
Abstract
Uterine fibroids are benign tumors, arising from uterine smooth muscle cells. They are one of the most common benign tumors of the female genital tract among childbearing women, occurring in 20%–50% of women of reproductive age. The association of uterine myomas with pregnancy is high. This occurrence is constantly increased, linked to the onset of pregnancies, leading to the incidence of myomas gradually rising with age, hence the emergence of ultrasound reveals during routine ultrasound examinations of pregnancies, that were previously asymptomatic. Myomectomy during the second trimester was done and pregnancy continued safely to the third trimester. After successfully repairing it, the pregnant woman followed her antenatal care at Wollega University Referral Hospital, Western Oromia, Ethiopia. We presented the 20-year-old primigravida lady with a complaint of lower abdominal pain and a slight fever. We found a non-pedunculated, attached to the uterus via a broad base) myoma measuring 4 × 4 cm on 2D pelvic ultrasound. We admitted the client and gave her conservative management after we put her on antibiotics. Despite antibiotics, the pain persists we decided to manage it through an operation after we counseled the client about the potential complications. Then we removed the myoma without manipulating the uterus and it was a successful myomectomy without complicating the fetomaternal conditions. Currently, fetomaternal conditions are safe, and the woman is following her antenatal care at Wollega University’s Referral Hospital. In the majority of cases of women with fibroids, pregnancy comes with complications, according to literature data, The coexistence of the myoma with pregnancy: increased frequency of spontaneous abortions and premature births, increased risk of bearing ablation, higher incidence of maternal-fetal incommunicability, incorrect position of the fetus, more often performed cesarean surgery, higher probability of postpartum hemorrhage. Prenatal myomectomy can be safely performed in the first and second trimesters of pregnancy; however, it is recommended to deliver the baby via cesarean section, due to fear of intrauterine rupture of the uterus.
Introduction
Uterine fibroids are benign tumors, arising from uterine smooth muscle cells. They are one of the most common benign tumors of the female genital tract among childbearing women, occurring in 20%–50% of women of reproductive age. Due to the late reproduction of the tumors, their prevalence in over 35-year-old women treated for infertility ranges from 12% to 25% but too high for less than 35 years old.1,2
The association of uterine myomas with pregnancy is high. This occurrence is constantly increased, linked to the onset of pregnancies, leading to the incidence of myomas gradually rising with age, hence the emergence of ultrasound reveals during routine ultrasound examinations of pregnancies, that were previously asymptomatic. Even though there is mutual tolerance, fibroids can impact fertility, and complicate the course of pregnancy, delivery, and the postpartum period.3,4
The consequence of uterine fibroids with adverse perinatal outcomes is determined. The prospective studies, using ultrasound to monitor uterine fibroids during pregnancy, showed that about one-third of myomas increase in the first trimester of pregnancy. The main problem with the presence of myomas in early pregnancy is miscarriage. In addition, the incidence of spontaneous abortion is doubled taking pregnant women with uterine fibroids into consideration.5,6
It is not the number of myomas that affects the pregnancy but single myomas affect the pregnancy outcome. Myomas increase uterine contractile activity, and cause a compression effect on the developing fetal egg, bleeding, and uterine pain also follow. In addition, myomas are responsible for disturbances in the blood supply to the placenta and fetus, as well as for the increased risk of uterine bleeding in early pregnancy. Moreover, pregnant women with fibroids, in comparison to pregnant women without fibroids, are more likely to have premature uterine contraction (16.1%) and premature delivery and postpartum hemorrhage also occur among 10–30 clients (16.0%). 7
The prevalence of uterine myomas during pregnancy is underestimated due to the difficulty of differentiating fibroids and physiological myometrium thickening. Literature has shown that fibroids during pregnancy do not significantly change in volume but pain is the most common complication of fibroids during pregnancy and is more common in the second and third trimesters of pregnancy. 8
During pregnancy, red degeneration and torsion of the subserosa fibroid and acute lower abdominal pain create a diagnostic dilemma. Red degeneration of fibroid during pregnancy responds to conservative management, whereas torsion of a subserosa fibroid requires an emergency myomectomy. This case report describes a clinical scenario wherein difficulties were encountered in diagnosing the cause of acute abdomen during second-trimester pregnancy in a pregnant woman with fibroid uterus and the role of imaging to differentiate the above two clinical conditions.9–11
Myomas are rare in pregnancy, with a 2% prevalence, and their sizes do not increase during pregnancy. While they are usually asymptomatic, some patients may experience complications such as red degeneration, increased risk of spontaneous abortion, preterm labor, premature rupture of fetal membranes, antepartum hemorrhage, mal presentations, obstructed labor, cesarean section (CS), and postpartum hemorrhage. In such cases, cesarean myomectomy may be necessary to avoid interval myomectomy, repeat surgery, and improve uterine contractions in the postpartum period. Studies in Nigeria have reported that 10% of cases of myomas with pregnancy result in postpartum complications. 12
Co-occurrence of uterine myoma and pregnancy are more frequently observed now than in the past because many women are delaying childbearing. When they occur together, uterine myomas increase the incidence of spontaneous abortions, ectopic pregnancies, preterm labor, premature rupture of the membranes, placental abruptions, abnormal fetal presentations, and red degeneration. Myomectomy during pregnancy is rarely performed because of a fear of pregnancy loss and bleeding. We report a case of an aspiration of painful uterine myoma during pregnancy.13–15
Myomectomy during CS is an increased risk of intrapartum and short-term postpartum complications, especially bleeding. However, many authors agree that myomectomy is a safe procedure during.11,14,16–18
However, it is mandatory to stress the need for early surgical intervention to avert serious maternal and fetal complications and to urge obstetricians to maintain the unusual presentation of myoma with pregnancy with good fetomaternal outcomes. During the second trimester of pregnancy, a 20-year-old woman experienced severe lower abdominal pain. It was initially challenging to differentiate between fibroid myoma and physiological thickening of the uterus, but ultrasound scanning confirmed the diagnosis of fibroid myoma. A myomectomy was performed during the second trimester, and the pregnancy continued safely to the third trimester. The patient is currently receiving antenatal care at Wollega University Referral Hospital in Western Oromia, Ethiopia.
Case presentation
This is a 20-year primigravid patient from Nekemte town, West Oromia, known to have subserous (non-pedunculated, attached to the uterus via broad base) myoma measuring 4 × 4 cm on 2D pelvic ultrasound diagnosed during her pre-conceptional contact with the gynecologists (Figure 1). At 20 weeks of gestational age, she presented with severe lower abdominal pain and low-grade fever. No other complaint was noted. On physical examination, she is in severe pain. Blood pressure = 118/74, pulse rate = 104 bpm, respiratory rate = 21 bpm, T = 37.9°C. Laboratory investigation was done hemoglobin was about 10.9 mg/dl. On abdominal examination, the uterus was 24 weeks gravid. The uterine fundal surface was irregular due to a palpable tender mass attached to the fundal area of the uterus above the umbilicus. The fetal heartbeat was positive on auscultation. There was no uterine contraction.

Photograph showing while myomectomy procedure was done at Wollega University Referral Hospital, 2023.
On abdomen-obstetric ultrasound, there is single intrauterine pregnancy, positive fetal heartbeats, antero-fund ally implanted placenta (no sign of placental separation), adequate liquor, active fetal movement noted, aggregate gestational age 20 weeks + 0 days, there was 12 × 8 cm hypoechoic mass attached to the uterus with a large surface area of the mass in contact with the uterine subserous. There was positive probe tenderness on the mass. There was no adnexal mass seen. There was no pelvic collection. The abdominal scanning with ultrasound revealed no abnormality. Urine analysis was non-suggestive of infections.
She was put on IV Normal saline for rehydration, paracetamol 1 g po QID, and pethidine 25 mg IM QID. The client’s plan was normal delivery since she was not aware of having myoma. Despite the conservative management for 48 h, the patient continued to have severe pain and the degree of tenderness increased from the time of admission. The patient gave consent for myomectomy after being counseled for potential complications. After preparation for the operation, she was given indomethacin 25 mg per rectum and continued after the operation for 48 h in BID base. Intra-operatively, there was a large subserous myoma attached to the fundus via masculine connection and broad surface with the uterus (Figure 2). Ovaries, uterine tubes, urinary bladder, bowels, and appendix were all healthy looking. Myomectomy at its base was done without manipulating the uterus. Hemostasis secured (Figure 3). With the above clinical findings, the patient was admitted for inpatient management for the diagnosis of second-trimester beat per minute + acute abdomen secondary to red degenerative myoma (Figure 4). The abdomen is closed in layers. The patient and fetal conditions were followed post-operatively. Antipain and indomethacin were discontinued after 48 h of operation.
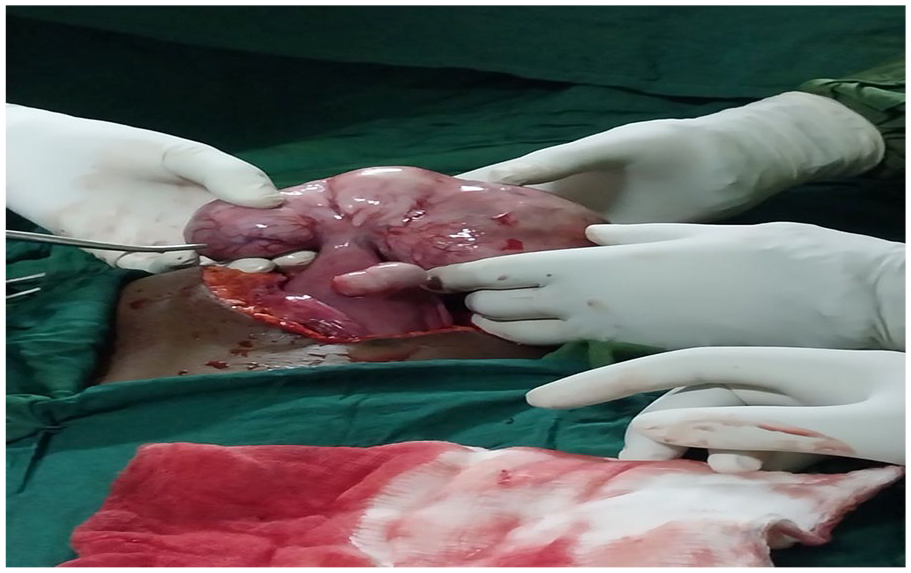
Photograph showing myomectomy procedure at Wollega University Referral Hospital, 2023.

Photograph showing degenerative myoma at Wollega University Referral Hospital.
Photograph showing histopathology for degenerative myoma at Wollega University Referral Hospital.
The patient was discharged on her fifth day of operation with an appointment. Up on discharge, there was no pain, no vaginal bleeding, normal vital signs, no abdominal tenderness, and with positive fetal heartbeats and normal obstetric scanning.
The patient is currently on her obstetric follow-up. She is 30 weeks + 6 days from her due date and has no complaints.
Discussion
Fibroids are tumors that grow from the muscle tissues in the uterus. It is not cancerous, but they are hormone-sensitive benign tumors of smooth uterine muscles, commonly encountered during pregnancy. They can be as small as a pea or larger than a grapefruit. The growth can be outside the uterine wall, inside the uterine cavity, or within the uterine wall. About 40%–60% of women have fibroids by the age of 35 whereas about 80% of the women have fibroids by the age of 50. However, diagnosing fibroids during pregnancy is very difficult. The reason behind this is that it looks like the thickening of the uterus muscle that occurs during pregnancy. This makes the known that fibroid cases are lower than the real cases happening. The primary problems that occur when fibroids are present are bleeding and pain, in 11% of the women, and miscarriage in about 14%. The prevalence in nonpregnant women ranges from 10% to 50%, but in pregnancy, it is reported to be 2%–10%. It is typically asymptomatic during pregnancy, but some women experience lower abdominal pain. Red degeneration, torsion, abortion, preterm labor, and antepartum hemorrhage complicate pregnancy and may present with acute pain in the abdomen during pregnancy. Fibroid-related complicatioarrive at term. Therefore, we need to report these unreportable cases ns occur in 10%–20% of women during pregnancy, and red degeneration occurs in 8%. The surgical management of fibroid during pregnancy includes torsion, failure of medical management, severe lower abdominal pain irrespective of the conservative management of a degenerated fibroid, and severe pressure symptoms. 17
The total incidence of uterine fibroids is estimated to be 20%–40% in women during their reproductive years. The association of myoma and pregnancy is becoming more frequent due to delaying the first pregnancy. 18
Although leiomyomas during pregnancy usually remain asymptomatic, they have complications such as abdominal pain, due to cernuous degeneration. The management of painful leiomyomas during pregnancy is medical, but myomectomies have been conducted in rare conditions reported. Even though myomectomies are avoided during pregnancy due to increased vascularity of the uterus leading to hemorrhagic complications. Successful myomectomies during pregnancy have been reported like our reportable cases. Our cases showed the most common indication for myomectomy during pregnancy due to severe abdominal pain to maintain pregnancy without any pregnancy complications. 13
Contrary to popular opinion, diagnosis of uterine fibroids during pregnancy is not an easy issue. In physical examination, it is possible to diagnose 42% of large (>5 cm) and 12.5% of smaller fibroids (3–5 cm). The usefulness of ultrasound examination in pregnancy is limited, mainly due to the difficulty in differentiating the physiological thickening of the uterine myometrium. During ultrasonography examination fibroids are only diagnosed in 1.4%–2.7% of cases. This leads to complications even where there are no ultrasonographic examinations. We need to remember that myomas can distort the architecture of the uterus and interfere with myometrial contraction, leading to uterine atony and postpartum bleeding. In addition, studies showed that retained placenta is more common in all women with myomas compared to the control group, regardless of the location of the fibroid. 7
Uterine fibroids are the most common benign uterine tumors, with an estimated incidence of 20%–40% in women during their reproductive years. The association of myoma and pregnancy is becoming more frequent due to the advanced maternal age. Uterine fibroids increase the number of CSs because they prevent the uterus not to contact.11,17
The coexistence of the uterine myoma with pregnancy might end up with pregnancy-related complications. Specially myomectomy during pregnancy aggravates pregnancy terminations and rarely arrives to continue pregnancy. But in our cases after myomectomy, pregnancy continues to arrive at term. Therefore, we need to report these unreportable cases to the scientific community.
Limitations
The lack of complete investigation of the potential cause for the coexistence of myoma with pregnancy was the limitation of the case report.
Conclusion
Uterine fibroid tumors arise from uterine smooth muscle cells. It is one of the most common tumors in 20%–50% of reproductive age. Due to the late reproduction of the tumors, their prevalence in over 35-year-old women treated for infertility ranges from 12% to 25% but too high for less than 35 years old.
The coexistence of myoma with pregnancy is a rare reportable case. Also, the existence of the myoma before 20 years old and arriving at term is a rare case. Successful myomectomy is also an infrequent procedure. Hence, we need to report the coexistence of myoma with pregnancy in 20-year-old primigravida women in Nekemte town. Successful myomectomy also makes it a reportable case.
Currently, both the fetus and mother are in good condition.
Footnotes
Acknowledgements
We thank the patient for allowing the publication of this case report.
Author contributions
All authors made a momentous involvement in the work reported, study design, execution, acquisition of data, analysis, and interpretation. They took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal requirements to which the article has been submitted and agreed to be accountable for all aspects.
Data availability
The datasets used are available from the corresponding author on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical approval to report this case was obtained from the Research Ethics Review Committee of the Institute of Health Sciences, Wollega University. The study protocol is performed per the relevant guidelines (22/IHS/2024).
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available to the corresponding authors.