
Abstract
Background:
Pregnancy complications are one of the most common health problems and causes of death among women in developing countries. Knowledge of obstetric danger signs during pregnancy, labor, and postnatal period is an essential first step for the appropriate and timely referral.
Objective:
To assess knowledge of pregnancy danger signs and its associated factors among pregnant women at Debre Tabor Town Health Facilities, South Gondar Zone, Northwest Ethiopia, 2019.
Methods and Materials:
Facility-based cross-sectional study conducted from 30 December 2018 to 30 January 2019 among 340 pregnant women. Simple random sampling was used to select study subjects. Data entered to Epidata 4.2 and exported Statistical package for social science version 26 for analysis. Binary logistic regression analysis was performed to determine predictors of knowledge of pregnancy danger signs among pregnant women. Finally, a p-value less than 0.05 was used to identify the significant variables.
Result:
Overall women’s knowledge score on pregnancy danger signs was 74.4%. This finding is not satisfactory and affects pregnancy outcomes. Age, religion, women’s educational status, family size, educational status, and antenatal care follow-up were identified as predictors of knowledge of pregnancy danger signs.
Conclusion:
Overall knowledge scores of pregnancy danger signs among women were satisfactory compared with different researches in Ethiopia and different countries. Age, mother’s occupation, and antenatal care visit were significant factors of knowledge of pregnancy danger signs among study participants.
Introduction
Pregnancy danger signs are warning signs that women encounter during pregnancy, childbirth, and postpartum. Globally, about 289,000 women die each year because of problems related to pregnancy and childbirth. Maternal mortality also remains a major challenge in developing countries. In sub-Saharan Africa, 1 out of every 16 women dies due to pregnancy-related causes. 1
The World Health Organization (WHO) estimated 300 million women in developing counties suffer from short-term or long-term illness due to pregnancy and childbirth that leads to high maternal mortality. More than half of these deaths occur in sub-Saharan Africa. According to the 2016 Ethiopia Demographic and Health Survey (EDHS), Ethiopian maternal mortality account 442. 2
About 75% of maternal deaths occur due to direct obstetric complications like hemorrhage, sepsis, pregnancy hypertensive disorders, obstructed and prolonged labor, and unsafe abortion. 3 Most mothers died in their homes due to poor awareness and definition of pregnancy danger signs. In Ethiopia, hemorrhage, hypertensive disorders of pregnancy, abortion, and sepsis are the leading causes of maternal deaths, which can be averted through recognition of danger signs of these complications and skilled institutional care, according to the Ethiopian. 4
Severe vaginal bleeding, prolonged labor, convulsions, retained placenta, premature rupture of membrane, fetal malposition are the commonest danger signs during labor and childbirth. Raising awareness among pregnant women about danger signs improves early detection of problems and reduces delays in deciding to seek obstetric care. 5
Every pregnant woman faces the risk of sudden, unpredictable complications that could end up with death or injury to themself or to their infant. Pregnancy-related complications cannot be reliably predicted. 6
The burden of obstetric danger signs is very critical, and pregnant women easily die from this preventable obstetric danger sign. Identifying pregnancy danger signs and its complications increase the capacity of women, their partners, and families to seek timely health care, following the appropriate steps to ensure safe birth and post-partum. 7
Antenatal care (ANC) has a potential role to identify and manage pregnancy complications, educate women’s risks during pregnancy and promote skilled birth attendance during childbirth. 8 Knowledge of the danger signs of obstetric complications is the essential first step in the appropriate and timely referral to essential obstetric care. 9
The majority of obstetric complications can be prevented if their occurrence is recognized and women receive timely quality obstetric care. 10 Appropriate knowledge of pregnancy danger signs is very critical to save the life of the mother and the fetus. Therefore, this study aimed to assess knowledge about pregnancy dangers signs and its associated factors among pregnant women at Debre Tabor Town Health Facilities, Northwest Ethiopia.
Methods and materials
Study area and period
The study was conducted at Debre Tabor Town Health Facilities. Debre Tabor Town is located 103 km far from Bahirdar (capital city of Amhara National Regional State). It is found 666 km away from Addis Ababa. The town has six Kebele and a total population of 60,563 of whom females account for 31,863 (52.6%). There is one hospital and three health centers in the town offering health care services for the population. The was study conducted from 30 December 2018 to 30 January 2019.
Study design
A facility-based cross-sectional study design was conducted.
Source population
All pregnant women who attended ANC at Debre Tabor Town Health Facilities during the data collection period were the source populations.
Study population
All sampled pregnant women attended ANC at Debre Tabor Town Health Facilities during the data collection period.
Eligibility criteria
Inclusion criteria
Those pregnant women who had ANC followed up at Debre Tabor Town Health Facilities were included in this study.
Exclusion criteria
Pregnant women who were seriously ill were excluded from the study.
Sample size determination and sampling technique
The sample size was calculated using the single population proportion formula, by considering the following assumptions. The proportion (p) of knowledge on pregnancy danger signs from the previous study, 11 95% level of confidence (Za/2)2 = 1.96, 5% of absolute precision, and 10% non-response rate. Hence, the final sample size was 340.

The reduction formula was used since the population was less than 10,000.

By adding a 10% none response rate, the final sample size could be 340. Source population (2041, average number of pregnant women attending ANC services in 1-month duration in the most recent quarterly report to study period in Debre Tabor Town Health Facilities).
Data collection tools and sampling procedure
Data were collected using a structured questionnaire which was prepared by reviewing previous studies.11,12 The questionnaire was first prepared in English then translated into the local language (Amharic). Pretest was conducted at 5% of participants in Mekane Eyesus Health Center and modification was considered according to its findings. The data were collected by face-to-face interviews by BSc holders, two nurses who are not working in the assigned area. The simple random sampling technique was used to select participants for the interview. The clients were interviewed in the waiting area prior to taking the ANC inappropriate and private room.
Operational definition
Knowledgeable
Those pregnant women who answer knowledge measuring items correctly above the mean value otherwise not knowledge.
Statistical analysis
The data were checked for completeness, entered into EPI Data version 4.2 to assure quality, and exported to SPSS version 26 for analysis. Descriptive statistics like frequencies, mean, SD, and percentage were calculated. The knowledge score of the participants was calculated by computing the response of the participants in knowledge measuring questions and using mean values as the cut-off points to classify the participants as knowledgeable and not knowledgeable. All variables were entered into a bivariate analysis and those explanatory variables with a p-value < 0.25 in the crude analysis were taken as a candidate for multivariable analysis.
Multivariable binary logistic regression analysis was carried out, and those variables with a p-value < 0.05 in the analysis and odds ratio with 95% confidence interval (CI) were taken as significant predictors of knowledge of pregnancy danger signs. Results are presented in tables, graphs, and figures.
Data quality assurance
Pre-tested data were done before the actual data collection to assure data quality. The training was given to data collectors for 1 day by the principal investigator focusing on the objective of the study, how to obtain consent, and keeping the confidentiality of the participants. The collected data were checked for completeness every day by the supervisors.
Ethical consideration
Ethical clearance was obtained from Debre Tabor University’s Ethical Review Committee. The University wrote an official letter was written to the Debre Tabor Town Health Office and consequently, The Town Health Office wrote a letter to each Health Facility. Before the interview, each participant was informed of the purpose of the study, possible benefits from the study, and confidentiality. Then, written informed consent was also taken individually, and any participant who was not assured had a full right to refuse to participate whether in the beginning or in the middle of the interview without any negative connotation on their future service. They were also informed that they will be kept anonymous.
Results
Socio-demographic characteristics of the respondents
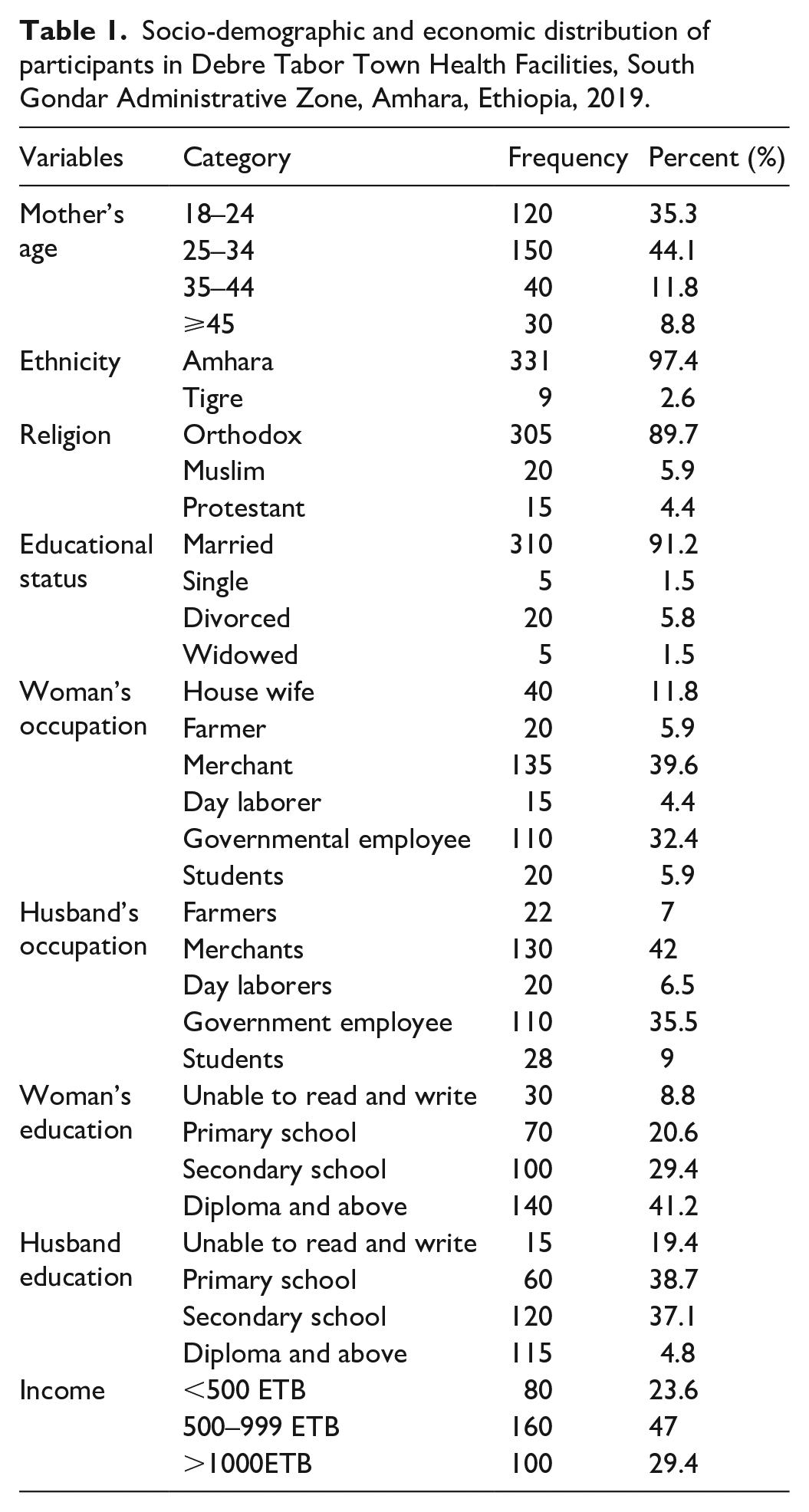
Three hundred and forty women were included in this study (response rate of 100%). Regarding sociodemographic, the majority of participants were in the age group of (25–34 years) 44.1% (150), married 91.2% (310), and merchants 39.6% (135) (Table 1).
Socio-demographic and economic distribution of participants in Debre Tabor Town Health Facilities, South Gondar Administrative Zone, Amhara, Ethiopia, 2019.
Obstetric histories of the respondents
Regarding obstetric history, the majority of respondents had first ANC follow-up 37.6 % (128), stillbirth 85.3% (290), and antenatal visits 88.8% (302) (Table 2).
Obstetric histories of the pregnant women in Debre Tabor Health Facilities, Ethiopia, 2019.

Knowledge of pregnant mothers about pregnancy danger signs
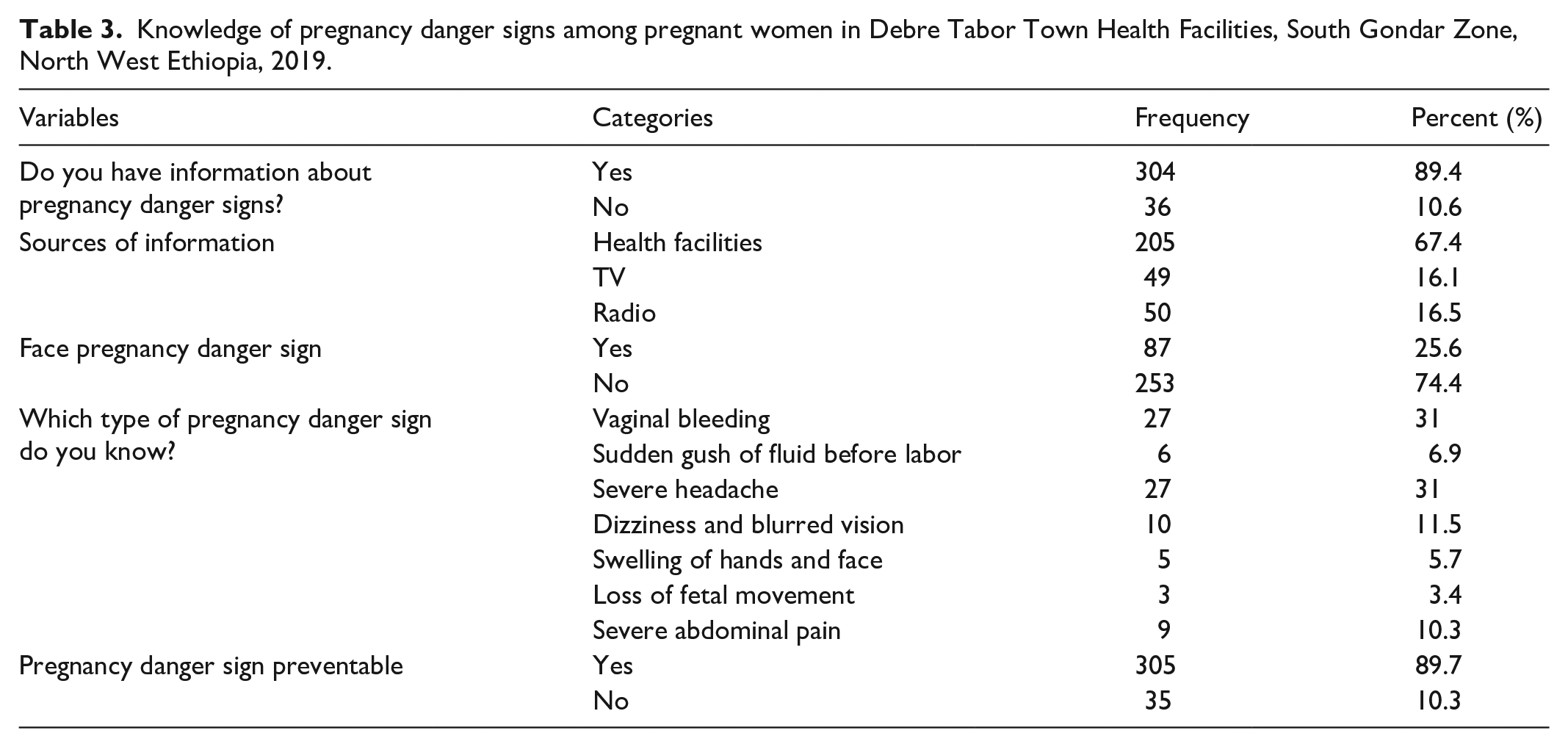
The overall knowledge score of pregnancy danger signs was 74% (252) (Figure 1). A majority, 89.4% (304) of respondents had information about pregnant danger signs and 67.4% (205) of the pregnant mothers got information about danger signs from the hospital (Table 3).

Knowledge of pregnant women about pregnancy danger signs in Debre Tabor Town Health Facilities, South Gondar Zone, North West Ethiopia, 2019.
Knowledge of pregnancy danger signs among pregnant women in Debre Tabor Town Health Facilities, South Gondar Zone, North West Ethiopia, 2019.
Factors associated with knowledge of pregnancy danger signs
Multivariable logistic regression analysis was performed to identify significant factors of knowledge of pregnancy danger signs using SPSS version 26. Women’s age group (35–44) years, Religion, women’s occupational status, women’s educational status, source of information about danger signs, and women with ANC follow-up were significant predictors of knowledge of pregnancy danger signs. Women’s age group (35–44 years) were 2.6 times more likely knowledgeable about danger signs than mothers age group < 18–24 (adjusted odds ratio (AOR): *2.6 (1.87–9.7)). Similarly, protestant followers had a 3.1 times more likely knowledge of pregnancy danger sign than orthodox Christianity followers (AOR: *3.1 (1.00–6.2)). Regarding occupation, governmental employee mothers knew five times more likely pregnancy danger sign as compared to housewives, and this was the highest knowledge level of mothers associated with danger signs of pregnancy (AOR: *5. 00 (1.04–8.1)) (Table 4).
Factors associated with knowledge of pregnancy danger sign among pregnant women in Debre Tabor Town Health Facilities, South Gondar Zone, North West Ethiopia, 2019.

Discussion
The overall knowledge score of the pregnant women about danger signs of pregnancy was 74.4% (CI 69.4%−79%). This finding is higher as compared with studies in Kinondoni municipality, Tanzania 31% 9 and in South Nigeria (24.9%), 13 Mechekel (55.1%), 14 Debre Birhan, Ethiopia (38.6%), 11 and Northern Ethiopia (37.5%). 12 The main reason of inconsistency might be the difference in the level of awareness and access the service among study participants. In addition, this finding was higher as compared to a study conducted at Harrar Regional state, Ethiopia 44.67%. 15 This difference might be due to the difference in study settings.
Our study finding is also higher as compared with study at Sidama Zone (24.1%) 16 and Eastern Ethiopia (30.4%). 17 The discrepancy may be due to the difference might be due to the level of knowledge and access to health information among women.
This study finding is also lower than the study in Madagascar (80.9%). 9 The main reason for this difference might be geographical difference and availability of service for participants. In addition, this study finding is in line with study at Mizan Aman, Ethiopia (77.5%). 9
In this study, age was a significant factor for pregnancy danger signs among study participants. The resulting finding showed that those mothers in age greater than 35 years were 2.6 times more likely to be knowledgeable about pregnancy danger signs than mothers greater than 35 years (AOR: 2.6 (1.87–9.7)). This finding is in-line with the study conducted at Shashemene, Ethiopia, 11 and Yirgachefe, Ethiopia. 18 It may be as the women’s age increases, they can be familiar with different danger signs and get information from their colleagues. Similarly, the region was a significant factor for pregnancy danger signs among participants. Those protestant followers were 3.1 times more likely to be knowledgeable than orthodox Christianity followers (AOR: 3.1 (1.00–6.2)).
Regarding occupation, governmental employee mothers were five times more likely to be knowledgeable than housewives (AOR: 5.00 (1.04–8.1)). This study was in line with Yirgachefe. 18 The governmental employee might easily access informed of pregnancy danger signs. In addition, the participants who had ANC visits were 3.1 times (3.1 (1.00–7.3)) more likely to be knowledgeable than those who had no ANC visits. The main reason, might as a woman accessing the ANC, they will get adequate information regarding pregnancy danger signs by healthcare providers.
Limitations of the study
Since it is a cross-sectional study, it is difficult to claim causal relationships. The study used cross-sectional study design which only gives evidence of women’s knowledge status within the times of the study period. It does not tell women’s knowledge of obstetric pregnancy danger signs before and after of the study period.
Conclusion
Overall knowledge scores of pregnancy danger sign among women were satisfactory compared with different researches in Ethiopia and different countries. Age, mother’s educational status, mother’s occupation, and ANC visit were significant predictors of pregnancy danger signs among study participants. The majority (83.9%) of the mothers had information about pregnant danger. Even though, the majority of pregnant mothers know about danger sign of pregnancy, it is not enough because all pregnant women are at risk for pregnancy danger signs. Therefore, the proper ANC delivery and community mobilization about awareness creation about pregnancy danger signs are very crucial. The healthcare provider should better emphasize counseling concerning pregnancy danger signs during ANC service promotion and community mobilization. The participants were also recommended to attend regular ANC visits and attain adequate information regarding pregnancy danger signs and their preventions.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221074492 – Supplemental material for Knowledge of pregnancy danger signs and its associated factors among pregnant women in Debre Tabor Town Health Facilities, South Gondar Administrative Zone, North West Ethiopia, 2019: Cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221074492 for Knowledge of pregnancy danger signs and its associated factors among pregnant women in Debre Tabor Town Health Facilities, South Gondar Administrative Zone, North West Ethiopia, 2019: Cross-sectional study by Worku Necho Asferie and Bizunesh Goshu in SAGE Open Medicine
Footnotes
Acknowledgements
All authors thank Debre Tabor University and departments of nursing for their contribution, data collectors, and study participants deserved to.
Authors’ contributions
W.N. and B.G. contributed to the study conception and design, W.N. supervised the study and conducted data analysis; B.G. was involved in data collection and contributed on data analysis, W.N. critically revised the manuscript. Finally, all authors read and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Debre Tabor University Ethical and Research Review Committee (approval no. dt/201/2019). Confidentiality of data kept at all levels of the study, and the data not used for other purposes other than for this study.
Informed consent
Written informed consent was obtained from all study subjects before the actual study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.