
Abstract
Esophageal perforation resulting from foreign body ingestion is a known complication that can lead to various complications, including esophageal erosion, esophageal perforation, and mediastinitis, with rare involvement of adjacent anatomical structures. Uncommonly, it can also result in the formation of a mycotic aortic pseudoaneurysm. In this report, we describe a 9-month-old girl who presented with an esophageal perforation following ingestion of a pin. She developed life-threatening mediastinitis with a mycotic aortic pseudoaneurysm in the aortic arch that required urgent surgical repair, which involved evacuation of infected mediastinal hematoma, resection of the mycotic aortic pseudoaneurysm, and reconstruction of the aortic arch. The patient did well after surgery and was discharged home in satisfactory condition. The case highlights the importance of early diagnosis, prompt intervention, and antibiotic therapy in esophageal perforation with suspected mediastinitis. Awareness of this life-threatening complication is crucial for optimizing patient outcomes.
Introduction
Esophageal perforation is a well-known complication of sharp or corrosive object ingestion, and it can lead to many complications, such as local erosion, perforation, mediastinal inflammation, and vascular injury. One of the life-threatening complications is bacterial mediastinitis, which carries a high percentage of morbidity and mortality.1–3 Infrequently, mediastinitis can extend to the great vessels, causing mycotic aortic pseudoaneurysms. 4 In this case report, we describe an infant with a 14-day history of esophageal perforation following a foreign body ingestion (FBI; pin) leading to mediastinitis and mycotic aortic pseudoaneurysm. The main aim of this report is to highlight the importance of early recognition, utilize proper investigation for diagnosis, and provide a management plan for such a serious complication.
Case presentation
A 9-month-old girl, previously healthy, had accidental ingestion of a pin that passed later on with stool. Initially, she was asymptomatic. Upon initial medical evaluation, the patient was doing well with negative chest and abdomen x-rays and was discharged. Two days after ingestion, she developed a fever with hemoptysis and melena. After a few days and due to her persistent fever, echocardiography (ECHO) was requested and showed a pseudo-aortic aneurysm. The patient was then referred to our center for further investigation and management.
At our center, chest computerized tomography with contrast showed mediastinitis and aortic pseudoaneurysm compressing the carina and left main bronchus. No foreign body was seen. ECHO confirmed the presence of a pseudoaneurysm in the aortic arch. An upper gastrointestinal (GI) endoscopy demonstrated an esophageal abrasion seen in the upper third of the esophagus with multiple gastric ulcers. There was no clear perforation in the esophagus. The infant was initially treated conservatively with broad-spectrum antibiotics and kept nil per os with administration of maintenance intravenous fluid.
The patient was discussed in a multidisciplinary meeting at our cardiac center, and the decision was taken to take her for emergent high-risk surgery.
Intraoperatively, cardiopulmonary bypass with systemic cooling was instituted. The findings during surgery were a mediastinal abscess and hematoma with two large pseudoaneurysms communicating with the lumen of the aorta (Figure 1(a) and (b)). All aneurysmal and infected aortic tissues were resected with the evacuation of infected mediastinal hematoma and reconstruction of the aortic arch using a pulmonary homograft through median sternotomy. Myocardial protection was maintained by antegrade cardioplegia. Then, a left thoracotomy was done to achieve optimal repair of the distal part of the aortic arch. A thoracotomy incision was performed, and the chest was entered through the fourth intercostal space. Adequate dissection was performed to delineate the anatomy. Large amounts of mediastinal and peripleural hematoma and abscess were evacuated. The distal aortic coarctation was repaired. The thoracotomy wound was then closed. (Figure 2 demonstrates a timeline of infection and the investigations done to confirm the diagnosis).
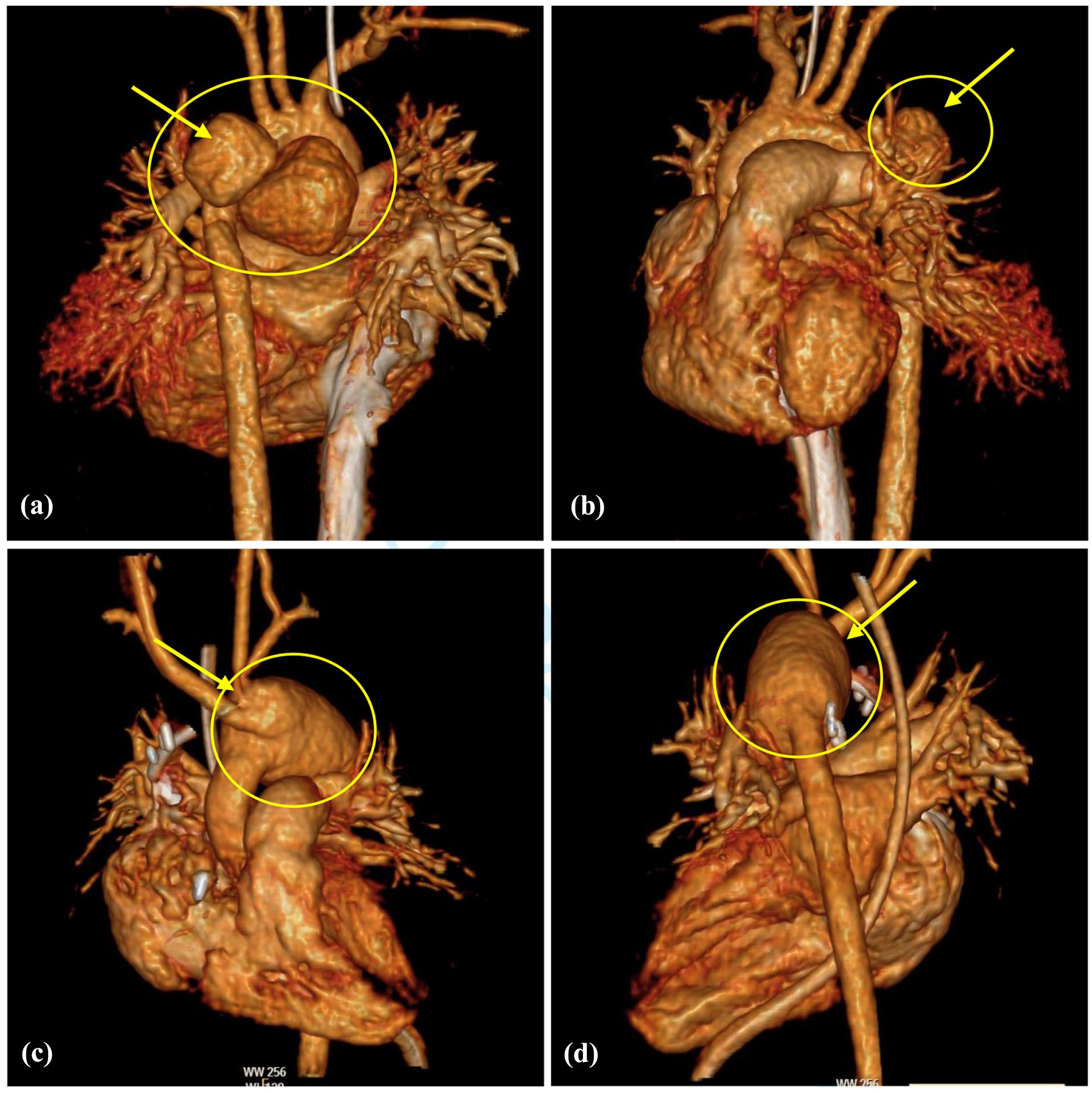
A posteroanterior view (a) and a lateral view (b) of a reconstructive cardiac CT scan image for a 9-month-old girl showing two large pseudoaneurysms communicating with the lumen of the aorta (yellow arrow).

Timeline of mycotic aortic pseudoaneurysm progression following pin ingestion in a child, including initial symptoms, progression of mycotic aneurysm (A), and mediastinitis (B). 3-D reconstruction (C) and ECHO (D) demonstrating the pseudoaneurysm communication with the aorta (yellow dashed line). Cardiac surgery was performed after 10 days to resect the aneurysm, reconstruct the aorta, and drain the mediastinum. 3D reconstruction of the aorta (E) after resection of aneurysm and repair of aortic arch using a pulmonary homograft. Echo after 1 year (F) demonstrating satisfactory arch repair and laminar flow with no gradient.
Two esophageal ulcers were found and clipped during a postoperative endoscopy that was performed to secure a nasogastric tube (NGT) safely.
Mediastinal cultures grew Staphylococcus aureus, confirming the bacterial mediastinitis diagnosis with a mycotic aortic pseudoaneurysm. To treat her infection, a 6-week antibiotic course was given.
A 4-week after-surgery follow-up chest CT scan showed the resolution of mycotic pseudoaneurysm and mediastinitis with satisfactory aortic arch reconstruction (Figure 1(c) and (d)). The infant was discharged home after completing her antimicrobial course satisfactorily. A 1-year follow-up showed normal growth and development of an asymptomatic child with no gradient at the area of the aortic arch. The timeline in Figure 2 demonstrates the recovery of mediastinitis and outcome after 1 year of arch aortic repair.
Discussion
FBI is a well-known subject in pediatrics. Most cases do not require urgent medical intervention. However, the FBI can be life-threatening, as in our case. The vast majority of these cases happen accidentally while the child is playing with the foreign body inside his mouth, and most of them do not need intervention because the foreign body will pass out of the body through the digestive system without complication. 5 In up to 4% of cases, the foreign body is removed or vomited before arriving at the ER; in 20% of cases, the foreign body cannot be found or identified. 5 About 23% of them required intervention to be removed. 5 Up to 40% of the patients with safety pin ingestion and other sharp objects do not need intervention, and the foreign body passes the GI system spontaneously. 5 Nevertheless, the remaining cases that required an endoscope or surgical removal had, in general, no significant complications except if there was perforation or deep mucosal erosion. 6 One of the most serious consequences associated with a particular form of ingestion is button battery ingestion. Some studies have found that it can cause tracheoesophageal fistulas in up to 4% of cases. 7
A few cases of sharp object ingestion had esophageal perforation that affected the mediastinum and soft tissue in that area, leading to serious complications like tracheoesophageal fistula, pneumomediastinum, vascular trauma, paraesophageal abscess, pneumothorax, pericarditis, and others.3,8
Due to the presence of a vascular structure adjacent to the esophagus, it is at risk of direct injury from a sharp object penetrating it. Similarly, the inflammatory process of mediastinitis can lead to vascular bleeding, pseudoaneurysm, or communication between the esophagus and the main blood vessel, leading to aorto-esophageal fistula. 9
There are limited published reports about sharp FBI causing mediastinitis with mycotic aortic pseudoaneurysm in children. Almost all of these cases related to fish bone ingestion were documented in adult literature. 10 These cases were managed by antibiotics and different surgical interventions such as endovascular stent graft, resection of the pseudoaneurysm, or only mediastinal debridement. 10
Upper GI endoscopy has its role in detecting esophageal ulcers and perforations, especially in cases of foreign ingestion that lead to mucosal injury, such as lithium batteries, sharp objects, or caustic chemical ingestion. Though direct visualization had a high detection percentage, it still can miss some cases and can’t rule out esophageal perforation. Due to the risk of esophageal perforation, it is recommended to secure NGT insertion under direct visualization with endoscopy and avoid blind insertion. NGT is needed for nutritional supplements when esophageal injury is suspected or confirmed, since oral feeding is contraindicated until the esophageal mucosa heals with normal esophageal function. Concerning our case, the initial endoscopy did not show clear esophageal mucosal injury. However, the follow-up endoscopy, which was done for NGT insertion, demonstrated two esophageal ulcers that were clipped.
In cases with confirmed or suspected esophageal perforation, a chest CT scan is useful and recommended. A study reported up to 100% sensitivity and 90% specificity.11,12 It can demonstrate an air leak in the mediastinum or evidence of inflammation. Despite the presence of different radiological modalities, CT scans continue to be the best choice, not only for primary diagnosis but also to know the extent of the complication and for follow-up.11,12
Broad-spectrum intravenous antibiotics are needed in the presence of suspected or confirmed mediastinitis. In cases of bacterial mediastinitis, one study reported that up to 66% of cases were gram-positive organisms (mainly methicillin-resistant Staphylococcus aureus (MRSA) and coagulase-negative Staphylococcus), and up to 28% of cases were gram-negative bacteria (mainly Escherichia coli, Klebsiella pneumoniae, and Enterobacter cloacae). 13 It is important to mention that some cases had polymicrobial and multi-resistant bacteria. 13 It is recommended to send cultures from the blood, mediastinal fluid, and the site of surgery with the administration of broad-spectrum antibiotics.
Controlling the infection source with debridement of the soft tissue is a mainstay in the surgical management of complicated mediastinitis. In case of vascular involvement in mediastinitis, resection of infected tissue and reconstructive vascular surgery are needed. Surgical intervention should be done as early as possible to avoid the dissemination of deep-seated infection and other complications like recurrent infection or even rupture of the aneurysm with imminent death.14,15 Some cases required revision surgery due to the recurrence of infection. 16 The use of a pulmonary homograft in our patient permits satisfactory repair, controlling the infection and allowing growth of the aorta with laminar blood flow after 1 year of follow-up.
While the majority of FBI in children is incidental, a few can be a marker of child abuse or inflecting injury, requiring awareness, psychological assessment of caregivers, and social support. 16
Conclusion
Ingestion of a sharp foreign body can lead to esophageal perforation with serious complications like severe mediastinitis affecting great vessels, with a high risk of high morbidity and mortality. In these situations, early diagnosis and intervention are the key to control and improve the outcome.
Footnotes
Acknowledgements
Nothing.
Ethical Considerations
Ethical approval for this study was obtained from King Abdullah International Medical Research Center (KAIMRC) (IRB Approval No.: 0000071524).
Consent to Participate
Written consent was taken from the caregiver.
Consent for Publication
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Author Contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data is available in the patient’s medical record as well as in the primary author's research file.