
Abstract
This study examines the contraindications of gabapentin and Nucleo C.M.P Forte in metformin-controlled diabetic patients, focusing on their potential to induce hyperglycemia. A case report of a 65-year-old woman with type II diabetes is presented, demonstrating elevated blood glucose levels following the initiation of gabapentin and Nucleo C.M.P Forte. The literature review highlights limited data on gabapentin-induced hyperglycemia, with additional consideration of the potential effects of Nucleo C.M.P Forte. The study suggests modifying insulin therapy in diabetic patients taking gabapentin and calls for further research on this interaction.
Key message
Gabapentin can cause mild disturbances in blood glucose levels, but the precise mechanism remains unknown due to limited data in medical literature. In the absence of other factors, clinicians may consider gabapentin and Nucleo C.M.P Forte as potential contributors to glucose fluctuations in metformin-controlled diabetic patients. Consequently, modifying insulin therapy may be warranted based on these principles.
Introduction
The objective of this study is to investigate the impact of gabapentin and Nucleo C.M.P use in metformin-controlled diabetic patients, focusing on the influence of these medications on glucose fluctuations. Diabetic patients often experience neuropathic pain, which can significantly affect their quality of life. Gabapentin and Nucleo C.M.P Forte are commonly prescribed medications for pain management in these patients. However, there are limited data on the effects of these medications on glycemic control, particularly in patients already on metformin therapy.
Diabetic patients often experience neuropathic pain, which can significantly affect their quality of life. Gabapentin and Nucleo C.M.P Forte are commonly prescribed medications for pain management in these patients. However, understanding the pharmacological properties and mechanisms of action of these medications, especially concerning diabetes, is crucial for optimizing treatment outcomes. 1
Gabapentin, a structural analogue of gamma-aminobutyric acid (GABA), exerts its analgesic effects through binding to the α2δ subunit of voltage-gated calcium channels in the central nervous system. In rodents that are given gabapentin ⩾400 mg/kg (orally or intragastrical), sedative effects have occurred. The dosage ranges from 600 to 1800 mg per day, divided every 8 h into three doses. 2 While gabapentin’s primary indication is for the treatment of seizures and neuropathic pain, its potential impact on glycemic control in diabetic patients remains poorly understood.
Similarly, Nucleo C.M.P Forte, a combination medication containing cytidine, inositol, and nicotinamide, is widely used for pain management in diabetic neuropathy. Nucleo C.M.P Forte has a wide spectrum of efficacy. It is used to treat carpal tunnel syndrome, and in addition to its analgesia, it is also used in treating neuropathy induced in diabetic patients, it is also used in the treatment of spinal cord injuries.3–5 However, its specific mechanisms of action and potential interactions with other diabetic medications, such as metformin, require further investigation.
Gabapentin and Nucleo C.M.P Forte are the usual treatments in clinics for pain caused by disk prolapse at any level of the spinal cord. 5
For the treatment of diabetes, metformin is used. This medication is used to decrease both the production of hepatic glucose and to decrease the absorption of gastrointestinal glucose, as well as to increase the sensitivity of target cell insulin.6,7 Some diabetic patients are controlled by metformin (dose differs depending on the case), especially in the earlier stages of diabetes. 7
Gabapentin may lead to mild disruptions in blood glucose levels, with the underlying mechanism of action still unknown. Because of the lack of data in medical literature, it is difficult to define the true incidence or causality of gabapentin-induced hyperglycemia. 8
Despite the clinical relevance of gabapentin and Nucleo C.M.P Forte in diabetic patients, there is a notable lack of data on their interactions and effects on glycemic control in medical literature. This knowledge gap underscores the need for a comprehensive review of existing research and relevant studies to elucidate the potential contraindications and implications for diabetes management.
Case report
A 65-year-old woman presented with severe lower back pain radiating to her thighs and legs. She had a known history of type II diabetes mellitus, managed with daily metformin (500 mg). Further medical history revealed stable angina and hypertension, both controlled with propranolol (80 mg). There were no prior surgical interventions or relevant medical history.
On examination, the patient was diagnosed with chronic arthritis and disk prolapse at L1–L2, confirmed by X-rays and laboratory tests. To manage her pain, gabapentin (100 mg) and Nucleo C.M.P Forte (5 mg) were prescribed once daily. The patient was instructed to continue her regular metformin and propranolol therapy.
The patient’s HbA1c value was 7.2%. She reported a sedentary lifestyle and a predominantly home-made diet consisting mainly of carbohydrates with low vegetable intake.
After 2 days, the patient reported elevated blood glucose levels, measuring 147 mg/dL. Treatment with gabapentin and Nucleo C.M.P Forte was paused, and the patient’s blood glucose levels were monitored daily. After 4 days, medication was resumed and blood glucose monitoring continued for 5 days, excluding 1 day for efficacy assessment, detailed in Table 1.
Fasting blood glucose levels measured before and after initiating treatment with gabapentin and Nucleo C.M.P Forte.
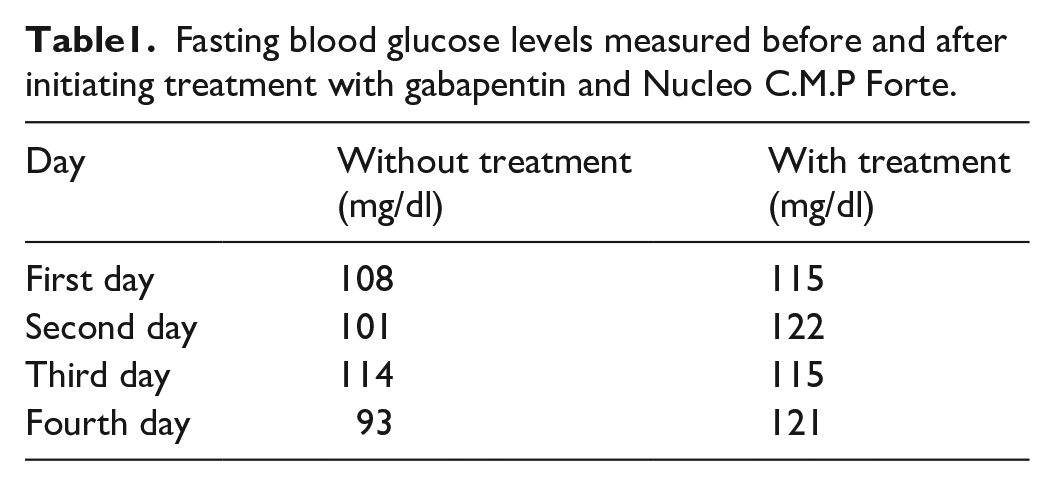
The mean glucose level without treatment was 104 mg/dL, while with treatment it was 118.25 mg/dL. These results were obtained using version 25 of the Social Science Statistical Package (SPSS) program (IBM Corp., Armonk, NY).
Discussion
The observed increase in blood glucose levels following the initiation of gabapentin and Nucleo C.M.P Forte underscores the potential association between these medications and hyperglycemia in diabetic patients. Several factors may contribute to this phenomenon, including the pharmacological properties of the medications, interactions with other drugs, and individual patient characteristics. 9
Gabapentin, a structural analogue of GABA, has been implicated in alterations in glucose metabolism, although the exact mechanisms remain elusive. Proposed mechanisms include direct effects on pancreatic function, modulation of neurotransmitter systems involved in glucose regulation, and alterations in insulin sensitivity. However, definitive conclusions regarding gabapentin’s impact on glycemic control necessitate rigorous mechanistic studies and clinical trials. 10
Similarly, Nucleo C.M.P Forte, containing cytidine, inositol, and nicotinamide, may also influence glucose levels through its pharmacological actions. While data on its glycemic effects are limited, its frequent use in pain management for diabetic neuropathy warrants consideration of its potential implications for blood glucose regulation. 11
The interactions between these medications and other concomitant drugs, such as metformin and propranolol, can further complicate glycemic management in diabetic patients. Clinicians should exercise caution and conduct comprehensive medication reviews to minimize the risk of adverse glycemic outcomes. 12
Recent research has shed light on gabapentin-induced hyperglycemia in diabetic patients. A systematic review and meta-analysis found that gabapentin use may be associated with a modest increase in blood glucose levels, although the precise mechanisms remain unclear. In addition, a randomized controlled trial demonstrated that gabapentin treatment was associated with a significant increase in fasting blood glucose levels compared to placebo, highlighting its potential impact on glycemic control. 13
In addition to gabapentin, recent studies have also focused on the glycemic effects of Nucleo C.M.P Forte in diabetic patients. A retrospective cohort study suggested that Nucleo C.M.P Forte may exacerbate hyperglycemia in certain individuals, warranting further investigation into its glycemic effects. 14
The limitations of this case report, including the lack of long-term follow-up data, absence of a control group, and reliance on intermittent blood glucose monitoring, should be acknowledged. Future research should incorporate continuous glucose monitoring and include control groups to better elucidate the effects of these medications on glycemic control in diabetic patients.
Conclusion
This study highlights the challenges in establishing a definitive causal relationship between gabapentin and blood glucose levels in diabetic patients receiving metformin therapy. While acknowledging the limited understanding of gabapentin’s impact on glycemic control, it is crucial to acknowledge the potential involvement of Nucleo C.M.P Forte in influencing blood glucose levels, an aspect initially overlooked. Future research efforts should focus on elucidating the mechanisms underlying gabapentin-induced hyperglycemia and exploring potential interactions with Nucleo C.M.P Forte and other diabetic medications. Clinicians prescribing gabapentin to diabetic patients should exercise caution, considering individual patient factors and possible drug interactions. Recommendations for clinicians include close monitoring of blood glucose levels and regular medication reviews to optimize patient outcomes and minimize the risk of adverse glycemic effects, thus enhancing patient care and safety.
Footnotes
Acknowledgements
None.
Author contributions
H.T.H.: Conceptualization; data curation; investigation; methodology; project administration. J.S.: Conceptualization; funding acquisition; resources; software; validation; visualization. N.A.: formal analysis; resources; software; supervision; validation. A.Q.M.A.: supervision; validation; visualization; writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from the ethical committee of the University of Baghdad—College of Medicine (BC1232).
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.