
Abstract
Foreign body (FB) ingestion leading to appendicular perforation, although rare in adults, presents a complex clinical challenge. The clinical presentation may not always be straightforward, necessitating a comprehensive array of diagnostic examinations. In fact, accurate and timely diagnosis is crucial to prevent severe complications. In this report, we present a case where a misleading clinical presentation led to the unexpected discovery of appendicular perforation during surgery, despite initial suspicion of small bowel perforation – a 77-year-old male patient who was edentulous and under follow-up for chronic bronchitis stage IV. He sought medical attention due to a 2-week history of right iliac fossa pain, during which he did not experience vomiting or fever. Upon physical examination, there was a tenderness noted in the sub umbilical region. An abdominal computed tomography (CT) scan was performed, revealing the presence of a dense FB which seems to be a bone located in the last ileal loop. Additionally, the appendix appeared slightly distended. Given the clinical presentation, which strongly indicated acute peritonitis resulting from small bowel perforation, and following consultation with gastroenterologists, it was decided that endoscopic retrieval was not suitable for this case. Therefore, a surgical approach was chosen, involving a midline incision, as laparoscopy was absolutely contraindicated because of patient’s respiratory distress. Per-operatively, we identified a clear effusion, and within the wall of the appendix, we discovered a thin, sharp chicken bone that had become lodged, resulting in a phlegmonous and perforated appendix. The 2-cm bone was successfully removed, and an appendectomy was performed. The post-operative period was uneventful, and the patient was discharged on the fourth postoperative day. This case highlights the need for a high index of suspicion for atypical clinical presentations and the ongoing need for research to improve our understanding and management of this rare condition, ultimately enhancing patient outcomes.
Introduction
The ingestion of indigestible objects is a common occurrence in children but is a rare condition in adults. It often happens accidentally, although it can also be associated with patients suffering from mental disorders or individuals in correctional facilities.1,2 Ingested foreign bodies (FBs), regardless of their composition, have the potential to become lodged at various locations within the digestive tract. Although certain locations, such as the small bowel, are more frequently affected, the appendix represents an atypical site for FB retention. 3 In this specific scenario, the presence of a FB can precipitate an acute appendicitis. Notably, documented cases of acute appendicitis resulting from FB ingestion exist in the literature, albeit being a rare occurrence, particularly in adults. The mechanism underlying this phenomenon is intricate, as these objects have the potential to trigger appendicitis within days, years, or even decades after ingestion. Delayed complications, including appendicitis or perforation, may manifest due to the FB becoming coated with fecal matter, leading to chronic inflammation, subsequent obstruction, and, eventually, perforation.3–5 The clinical presentation may not always be straightforward, necessitating a comprehensive array of diagnostic examinations, including abdominal X-rays or computed tomography (CT) scans, and occasionally, intraoperative exploration. In this report, we present a case where a misleading clinical presentation led to the unexpected discovery of appendicular perforation during surgery, despite initial suspicion of small bowel perforation.
Case presentation
We present a 77-year-old male patient who is edentulous and is under follow-up for chronic bronchitis stage IV, which has progressed to the stage of respiratory failure. He sought medical attention due to a 2-week history of right iliac fossa pain, during which he did not experience vomiting or fever. The patient did not report any changes in bowel habits. Upon physical examination, the patient was found to be afebrile, Glasgow coma scale 6 of 15/15, the heart rate was 90 bpm, and there was a tenderness noted in the sub umbilical region. The remainder of the abdominal examination revealed softness and the absence of pain. Laboratory investigations revealed leukocytosis with a white blood cell count of 16,000 cells per milliliter and an elevated C-reactive protein level of 87 mg/L. An abdominal CT scan was performed, revealing the presence of a bone-dense FB located in the last ileal loop, embedded in the wall approximately 7 cm from the ileocecal valve (Figure 1). Additionally, the appendix appeared slightly distended with surrounding fat densification, and there was a moderate effusion present. Notably, upon further questioning, the patient denied any history suggestive of FB ingestion. This was significant as the patient was edentulous and could not recall ingesting any inappropriate substances. Given the clinical presentation, which strongly indicated acute peritonitis resulting from small bowel perforation, and following consultation with gastroenterologists, it was decided that endoscopic retrieval was not suitable for this case. Therefore, a surgical approach was chosen, involving a midline incision, as laparoscopy was absolutely contraindicated because of patient’s respiratory distress. During the surgical procedure, while monitoring the patient and collaborating with the anesthesia team, we optimized treatment of chronic bronchitis with bronchodilators, steroids, and oxygen therapy. Per-operatively, we identified a clear effusion, and within the wall of the appendix, we discovered a thin, sharp chicken bone that had become lodged, resulting in a phlegmonous and perforated appendix (Figure 2). The 2-cm bone was successfully removed (Figure 3), and an appendectomy was performed. We thoroughly examined the small bowel loops and the colon, both of which were found to be intact. The postoperative period was uneventful, and the patient was discharged on the fourth postoperative day. After a 1-year survey, the patient was seen in the outpatient department. At no time did he represent abdominal pain, and he was aware while eating solid food. Pathological analysis of the resected appendix revealed inflammatory lesions (Figure 4).

Abdominal computed tomography showing a 2 cm-bone-dense foreign body located in the last ileal loop, embedded in the wall.

(a) Per-operative findings showing a phlegmonous and perforated appendix. (b) A thin and a sharp chicken bone extracted through the perforation.

Image of the chicken bone postoperation.
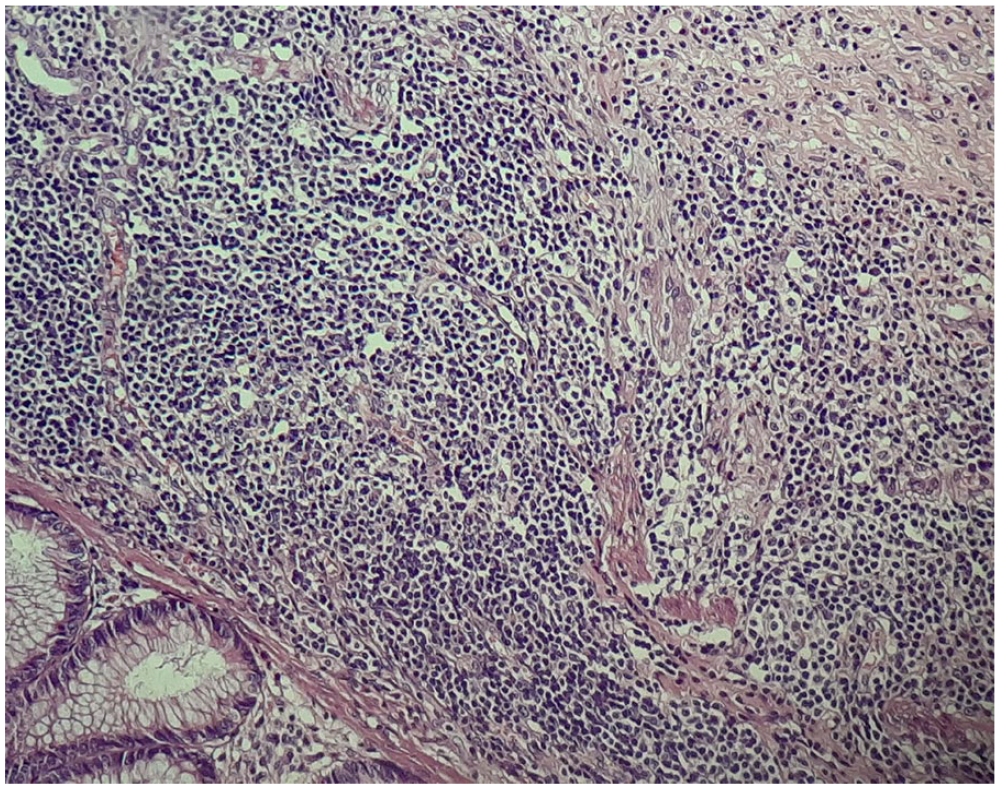
Pathological slides of the phlegmonous appendix showing inflammatory infiltration involving all layers of the appendicular wall.
Discussion
FB ingestion is an infrequent clinical issue in healthy adults, in stark contrast to its prevalence among children. In the majority of adult cases, FB ingestion is food-related, 4 and the majority of instances resolve spontaneously without complications, 4 rendering surgical intervention unnecessary. 5 In exceptionally rare cases, estimated to occur at a rate of 0.0005%, these FBs become lodged in the appendix. 5 This is a rare condition, often asymptomatic, and there is a distinct time interval between ingestion of the FB and the onset of appendicitis. 7 However, FB-induced appendicitis manifests with a wide spectrum of clinical presentations, ranging from complete asymptomatic cases to abdominal pain and other nonspecific symptoms. 7 The variation in presentation depends on several factors, including the size and shape of the FB, the anatomic position of the appendix, 8 and the orifice of the appendicular lumen. For instance, blunt FBs can lead to appendix irritation through obstruction, while elongated and pointed objects, like the one in our case, are more likely to cause perforation and the development of an abscess. 6 This diverse array of symptoms can result in a range of clinical presentations, encompassing generalized peritonitis, localized abscess formation, the presence of inflammatory masses, localized peritonitis, obstruction, and even occasional hemorrhage. 9 Radiopaque objects can be identified through X-ray imaging, but the diagnosis of FB-induced appendicitis requires confirmation via a CT scan.4,5 Interestingly, approximately 11% of cases involving FBs found in the appendix were discovered incidentally in patients undergoing surgery for classic acute appendicitis presentation. 5 In our specific case, however, the clinical presentation never suggested appendicular perforation, from the initial evaluation to the CT scan. This was the reason for choosing a midline incision rather than the McBurney incision, 10 especially when laparoscopy was absolutely contraindicated. The existing literature suggests that the initial diagnostic step should be an X-ray, as it is cost-effective and carries a lower radiation risk for the patient. However, in cases involving suspected sharp objects, such as fish bones, chicken bones, or hair bezoars, a direct CT scan is advisable to precisely locate the FBs and identify potential complications, like perforation and obstruction. 5 While most ingested FBs traverse the gastrointestinal tract without issue, this is not always the case for sharp or pointed objects, which have a higher risk of causing appendix perforation. 5 Some studies recommend prophylactic appendectomy for sharp objects lodged in the appendix, 11 while others suggest attempting gastroscopy or colonoscopy before resorting to laparoscopic-guided removal. 8 Nonsurgical approaches, ranging from bowel preparation, enteroscopy, colonoscopy, conservative management with intravenous antibiotics, and serial X-ray follow-up, are often reported as unsuccessful. 5 Surgery remains the primary treatment modality, aimed at preventing severe and potentially fatal complications. 5 Our report holds significance as it highlights the diversity of clinical presentations associated with appendicular perforation, an extremely rare condition, which prompted us to perform, falsely, and when a laparoscopic approach is not possible, a laparotomy surgery when it could have been performed by the McBurney incision. This emphasizes the importance of collecting all relevant clinical, biological, and radiological information essential for the diagnosis of appendicular perforation, and subsequently, for determining the most appropriate surgical approach.
Conclusion
FB ingestion leading to appendicular perforation presents a complex clinical scenario. Accurate and timely diagnosis is critical to prevent severe complications. Our case highlights the importance of a multidisciplinary approach, utilizing clinical, biological, and radiological data for optimal surgical decision-making. Prompt CT scans are essential, especially in cases involving sharp objects lodged in the appendix. Surgical intervention remains the primary treatment option, offering the best chance to avert life-threatening outcomes.
Footnotes
Acknowledgements
None.
Author contributions
T.M.M.: conceptualization, writing—original draft; K.N.: supervision, N.S.: writing—original draft; B.S.: validation, writing—review and editing; C.M.A.: validation, writing—review and editing; O.A.: validation, writing—review and editing; K.M.: validation, writing—review and editing; N.R.: validation, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written informed consent was obtained from the patient to publish this case report and accompanying images. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.