
Abstract
Due to the rarity of the condition, Valentino’s syndrome is an underrated differential diagnosis for acute appendicitis. We describe a patient with Valentino’s syndrome in whom preoperative and intraoperative diagnoses were challenging due to misleading clinical, investigative, and morphological findings. A 31-year-old woman who was on methylprednisolone for sensory radiculopathy presented to the emergency department with acute right lower quadrant pain. The clinical diagnosis of acute appendicitis was supported by the elevated inflammatory markers and ultrasonographic findings. An appendicectomy and an ovarian cystectomy were performed due to the findings of mild appendicitis and right ovarian endometrioma, respectively. Postoperatively, she developed peritonitis with a purulent bile-stained discharge from the surgical site and per vagina. Contrast-enhanced computed tomography of the abdomen showed a retroperitoneal collection at the second lumbar vertebral level extending along the right paracolic gutter to the pelvis and intraperitoneal fluid collections in right lower quadrant and pelvis. An emergency exploratory laparotomy confirmed a perforation at the posterior aspect of the duodenum which was repaired with an omental patch. Unfortunately, relaparotomy and end ileostomy were required due to colonic perforation with the eroded drain tube. She made an uneventful recovery with intensive care and underwent ileostomy reversal after 12 weeks. We emphasize the clues to have a high degree of suspicion during preoperative and intraoperative evaluation to recognize this lethal mimicker of acute appendicitis.
Introduction
Acute appendicitis is a common pathology that presents to the emergency service as right lower quadrant pain. Careful clinical evaluation and diagnostic workup are important as there are a number of common differential diagnoses such as ureteric colic, Crohn’s disease, ruptured ectopic pregnancy, tubo-ovarian abscess, ovarian torsion, and mesenteric adenitis.1,2
Valentino’s syndrome is rare and less known, but a potentially lethal condition that occurs following gastric or duodenal perforation mimicking acute appendicitis clinically, biochemically, and radiologically. We present a case of Valentino’s syndrome in which preoperative diagnosis was challenging due to misleading clinical and investigation findings.
Case
A 31-year-old woman presented to the emergency department with 1-day history of right lower quadrant abdominal pain. She described a constant, moderate, aching type of pain associated with nausea, vomiting, and anorexia. Her symptoms were worsening over 4 h prior to the admission. She denied a history of fever, urinary symptoms, alteration of bowel habits, or vaginal discharge. Her surgical and medical histories were unremarkable except for right-sided L5S1 sensory radiculopathy for which she had been taking a course of methylprednisolone for over a week duration.
She was afebrile, neither pale nor icteric. Abdominal examination revealed tenderness in the right iliac fossa without rebound tenderness. Psoas sign was positive while Rovsing’s sign and renal angle tenderness were absent. She was normotensive without tachycardia. The straight leg raise test on the right side was positive.
Laboratory investigations revealed a neutrophilic leukocytosis with an elevated level of C-reactive protein (CRP = 78 mg/L). Her urine HCG test was negative, and the urinalysis was unremarkable. Ultrasonography showed inflammation in the right iliac fossa with an inflamed appendix and few reactive mesenteric lymph nodes. There was no free fluid or mass formation. A right-sided simple adnexal cyst measuring 4 cm × 4.5 cm was noted additionally. X-ray of the lumbosacral spine showed a straight spine without bony abnormalities. The clinical diagnosis of acute appendicitis was made and was supported by Alvarado score of 7.
The patient was started on intravenous cefuroxime and metronidazole. Written informed consent was obtained for open appendicectomy because of the non-availability of a laparoscopic facility. During the surgery, mildly inflamed and congested appendix was apparent. There was brownish-yellow discoloration with thrombosed blackish small vessels visible through the posterior parietal peritoneum (Figure 1). There was no free fluid. Appendicectomy was performed and was sent for histopathological analysis. The ultrasonically mentioned right adnexal cyst appeared to be a chocolate cyst that was accidentally ruptured during manipulation. The peritoneal cavity was thoroughly washed, and the drain was placed into the pelvis following the opinion of the Gynecology team.

(a) Mildly inflamed appendix and (b) brownish-yellow discoloration of the retroperitoneum with thrombosed small blood vessels.
The patient did not show clinical improvement expected following appendicectomy despite the continuation of intravenous antibiotics postoperatively. On postoperative day 4, she developed generalized abdominal pain, fever, and a purulent bile-stained discharge from the surgical site as well as per vagina. A few clips were removed from the incision site, a pus sample was sent for culture, and antibiotics were changed to meropenem and metronidazole. A contrast-enhanced computed tomography (CECT) of the abdomen was performed with oral contrast immediately and showed multiple intraperitoneal fluid collections in right lower quadrant and pelvis. A retroperitoneal collection at the second lumbar vertebral level lateral to the right psoas muscle and posterior to the second part of the duodenum extended along the right paracolic gutter into the right iliac fossa (Figure 2). There was no pneumoperitoneum and evidence of contrast leak from the gut to the peritoneum.
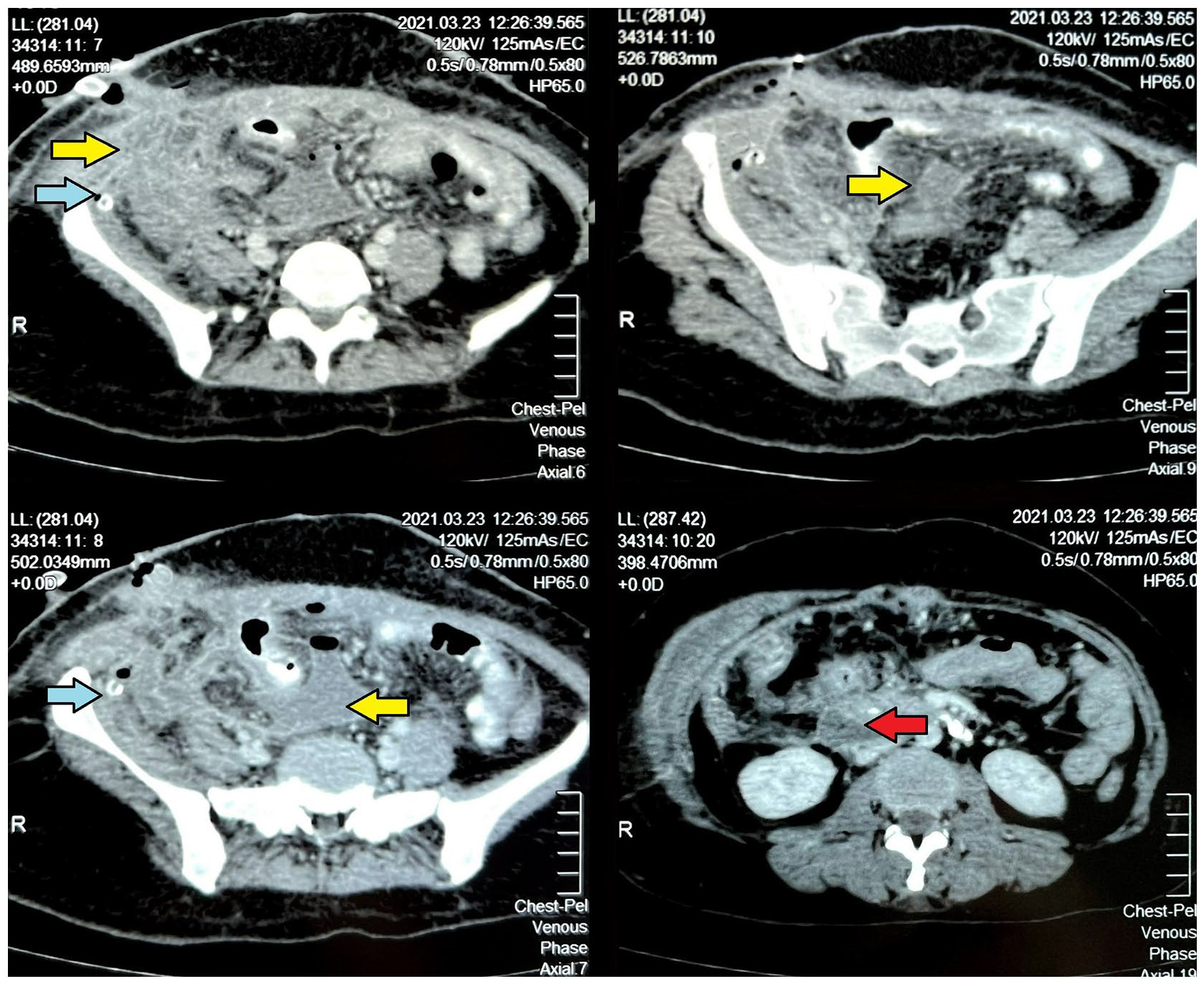
CECT showing multiple intraperitoneal fluid collections in between the bowel loops, in right lower quadrant and pelvis (yellow arrow). A retroperitoneal collection at the second lumbar vertebral level (red arrow) extended along the right paracolic gutter into the right iliac fossa. The surgical drain tube is present within the fluid collection.
An emergency laparotomy through a midline incision was performed on the fifth postoperative day. Generalized purulent peritonitis with inter loop and pelvic collections were noted. A pus sample was sent for culture. The right colon was mobilized and assessed for perforations, but no abnormalities were noted. Duodenal Kocherization demonstrated bilious fluid seepage from the retroperitoneum and perforation at the posterior aspect of the junction of first and second part of the duodenum. An omental patch was applied to cover the perforation. The stomach, rest of the large bowel, jejunum, and ileum were unremarkable. A thorough peritoneal washout was done, and paraduodenal and pelvic drains were inserted. Postoperatively, the patient was kept nil orally with nasogastric drainage, and total parenteral nutrition and intravenous proton pump inhibitor (PPI) were continued. The patient was managed postoperatively in the High Dependency Unit. After which she showed remarkable improvement clinically and biochemically. Bilious drainage gradually declined and stopped by postoperative day 5.
Unfortunately, on postoperative day 7, she developed sudden abdominal distension shortness of breath and desaturation which required endotracheal intubation and intensive care. A feculent discharge was noted through appendicectomy wound dressing and the drain. Traumatic ascending colonic perforation due to drain was identified during the re-exploratory laparotomy. A limited right hemicolectomy was carried out with the creation of end ileostomy in the left iliac fossa. Subsequently, the patient made an uneventful recovery and was discharged on postoperative day 10 on PPI after completing Helicobacter pylori eradication treatment. Endoscopic assessment performed on postoperative eighth week revealed healed posterior wall duodenal ulcer while colonoscopy was unremarkable. The ileo-colonic anastomosis was done after 12 weeks, and the recovery was uneventful.
Discussion
Valentino’s syndrome was named after a French movie star Rudolph Gugleimi Valentino who underwent appendicectomy following hospitalization with right lower quadrant pain in 1926. He later died due to peritonitis and multi-organ failure. The autopsy revealed a perforated gastric ulcer.3–5
Gastric or duodenal peptic ulcers occur due to infection with H. pylori, use of nonsteroidal anti-inflammatory drugs and steroids, smoking, alcohol, and Zollinger-Ellison syndrome. Perforation is one of the detrimental complications of peptic ulcers with increased mortality.6–8
The eponym Valentino’s syndrome is referred to when the digestive fluid from peptic ulcer perforation seeps and settles down in the right iliac fossa causing inflammation and giving rise to symptoms and signs similar to acute appendicitis. The majority (60%) of peptic ulcers are anterior and perforation occurs into the peritoneal cavity.7,8 Free peritoneal air may be apparent as the gas under the diaphragm in the erect chest X-ray. As the digestive fluid tracks along the paracolic gutter into the right iliac fossa, a fluid collection is apparent surrounding the normal appendix in ultrasonography or intraoperatively. 9
Unfortunately, our patient had a posterior wall ulcer perforation which allowed the digestive fluid to seep into the retroperitoneum along with the psoas muscle into the right iliac fossa. Therefore, intraperitoneal changes such as free air and free fluid were absent. Retroperitoneal free air around the kidney (veiled kidney sign) may be apparent in X-ray in 33% of patients with posterior duodenal perforation.10,11 Even though the classic X-ray signs are largely obsolete, detection of such a finding would have led to preoperative CT imaging.
The diagnosis of acute appendicitis was based on the combination of Alvarado score, CRP level, and ultrasonographic findings. Alvarado score is a 10-point system that stratifies patients suspected to have acute appendicitis based on symptoms, signs, and laboratory findings. The cut-off point of 5 is used to rule out acute appendicitis with a sensitivity of 99% and a specificity of 81%. 12 Considering the inconsistent results obtained from the studies that have been performed to evaluate the diagnostic performance, Alvarado score alone is inadequate as a diagnostic tool. A combination of Alvarado score, elevated CRP level, and positive ultrasonographic findings has shown a higher diagnostic accuracy limiting the use of CECT of the abdomen (sensitivity of 94% and specificity of 95%) for equivocal cases.13–15 As the initial diagnosis of acute appendicitis was based on the above three criteria, CECT of the abdomen was not performed prior to surgery in this case.
Mild thickening of the appendix in Valentino’s syndrome can be explained by chemical peri appendicitis due to the digestive fluid from peptic ulcer perforation.3–5 The presence of a right ovarian endometrioma which may have contributed to her symptomatology in the right lower quadrant further misled us not to think of other differential diagnoses. On retrospective thinking, the tissues with blackened small blood vessels in the background of brownish-yellow discoloration in the right iliac fossa were due to the bile containing digestive fluid that tracked along the retroperitoneum causing thrombophlebitis (Figure 1). We recognize this as a characteristic finding to suspect Valentino’s syndrome due to retroperitoneal duodenal perforation not reported in the literature previously.
Generalized purulent peritonitis was due to the combined action of persistent leakage of acid- and enzyme-rich duodenal contents and bacterial translocation from the intestinal flora. The presence of a second pathology again delayed the clinical suspicion and decision of the CECT abdomen as the initial deviation from normal recovery was attributed to the peritoneal contamination following the accidental rupture of ovarian endometrioma. Unfortunately, the later development of fecal peritonitis caused by a perforation in the ascending colon is probably due to erosion of the drainage tube into the colon facilitated by acid- and enzyme-rich intestinal fluid due to duodenal perforation.
Conclusion
Valentino’s syndrome is a lethal but rare mimicker of acute appendicitis. Even though the preoperative diagnosis would be difficult, certain clues allow us to have a high degree of suspicion in a patient with clinical features of acute appendicitis. These include a history of peptic ulcer disease or having risk factors for peptic ulcer disease, and ultrasonic findings of a non or mildly inflamed appendix with surrounding fluid despite raised inflammatory markers. If these clues are present, performing a CECT abdomen would be beneficial before embarking on an appendicectomy. Usage of laparoscopy for intraoperative assessment might have changed the course of management.
The brownish-yellow discoloration of retroperitoneal tissues in the right iliac fossa with blackened streaks of small blood vessels is an intraoperative clue that is suggestive of a perforated posterior duodenal ulcer. Therefore, we must have a higher degree of suspicion of this lethal mimicker of acute appendicitis.
Footnotes
Author contributions
V.E.U.R. and M.S.E.K. conceived the idea of reporting this case. V.E.U.R., D.S.H.J., S.S., D.W., and M.S.E.K. were involved in the management of the patient data collection and interpretation. V.E.U.R. and G.P.U.P.d.S. wrote the manuscript. S.P.B.T. and M.S.E.K. modified the manuscript, and all authors read and approved the final version of the manuscript.
Availability of data and materials
All data used to support the findings of this study are included within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.