children with CLP often experience increased emotional stress, financial strain, social isolation, and disruptions to daily functioning, which can significantly influence their satisfaction with life and caregiving. 10 The burden of managing medical appointments, surgical procedures, and psychosocial challenges often affects parental well-being and their perceived QoL. WHO has developed a tool specifically designed to assess the QoL of children with CLP in the Thai context, known as the THAICLEFT QoL for children with CLP and their families.5,6
The Tawanchai Center, in collaboration with the Faculty of Medicine and the Faculty of Dentistry at Khon Kaen University, serves as a central hub for providing comprehensive care, including treatment, surgery, and rehabilitation for CLP patients. The center also focuses on developing care protocols, conducting research, and supporting affected families to improve their QoL. 7 The center employs nurse coordinators who provide counseling and oversee physical, psychological, psychosocial, and socioeconomic care. These nurses coordinate individualized case management, starting from the prenatal stage through childbirth and continuing until the completion of treatment around the age of 20. Quality-of-life assessments are fundamental to nursing care, particularly for children aged 8–12 with unilateral or bilateral complete clefts, as these conditions significantly impact patients well-being.
Therefore, this study aims to assess satisfaction with CLP care among patients and their parents at a specialized treatment center in northeastern Thailand. The findings will guide future improvements in patient care and overall QoL for both patients and their families.
Methods
This cross-sectional study was conducted among parents and children aged 8–12 years with complete unilateral or bilateral CLP receiving treatment at the Tawanchai Center, Faculty of Medicine, and Faculty of Dentistry, Khon Kaen University, Thailand, in 2024. A purposive sampling method was used to select 32 participants who were in continuous follow-up care during the alveolar bone graft preparation phase.
The population consisted of 292 patients receiving services at the Tawanchai Center in 2024. The sample size was calculated based on the standard deviation of overall QoL and self-image in 10-year-old CLP patients
11
(SD = 1.39), with Zα/2 = 1.96 and d 0.45, N = 292. The sample size calculation formula for this study is
The sample size calculated for this study is 32 participants.
Inclusion criteria
Patients aged 8–12 years with unilateral or bilateral complete CLP who received continuous treatment at the Tawanchai Center during the year 2024.
Exclusion criteria
Patients with any type of comorbid condition, such as heart disease, Pierre Robin Sequence (PRS), or Down syndrome.
Research tool
The research tool consisted of three components: a General Information Questionnaire, the THAICLEFT QoL Questionnaire, and a patient self-assessment. The THAICLEFT QoL Questionnaire was developed in Thailand to specifically assess the QoL in individuals with cleft lip and/or palate (CLP) within the Thai cultural context.5,6 It has demonstrated good internal consistency, with a Cronbach’s alpha of 0.861. Completed by parents or guardians, the questionnaire includes 49 items covering five dimensions: (1) medical care, (2) service delivery, (3) medical expenses, (4) psychosocial aspect, and (5) family impact. The Patient Self-Assessment, completed by the 32 patients themselves, consisted of questions derived from the psychosocial aspect of the THAICLEFT QoL Questionnaire. The average completion time was approximately 20 minutes. Each item was rated using a 5-point Likert-type scale, 12 where 1 indicated the lowest level of satisfaction and 5 indicated the highest.
Score interpretation criteria:
1.00–1.49: Very low satisfaction
1.50–2.49: Low satisfaction
2.50–3.49: Moderate satisfaction
3.50–4.49: High satisfaction
4.50–5.00: Very high satisfaction
Data analysis
Data analysis was conducted to assess both general information and QoL using descriptive statistics, such as percentages, means, and standard deviations. To compare satisfaction levels between groups, the Mann–Whitney U test was employed, providing a nonparametric method suitable for evaluating differences in ordinal data or data that does not follow a normal distribution.
Ethical considerations:
This study was approved by the Khon Kaen University Ethics Committee for Human Research (Approval No. HE671291).
Results
The general characteristics of the patients in the study showed that the majority, 22 individuals (68.75%), were male. The average age of the patients was 10.38 years, with a standard deviation of ±1.52 years. Most patients, again 22 (68.75%), presented with unilateral CLP. Regarding surgical history, 11 patients (34.38%) had undergone alveolar bone grafting. In terms of caregiving, 23 patients (71.88%) were primarily cared for by their parents. The educational background of caregivers revealed that 18 (56.24%) had attained only a primary level of education. Notably, 30 patients (93.75%) were covered under the Universal Coverage Scheme or the “Yim Suay Saing Sai Project,” reflecting broad access to healthcare support within this group (Table 1).
General information of patients with CLP (ages 8–12) and their caregivers (n = 32).
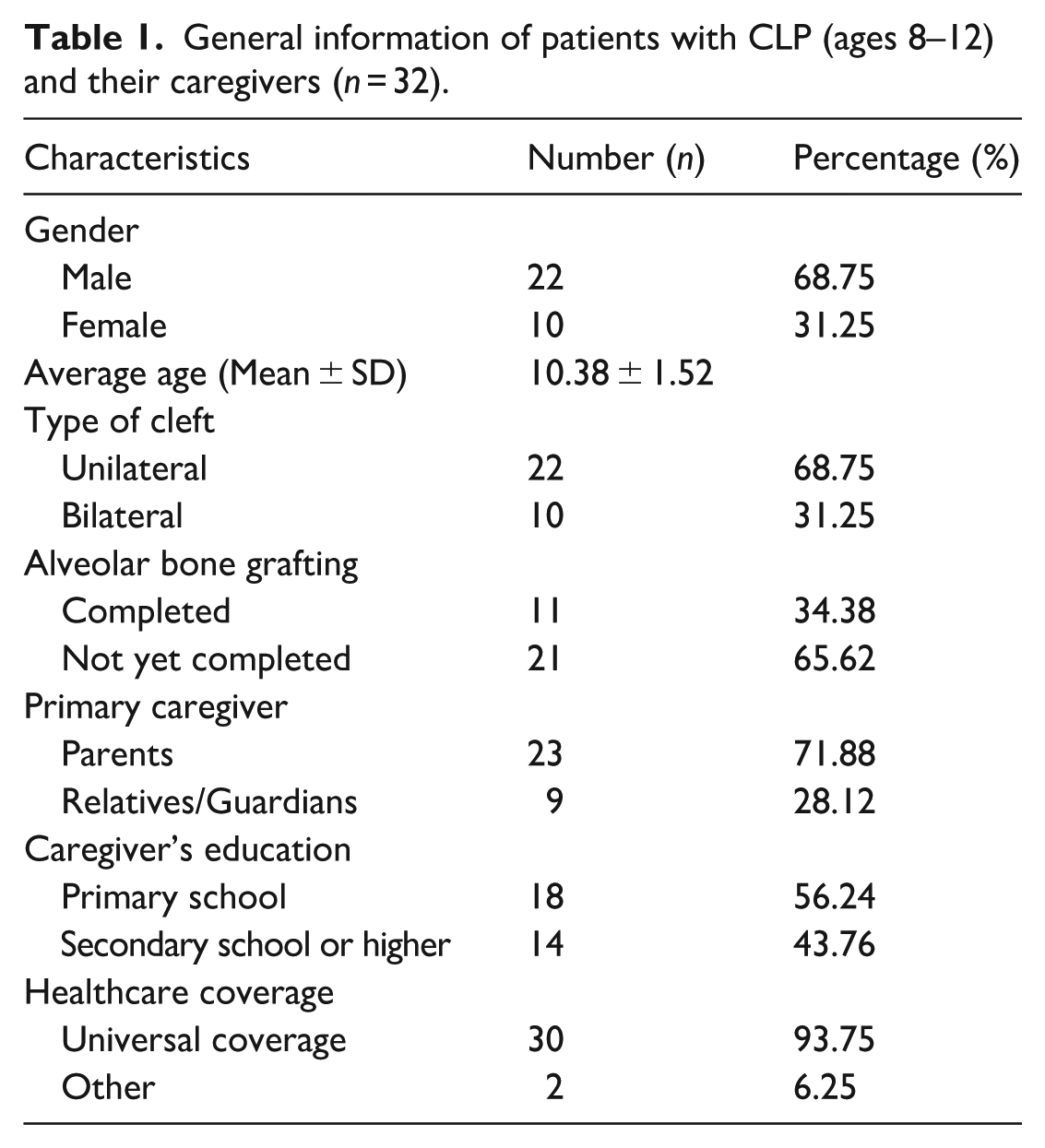
This table summarizes the demographic information of patients and their caregivers, including gender, age, cleft type, surgical history, caregiver details, and healthcare coverage (Table 2).
Psychosocial satisfaction of patients with CLP (n = 32).

Patients demonstrated high satisfaction in five key aspects (e.g., self-perception, voice, and hearing) with a mean score of 4.00 ± 1.26. However, moderate satisfaction was reported in nine areas related to facial appearance and speech clarity, with a mean score of 3.30 ± 1.20. The overall psychosocial satisfaction was 3.65 ± 1.23, indicating a generally positive outlook.
The satisfaction with the QoL in four aspects revealed that parents reported the highest satisfaction in service quality, with a mean score of 4.65 ± 0.52. This was followed by three aspects with a high level of satisfaction:
Medical care: 4.21 ± 0.91
Medical expenses: 3.66 ± 0.87
Psychosocial aspect: 3.54 ± 1.37
Meanwhile, the family impact was reported at a low level, with a mean score of 2.25 ± 1.71 (Table 3).
Satisfaction scores of parents regarding quality of life in five aspects and their interpretation (n = 32).

In comparing psychosocial satisfaction between patients and parents, a statistically significant difference was found in the aspect of effective communication (p-value = 0.024). No other aspects showed statistically significant differences (Table 4).
Comparison of psychosocial satisfaction between patients with CLP and their parents* (n = 32).

Discussion
This study demonstrated that, among the five domains assessed, parents reported the highest satisfaction with service quality, followed by high satisfaction with medical care, medical expenses, and psychosocial well-being. Prior studies suggest that parents with lower educational attainment report significantly higher satisfaction with services compared to those with higher education levels. This phenomenon may be explained by the difference in service expectations. Individuals with higher education often have a greater awareness of service standards and their rights, leading to higher expectations. In contrast, those with lower educational backgrounds may perceive public services as something to be grateful for, rather than scrutinizing them for quality, resulting in higher perceived satisfaction. 13
The family impact was rated at a low level, indicating that families experienced minimal disruption to daily life despite managing their child’s cleft condition. This positive finding can be attributed to the Tawanchai Center’s comprehensive care approach, which employs a multidisciplinary team with coordinated nursing support. Patients receive standardized treatment protocols that promote positive development in eating, speaking, and hearing abilities, consequently reducing family burden and contributing to high parental satisfaction levels. These findings align with Surakunprapa et al., who reported high life satisfaction among 10-year-old cleft patients, and Pakkasung et al., who demonstrated that home-visit care from the Tawanchai Center contributed to good-to-very-good health outcomes in adolescent patients. 14 The low family impact scores suggest that well-coordinated, specialized care can effectively minimize the psychosocial burden typically associated with complex pediatric conditions. 15
The psychosocial aspect of the study revealed that patients reported high satisfaction in five areas: self-satisfaction, speech clarity, communication ability, hearing, and lack of illness-related anxiety. The remaining nine items were rated as moderately satisfactory. Overall, patients expressed a high level of psychosocial satisfaction. Traditionally, Thai children in this age group tend to hesitate when expressing their opinions, resulting in parent-reported assessments. This study’s parental satisfaction ratings align with the research by Surakunprapa et al., which found that 10-year-old cleft patients reported high psychosocial satisfaction. Similarly, Pradubwong et al. noted high psychosocial satisfaction in patients aged 16–20 years. However, a previous study conducted with parents of cleft patients aged 8–12 at the Tawanchai Center found only moderate satisfaction in the psychosocial domain. 16 The higher satisfaction levels observed in the current study may reflect recent improvements in the Center’s multidisciplinary services, such as the implementation of a fast-track system to ensure timely treatment, the development of a speech therapy application, and the use of nasal stents to help maintain nasal structure after surgery. These service enhancements have likely contributed to better treatment outcomes, thereby increasing satisfaction reported by both patients and their parents.
The comparison of psychosocial satisfaction between patients and parents revealed a significant difference regarding communication clarity. Patients rated their communication ability as very high. Parents reported it as high but not at the same level. This discrepancy might stem from self-serving bias, where individuals tend to overestimate their own abilities compared to external observations. 17 To validate these findings, it’s recommended that a speech language pathologist (SLP) assess each patient’s communication skills objectively. This professional evaluation would provide a more accurate understanding of the patients’ speech clarity. Prior studies suggest that children who have received structured speech therapy such as articulation or resonance-focused intervention often show measurable improvements in communication skills. 18
A particularly significant contributor to these high satisfaction levels appears to be the role of the nurse coordinator. Serving as the central figure in patient management, the nurse coordinator facilitates communication among the multidisciplinary team, ensures timely referrals, provides psychological support to families, and offers education on treatment plans and home care, including wound management and device use. These efforts not only support physical recovery and reduce complications but also contribute to improved emotional well-being and family confidence. As case managers, nurse coordinators also ensure continuity of care aligned with treatment protocols, reinforcing the center’s interdisciplinary model. This comprehensive, nurse-led approach is likely a key factor in the consistently high satisfaction levels reported and underscores the critical role of coordinated care in improving QoL for both patients and their families.
This study does, however, have some limitations. First, the small sample size of only 32 participants from a single center, the Tawanchai Center, limits the generalizability of the findings to broader populations or different healthcare settings. Second, the majority of participants were families covered by the Universal Coverage Scheme or a special assistance program, which may have positively influenced their reported satisfaction levels and introduced potential bias. Third, the selected QoL assessment tool may not capture all relevant dimensions of QoL, potentially resulting in incomplete data. For instance, the educational dimension was not fully addressed, even though CLP conditions can significantly influence academic achievement and school experiences.
Despite these limitations, the study provides valuable insights into the quality of care at the Tawanchai Center. It is particularly significant as one of the first in Thailand to employ the THAICLEFT QoL Questionnaire to comprehensively assess both patient satisfaction in the psychosocial domain and parental satisfaction across all five domains. It is therefore recommended that QoL questionnaires for patients with CLP be further developed and adapted for different age groups. Such tools should be tailored to specific dimensions relevant to each developmental stage, thereby providing more precise and comprehensive insights into the overall QoL of affected individuals.
Conclusion
Parents demonstrated highest satisfaction with service quality, while reporting high satisfaction across treatment, cost, and psychosocial domains. Both patients and parents reported high psychosocial satisfaction overall. Patients rated communication effectiveness significantly higher than their parents, suggesting that communication approaches may resonate differently with children and adults. These findings indicate that while the Tawanchai Center delivers satisfactory care across multiple domains, attention to parent-patient communication strategies may further optimize satisfaction and overall QoL.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251378237 – Supplemental material for Satisfaction with the Quality of Life of Parents of Cleft Lip and Palate Patients Aged 8–12 Years, Tawanchai Center, Northeastern, Thailand
Supplemental material, sj-docx-1-smo-10.1177_20503121251378237 for Satisfaction with the Quality of Life of Parents of Cleft Lip and Palate Patients Aged 8–12 Years, Tawanchai Center, Northeastern, Thailand by Yupin Paggasang, Suteera Pradubwong, Sasitorn Duangmun, Kaweesak Saothonglang and Bowornsilp Chowchuen in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to express our gratitude to the patients and their guardians for their cooperation in participating in this study, to the staff members of the Tawanchai Center for collecting the data, and to the Research Center of Cleft Lip-Cleft palate and Craniofacial Deformities at Khon Kaen University for their financial support this study.
Ethical considerations
The study received approval from the Center for Ethics in Human Research, Khon Kaen University, Thailand (Ref. HE671291).
Consent to participate
Verbal and written informed consent was obtained from legally authorized representatives and all participants before the study.
Author contributions
All authors designed the study. Yupin Paggasang and Suteera Pradubwong collected the data. All authors participated in interpreting the data and discussing the findings. The manuscript was drafted by Yupin Paggasang. The manuscript was revised and approved by Kaweesak Southonglang.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) disclosed receipt of the following financial support for the research, authorship, and or publication of this article. This work was supported by the Research and Graduate Studies Khon Kaen University and Research Center of Cleft Lip-Cleft Palate and Craniofacial Deformities, Khon Kaen University, Khon Kaen Thailand (grant number TWG6611).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this research were acquired from a public resource.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.