
Abstract
Meningitis is a severe infection of the central nervous system. Cryptococcus neoformans is an uncommon fungal agent that can cause meningitis and often manifests unusual symptoms. While this infection is more prevalent in immunocompromised patients, it can also affect immunocompetent patients. A 33-year-old housewife living in the village visited our hospital emergency department complaining of a severe headache and mild fever for 7 days. We diagnosed an unusual occurrence of cryptococcal meningitis with infarction of the splenium of the corpus callosum in a patient who appeared to have a healthy immune system. This disease should be considered in immunocompetent individuals with persistent headache or other neurological findings, even in the absence of overt risk factors.
Introduction
Cryptococcus is an opportunistic, systemic fungal infection caused by ubiquitous encapsulated yeast found in many soil types in temperate regions worldwide. This yeast is especially found in soils enriched with decaying materials or bird or animal droppings. Transmission of this infection occurs primarily through inhalation.1,2 The most common causative organism is Cryptococcus neoformans var. grubii and Cryptococcus gatti, a native species in the Pacific Northwest is known to cause disease in patients with immune system deficiency. 3 This disease usually occurs as an opportunistic infection in immunocompromised patients, classically patients with human immunodeficiency virus (HIV).4,5 Its prevalence in immunocompromised patients is 5%–10%. 1 The highest burden of disease is related to people with HIV in low-income and middle-income countries. 6 Cryptococcal meningitis (CM) is uncommon in immunocompetent patients but may account for one-third of all cases. Cryptococcus causes 280,000 cases of infection in patients annually, of which 130,000 are fatal. A total of 152,000 cases and 112,000 deaths are estimated annually in patients with acquired immunodeficiency syndrome. 7 Cryptococcal meningoencephalitis also occurs in solid organ transplant recipients, patients with malignancy, and other immunosuppressive conditions, as well as in apparently immunocompetent hosts. 8 It is associated with various complications, including diffuse disease, as well as neurological complications such as increased intracranial blood pressure, cerebral infarction, vision loss, and other neurological defects. This disease is diagnosed by lumbar puncture (LP) and cerebrospinal fluid (CSF) examination, including fungal culture and cryptococcal antigen (CRAG) test. 5 Although there is little specific evidence on the epidemiology, presentation, treatment, and outcomes of cryptococcal infection in nonimmunocompromised patients, according to a retrospective study, this population may comprise up to 30% of patients who develop central nervous system (CNS) cryptococcus. 9 Antifungal therapy is the hallmark of this disease, and current guidelines recommend baseline intracranial pressure (ICP) measurement and management of increased ICP using LP. 10 There is a lack of complete information on the treatment of this disease in immunocompromised patients, as much of the data used to derive treatment guidelines comes from the treatment of HIV-positive individuals. Current Infectious Diseases Society of America (IDSA) guidelines Infectious Disease Society of America) recommends induction treatment with amphotericin B and flucytosine for 2–6 weeks, depending on the clearance of CSF cultures and the presence of neurological complications, followed by maintenance treatment with fluconazole for 6–12 months. Aggressive management of increased ICP with serial LP or ventriculoperitoneal shunt is also one of the important principles of treatment. 11 Early diagnosis of this disease and initiation of antifungal treatment are important to prevent complications such as increased ICP, cerebral infarction, and disseminated disease. Delay in diagnosis is associated with long-term neurological deficits. 5
Case report
A 33-year-old housewife living in the village came to our hospital emergency department, Rasoul Akram Hospital, Rasht Social Security Hospital, related to the Iranian Social Security Organization (ISSO), complaining of severe headache, and mild fever for 7 days. Her initial vital signs in the emergency department were as follows: pulse rate of 110 beats per minute, blood pressure of 120/90 mmHg, and temperature of 38°C. She was alert and well-oriented. Her pupils’ diameter was symmetrically 3 mm and responded to the light normally. Her cornea, oculocephalic, and gag reflexes were intact. Electrocardiography showed sinus tachycardia and a chest CT scan showed nodular opacity in the lower lung. We requested a brain magnetic resonance imaging (MRI) for her. Brain MRI showed an acute interface in the splenium of the corpus callosum (Figure 1). In this MRI, hyperintensity in the body of the corpus callosum was seen in the Diffusion Weighted Imaging sequence.

An acute interface in the splenium of the corpus callosum in the patient’s brain magnetic resonance imaging before treatment.
Blood tests indicated that the patient had normal immunological fungi and anti-HBS Ag, anti HCV, and HIV I/II antibodies were negative in serum. All vasculitis tests were normal. We performed a LP and sent it for CSF analysis. CSF analysis showed elevated opening pressure (25 cm/H2O), low CSF glucose level (39 mg/dl), and high CSF protein level (184 mg/dl). Upon finding these signs of possible CNS infection, CSF analysis showed Herpes Simplex Virus Polymerase Chain Reaction 1–2 was negative. Tubercle Bacillus Polymerase Chain Reaction was negative. Brucella, gram, and culture were negative. Indian Ink was negative (Table 1).
The results of the first LP.

CSF: cerebrospinal fluid; cu mm: cubic millimeter; LDH: Lactate Dehydrogenase; LP: lumbar puncture.
Although culture is the standard method for definitive diagnosis, detection of CRAG in the serum or CSF is used to make a presumptive diagnosis. CRAG screening in the peripheral blood is also recommended for HIV-infected individuals with CD4 cell counts >99%. 12 However, CRAG latex testing requires laboratory infrastructure and expertise, electricity, heat inactivation, cold chain delivery, and reagent cooling. Unfortunately, the required infrastructural structure is usually not available in resource-limited settings where cryptococcal prevalence is the highest. Thus, India ink microscopy is the preferred diagnostic method, despite its lower sensitivity. 13
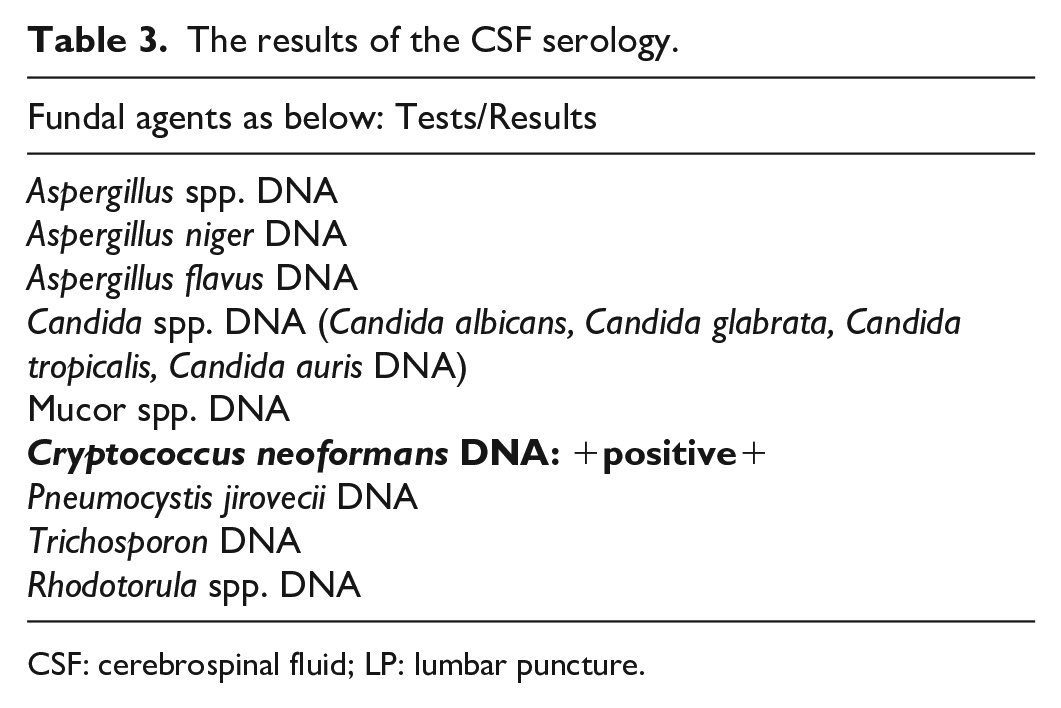
The patient was treated with intravenous Meropenem (2 g, three times a day) and Vancomycin (1 g, twice a day). Seven days after admission, her level of consciousness decreased, and she was immediately intubated and transferred to the intensive care unit. She was connected to mechanical ventilation in the synchronized intermittent mandatory ventilation mode. We performed a second LP on admission to the ICU. The LP results are listed in Table 2. The open pressure was elevated (25 cm/H2O), CSF glucose was low (41 g/dl), and CSF protein was high (180 mg/dl). The patient’s serum glucose level was 93 mg/dl. Subsequent CSF pathology revealed that the CSF serology was positive for C. neoformans (Table 3). After 2 weeks of hospitalization in the ICU, the patient was successfully extubated and transferred to the neurology ward of the hospital.
The results of the second LP.

CSF: cerebrospinal fluid.
The results of the CSF serology.
CSF: cerebrospinal fluid; LP: lumbar puncture.
The patient was treated with intravenous amphotericin B (5 mg/kg) once a day, and oral fluconazole capsules (20 mg twice a day) were successfully administered. She was hospitalized for 2 months at our hospital. She was visited daily by an infectious disease specialist and a neurology specialist. After 2 months, an MRI was performed again. In the second MRI, bilateral hyperintensity in the internal capsule was observed, which showed angiotropia of the fungal agent. Based on the normality of the second MRI (Figure 2) and the patient’s general condition, the patient was discharged. One month after discharge from the hospital, she was followed up at a neurological clinic. The patient’s condition was generally good during the follow-up visit.

Brain magnetic resonance imaging of the patient after treatment.
Discussion
Cryptococcal species can invade various tissues and organs of the human body and pose a serious threat to human health. Pulmonary cryptococcosis is the most common form, characterized by respiratory fungal infection caused by inhalation of cryptococcal spores. Cryptococcal infections can spread from the lungs to the CNS and other extrapulmonary sites. Cases of disseminated cryptococcosis are increasing owing to the continued evolution of Cryptococcus species and an increasingly susceptible population. 14
CM is a deadly fungal infection of the CNS caused by Cryptococcus, which affects the meninges and/or brain tissue. Common symptoms include fever, headaches, neck stiffness, and visual disturbances. Our patient’s chief complaint was also severe headaches. Patil et al. also reported an immunocompetent patient who experienced a subacute onset with a 30-day history of headaches and normal CT scan results. He presented with meningitis and C. gattii infection. 15 Prolonged headaches are the most common neurological signs of meningitis caused by Cryptococcus in immunocompetent patients.15,16 However, other signs may differ among patients.
Both immunocompromised individuals, such as those with HIV or organ transplants, and immunocompetent individuals are susceptible to CM. However, the incidence of Cryptococcus species-induced meningitis in immunocompetent patients appears to be rising.15,16 Untreated CM has a posthospitalization mortality rate of up to 100%. Despite treatment, complications like treatment resistance, poor prognosis, and high mortality rates remain significant. Thus, timely and effective treatment is essential for better CM patient outcomes. 17
C. neoformans and C. gattii species complexes are responsible for causing meningoencephalitis, resulting in high mortality rates and substantial morbidity, particularly in individuals with compromised T cell-mediated immunity, predominantly affecting those living with HIV. 18 In this instance, C. neoformans was the etiological agent of meningitis, not in a patient living with HIV, but in an immunocompetent individual.
As previously described, Cryptococcal infection is acquired through the inhalation of infectious particles present in the environment, a phenomenon particularly prevalent among individuals with compromised immune systems.19,20 However, this patient was immunocompetent and was not employed in environments where CM is commonly encountered. Approximately 20% of Cryptococcus cases occur in individuals who appear clinically immunocompetent. 9
With the advancement of antiretroviral therapy, the incidence of CM in HIV-negative individuals is increasing. As previously mentioned, the most common organisms responsible for cryptococcosis are C. neoformans var. grubii and C. gattii. C. gattii is a variant found in the Pacific Northwest and is known to cause disease in immunocompetent individuals. 3 According to the literature, identifying cryptococcus in immunocompetent patients can be challenging because the symptoms may be more gradual and subtle compared to the typical presentation of meningitis. This subtle presentation can delay diagnosis and treatment initiation, potentially resulting in complications and the progression to more severe disease. 5
In recent years, the diagnosis and management of CM have substantially changed. 21 In this case, the diagnosis was challenging. CM with an acute infarction of the splenium of the corpus callosum was discovered in an immunocompetent patient, while cerebral infarction and concomitant CM are scarce. Generally, Cryptococcal infections of the CNS are very rare in immunocompetent patients. They usually present as meningitis or as fungal cysts with or without hydrocephalus. Hamdan et al. reported a rare case of CM in an immunocompetent patient with obstructive hydrocephalus. 22 While in the presented case, hydrocephalus was not seen.
Considering the low glucose of CSF in the LP, fungal meningitis should be considered. However, considering the patient’s normal immunity, as well as the infarction of the corpus callosum, this diagnosis seems very unlikely. 9 On the other hand, all the patient’s vasculitis tests were normal, and the results of the tests on both occasions of CSF puncture were almost the same. In nonimmunocompromised patients, serum CRAG testing may be less reliable, especially when the disseminated disease is absent. Additionally, India ink staining is less frequently positive in HIV-negative individuals with cryptococcal meningoencephalitis. 9 In this case, India’s ink staining was negative, too.
The fundamental principles of CM management involve initiating aggressive antifungal medications such as amphotericin B and flucytosine upon diagnosis, followed by a prolonged antifungal treatment regimen aimed at achieving both clearance and suppression of the condition. Additionally, it is essential to proactively manage elevated ICP, which occurs in as many as 75% of patients.21,23 It is important to consult with an infectious disease specialist when making this treatment decision. 24
We consulted with our infectious disease specialist. She prescribed intravenous amphotericin B (5 mg/kg) once a day and oral fluconazole capsules 20 mg twice a day. The patient was visited daily by an infectious disease and neurology specialist.
According to the literature, patients with CM who do not exhibit typical meningitis symptoms and lack key risk factors, such as immunosuppression, may experience unfavorable outcomes due to delayed diagnosis and treatment. 25 In these patients, the primary prognostic factors include the type of underlying immunosuppression and any concurrent medical conditions. Additional factors linked to poor prognosis include a positive India ink test on CSF, a CSF white blood cell count below 20 μl, an initial CSF or serum CRAG titer exceeding 1:32, and elevated opening pressure during a LP procedure. 26 Although our patient was immunocompetent, we could diagnose her disease timely and start the treatment on time.
Conclusion
The exact determination of cryptococcal meningoencephalitis is vital to begin accurate treatment early and avoid long-term complications. Healthcare providers ought to consider this type of meningitis in patients with corpus callosum infarction, especially in patients with precise symptoms or risk factors such as recent travel to endemic regions or contact with contaminated pigeon droppings. Additionally, healthcare providers should be aware of the possibility of concurrent corpus callosum infarction in patients with CM, as this may complicate clinical presentation and disease management. Collaboration between neurologists, infectious disease specialists, and other healthcare providers is essential for the rapid diagnosis and management of this disease. Overall, this case emphasizes the importance of considering rare and atypical causes of meningitis in immunocompetent patients, especially when neurological symptoms are present. Early detection and treatment of CM can significantly improve patient outcomes and reduce the risk of long-term neurological sequelae.
According to the presented case, it is necessary to pay attention to the early diagnosis of this kind of meningitis, even in immunocompetent patients. Furthermore, in patients where corpus callosum infarction also occurs, this type of meningitis should be considered and the serology tests of CSF should be done as soon as possible. A delay in diagnosis has been linked to the development of long-term neurological deficits. Indeed, diagnosing cryptococcal meningoencephalitis in immunocompetent patients with a subtle and indolent presentation can be challenging. It’s important to consider this disease in immunocompetent individuals with persistent headaches or other neurological findings, even in the absence of overt risk factors.
Footnotes
Acknowledgements
Not applicable.
Author contributions
S.H.A. conceptualized the study, reviewed, edited the article, and submitted it. S.R. conceptualized, wrote, reviewed, and edited the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.