
Abstract
Background:
The etiology of pancreatic cancer remains elusive. Several studies have suggested a role for diabetes mellitus, but the magnitude of its contribution remains controversial.
Objectives:
Utilizing a large administrative database, this retrospective cohort study was designed to investigate the relationship between type 2 diabetes mellitus and pancreatic cancer.
Patients and design:
Using the Veterans Integrated Services Network 16 database, 322,614 subjects were enrolled in the study, including 110,919 with type 2 diabetes mellitus and 211,695 diabetes-free controls matched by gender, year of birth and healthcare facility.
Results:
A significantly higher incidence of pancreatic cancer was observed in patients with type 2 diabetes mellitus, with an adjusted hazard ratio (95% confidence interval) of 2.17 (1.70–2.77) for type 2 diabetes mellitus compared to controls (p < 10−9) after controlling for the matching factors.
Conclusion:
The association between type 2 diabetes mellitus and pancreatic cancer was statistically significant and may, in part, explain the rising incidence of pancreatic cancer.
Keywords
Introduction
Pancreatic cancer (PC) is the fourth leading cause of cancer death in the United States, with more than 40,560 expected PC-related deaths out of 48,960 cases of PC in 2015. 1 The etiology of PC remains elusive. An association with diabetes mellitus (DM) has been suggested, but a consensus has not been reached.
Several meta-analyses2–7 showed that individuals with DM have a twofold greater relative risk (RR) of developing PC than non-diabetics. The paradox that remained unanswered by these studies was the fact that the RR of PC was found to be negatively associated with the duration of DM. If the time of exposure to a risk factor for a disease is increased, it is expected that the incidence of the disease would be increased, too. However, that was not the finding of these studies; rather they showed that the RR for PC was 50% lower in individuals who had had DM for more than 5 years compared to individuals for whom the duration of DM was shorter. To explain this paradox, it is tempting to invoke the kinetics of insulin secretion in type 2 diabetes mellitus (T2DM). Growing evidence implicates hyperinsulinemia, with or without hyperglycemia, as a risk factor for developing PC. Hyperinsulinemia is characteristic of early T2DM, 8 as compared to late T2DM. Another possibility to explain this paradox might be reverse causality. Under this scenario, some of the DM cases are induced by PC, and since survival beyond 5 years is very rare in PC, we do not see this association past 5 years. This study was designed to evaluate the incidence of PC in large cohorts of patients with and without T2DM. The temporal relationship of the clinical diagnosis of DM and the diagnosis of PC was also evaluated.
Patients and methods
This study was approved by the Institutional Review Board of the Central Arkansas Veterans Healthcare Services (CAVHS) facility in Little Rock, AR. It is a retrospective cohort study utilizing the healthcare database maintained by the Veterans Integrated Services Network 16 (VISN16), which consists of 10 Veterans Health Administration (VHA) hospitals in the south-central United States. There were two planned cohorts in this study: (1) patients diagnosed with T2DM between 1 October 1996 and 31 March 2009 and (2) a control cohort of subjects with no diabetes history matched to T2DM patients by year of birth (YOB), gender and VHA hospital at a ratio of 2:1 whenever possible, or 1:1 otherwise. T2DM was defined by the treating physicians and was coded accordingly in the electronic medical record (EMR). Subjects were enrolled into a DM cohort if their EMR contained an International Classification of Diseases, 9th edition (ICD-9) code ranging from 250.00 to 250.93 and further classified as T2DM if the final digit of this ICD-9 code was even (0 or 2). Patients who carried T2DM diagnosis in their records and were on insulin were excluded from the study. Because VHA hospitals do not routinely record smoking history, subjects were instead classified for smoking status using “tobacco abuse disorder” (ICD-9 code 305.1) as a surrogate variable. Alcohol consumption data were not abstracted due to inconsistency in their reporting in the EMR.
Members of the DM cohort were entered into the study on the date of their DM diagnosis, whereas members of the control cohort were entered into the study on the date of their entry into the VISN16 database. To eliminate cases in which DM may have been induced by occult PC, we conducted a landmark analysis 9 by requiring subjects to have a minimum of 365 cancer-free days on study. When individual subjects failed this criterion, those individuals were excluded, but not the subjects matched to them. Those who survived past the 365-day landmark, denoting the end of the washout period, were followed from this landmark for the development of PC, with censoring at the date of death or last contact if no PC had developed. Incidence during follow-up was computed for each group and was defined as the number of PC occurrences divided by the total follow-up time and expressed as the number of occurrences per million person-years (MPY). The T2DM and control groups were compared for their difference in PC incidence, first by crude PC-rate ratio, then by stratified Cox regression with YOB, gender and VHA hospital as the stratification factors. Incidences of PC during each year of follow-up were computed via life-table methods and compared between groups on a year-by-year basis via pooled Z-test for the difference between two proportions. Differences in gender, YOB, age when follow-up began and prevalence of tobacco abuse disorder were compared between groups via Wilcoxon rank-sum test or Fisher’s exact test. All tests were two-sided and employed a 5% alpha significance level using Excel 2007 (Microsoft Corp., Redmond, WA) and SAS v9.1 (The SAS Institute, Cary, NC).
Results
Our database search showed that 322,614 subjects met the study inclusion criteria and survived free of cancer through the 365-day washout period, including 110,919 T2DM subjects and 211,695 controls (Table 1). Cohorts remained remarkably well-matched for gender after the washout, with 2.29% females in the T2DM group versus 2.30% females in the control group (p = 0.80). With respect to YOB, cohorts also remained well-matched after the washout, with equal medians, quartiles and minimums; the comparison p-value of p < 0.0001 was low only because of the massive sample sizes in each group. Cohorts also remained well-matched with respect to VHA facility after the washout (data not shown). The ICD-9-documented prevalence of tobacco abuse disorder, 10.67% in T2DM versus 10.91% in controls (p = 0.042), was remarkably equal between groups despite the fact that it was not a matching factor. T2DM subjects tended to be 2 years older than their controls when follow-up began (p < 0.0001).
Patient characteristics.

T2DM: type 2 diabetes mellitus.
Table 2 shows details of PC development during follow-up. The T2DM cohort had 124 PCs develop during 0.558 MPY of follow-up (222 PCs/MPY), whereas the control cohort had 140 PCs develop during 1.299 MPY of follow-up (108 PCs/MPY), yielding a crude PC-incidence ratio (95% confidence interval (CI)) of 2.06 (1.62–2.62) for T2DM compared to controls. Comparing PC incidence between groups via stratified Cox regression with stratification on the matching factors yielded an adjusted hazard ratio (HR) (95% CI) of 2.17 (1.70–2.77) for T2DM compared to controls (chi-square = 38.9, df = 1, p < 10−9) (Table 2).
Results.
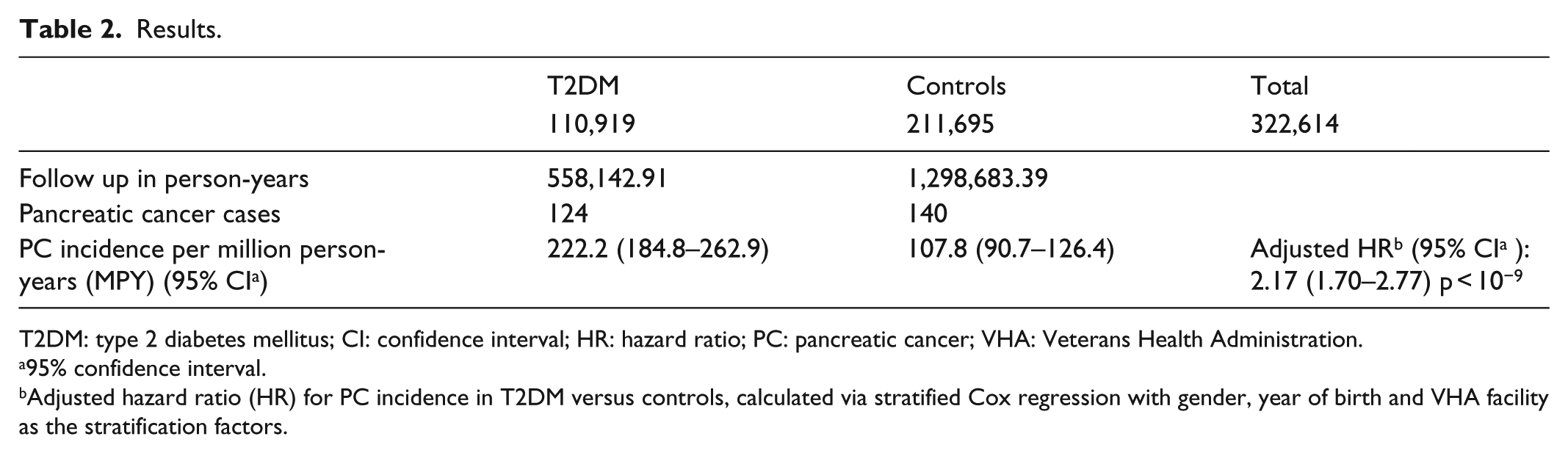
T2DM: type 2 diabetes mellitus; CI: confidence interval; HR: hazard ratio; PC: pancreatic cancer; VHA: Veterans Health Administration.
95% confidence interval.
Adjusted hazard ratio (HR) for PC incidence in T2DM versus controls, calculated via stratified Cox regression with gender, year of birth and VHA facility as the stratification factors.
The increased incidence of PC in the T2DM cohort persisted in the first few years after clinical diagnosis of T2DM. The increased incidence remained in our cohorts through the ninth year, but became statistically insignificant after the fifth year, either due to the high rate of dropout with follow-up or due to a more biologic mechanism, as discussed later (Figure 1).

The difference in the incidence of PC remained higher in T2DM than in controls, with respective PC-incidence ratios (p-values) of 1.89 (0.020), 2.56 (0.0017), 2.41 (0.0045), 2.00 (0.034) and 4.17 (0.0003) in the first, second, third, fourth and fifth year of follow-up after the 365-day landmark, respectively. Although DM patients continued to have higher PC incidence during the sixth through ninth year of follow-up, differences between the PC and control groups were not statistically significant.
There were 62 PCs diagnosed in the T2DM cohort during the 365-day washout (505/MPY). These were not included in the above analysis since they may represent the phenomenon of PC-induced DM or type 3c diabetes mellitus (T3cDM). 10
Discussion
Recent cohort studies have identified positive associations between obesity, hyperglycemia, physical inactivity and the increased risk of developing PC. 8 These findings collectively suggest that an abnormal insulin and/or glucose metabolism may be important and indirectly support the hypothesis that hyperinsulinemia contributes to the pathogenesis of PC.
Animal and in vitro studies lend strong evidence to the role of insulin in PC. Experimental studies have shown that insulin has growth-promoting and mitogenic effects on hamster, 11 rat acinar 12 and human PC cell lines in vitro.13–19 There is evidence that PC cells express insulin receptors.11–13 Insulin can also activate the insulin-like growth factor I (IGF-I) receptor, which is found on PC cells and is known to have growth-promoting effects including modulation of cell-cycle progression. 20 Hamsters pretreated with streptozotocin, which lowers insulin secretion by damaging pancreatic beta cells, showed a reduced incidence of carcinogen-induced PC.21,22 Similarly, caloric restriction, which decreases daily insulin secretion, also inhibits the induction of PC in hamsters.12,23,24
Studies of the unique vascular supply of the pancreas have shown that the exocrine parenchyma is bathed in high concentrations of islet hormones and is the first target tissue for islet hormone action. The periacinar physiologic concentrations of insulin are estimated to be at least 20-fold higher than those found in systemic circulation. 25 Patients with T2DM are known to have periods of hyperinsulinemia during the early stages of their disease 18 up to twice the normal concentrations of insulin in the blood, which essentially translates into chronic exposure of the exocrine parenchyma to even higher concentrations of insulin within the pancreas. Prolonged and continued exposure to persistently high levels of insulin may serve as a chronic trophic stimulus for the exocrine pancreas that leads to increased risk of PC during the hyperinsulinemia phase. When the beta islet cells “burn out” and patients become dependent on exogenous insulin, this trophic effect is expected to decrease with the depletion of the endogenous insulin, leading to decreased risk of PC in this population with time. 7 This study has shown an incidence pattern of PC that might lend support to this hypothesis, thereby suggesting a role for hyperinsulinemia in the genesis of PC and adding to findings from other studies 26 (see below). However, some case-control studies reached different conclusions suggesting similar PC risk across different duration of DM. 27
We excluded the 62 cases of PC that occurred in the T2DM group (of the 122,850 at risk; 50.4 per 100,000) during the initial 365-day washout period. During the same period, only 37 cases (of the 229,899 at risk; 16.18 per 100,000) were diagnosed in the control arm. We speculate that the 34.22 per 100,000-case difference between these groups might, in part, be related to reverse causality, that is, PC caused the DM (T3cDM), not the opposite. The one mechanism invoked to explain this association implicates a diabetogenic substance (islet amyloid polypeptide—IAPP—or amylin) released by the PC, the resection of which can, in some cases, lead to improvement and resolution of DM.28–30 Other possibilities include the atrophy of the normal pancreas that is usually associated with PC. It is very likely that this group of 62 patients contains a mixture of T2DM and T3cDM. Assuming that the incidence of DM-induced PC remains stable and similar during years 1–5, it is possible that two-fifths of those 62 patients had T3cDM.
Although PC incidence was elevated 1.89-fold in the first year of follow-up compared to controls, the ratio of HR of PC incidence among T2DM patients compared to controls increased to 2.5 in the second year, and remained above 2.0 through the seventh year before declining to 1.86 and 1.76 in the eighth and ninth year, respectively; however, the statistical significance of these differences failed to be maintained after the fifth year, due undoubtedly to insufficient sample sizes (i.e. not enough PC cases per year) from the sixth year onward. This increase and then decline of PC HR suggest that the risk of PC is not cumulative and is associated, not with the duration of DM, but with another factor that has a similar dynamic course, that is, rising during the early phase of T2DM then declining after the early few years. It is possible that this factor is hyperinsulinemia as suggested by Stolzenberg-Solomon et al. 26 However, it is likely that the increase in the incidence of PC in the control group starting on year 6 onward is related to age, which is a well-accepted risk factor for PC. A similar age effect is at work in the T2DM group and explains the high incidence of PC in this group as well, but it does not differ significantly from the control group (Figures 1 and 2).

In this figure the authors speculate based on their results about a possible relationship between hyperinsulinemia, T2DM, age and PC. Hyperinsulinemia precedes the rise in incidence of PC by many years. As hyperinsulinemia regresses with the advancement of T2DM, its contribution as a risk factor for PC diminishes while the role of age increases at the same time. The net result is still high incidence of PC, but it is not as high as during the early phase of T2DM and it is not statistically different from its incidence in controls where the effect of age is the main factor. Cases of PC-induced DM were excluded from the analysis. We have not measured insulin levels in this study, but we used information from other publications to build our model.31–33 PC: pancreatic cancer; there are two y-axes: the first to the left of the figure illustrates the incidence of pancreatic cancer. The second, to the right, represents insulin level. The x-axis represents age.
The results from the Finnish case-cohort prospective study conducted within the Alpha-Tocopherol, Beta-Carotene Cancer (ATBC) Prevention Study of 29,000 male smokers, aged 50–69 years, support a strong role for hyperinsulinemia and hyperglycemia as a risk factor for PC. 26 Baseline blood samples collected in the mid-80s were used to determine fasting serum glucose and insulin levels as well as insulin resistance. After 17 years, 169 men developed PC, yielding a twofold increase in the risk of developing PC among subjects with the highest fasting serum insulin/glucose levels compared to those with the lowest levels. In contrast to this study, the Finnish study showed that the association was stronger, and the risk of PC increased with longer follow-up time. It is worth noting that the Finnish study started the follow-up long time before the diagnosis of clinical DM, and the risk of PC was not evaluated before and after the diagnosis of DM. It is possible that the diagnosis of DM in the Finnish study occurred during the last 5–7 years of the study follow-up since it is known that clinical diabetes is preceded by 7–10 years of occult hyperglycemia and hyperinsulinemia. This study started the follow-up from the point of DM diagnosis. Alternatively, reverse causality may explain the association of PC with new onset DM. 34 In a large database study that included 1 million subjects, Tseng found that hyperlipidemia rather than DM was significantly associated with the diagnosis of PC. The main flaw of Tseng’s study was the short follow-up, which was limited to 3 years.
The role of other risk factors such as alcohol could not be explored in this study due to major inconsistency in collecting this information in the database that we used. Since this study is retrospective with practical impossibility to collect reliable data about alcohol consumption and in the presence of excellent prospective studies35–37 that addressed this issue, we feel that this study is not the best context to answer this question. Furthermore, the fact that heavy alcohol use is associated with increased risk of PC in smokers 36 only and the number of smokers in this study was balanced between the DM and control groups, we feel that even if the information about alcohol consumption was available it would not have changed our conclusions. The role of sex was not addressed in this study either due to the small number of female in the study population and, hence to insufficient power to perform reliable comparisons. Furthermore, data on chronic pancreatitis, a known risk factor for PC, were not available for further analysis of its role and possible interaction with DM.
The role of oral antidiabetic agents has been explored in many retrospective epidemiologic studies. A recent meta-analysis showed that the use of sulfonylurea significantly increases the risk of developing PC (by 70%), but there was no significant association between metformin, insulin or use of thiazolidinediones and the risk of developing PC. 38 Many methodological and design flaws plagued these studies, though; therefore, definitive conclusions could not be drawn. However, it is possible that metformin may have a protective role against PC or a therapeutic role after the diagnosis of PC due to its modulatory effect on the microenvironment.36,39–42 Statins were found to have a protective effect against PC. 43
Conclusion
We examined the incidence of PC in patients with T2DM. This study showed a significantly higher incidence of PC in patients with T2DM (HR: 2.17) after controlling for known risk factors. The significant association was mostly observed in the first 5 years of follow-up after the diagnosis of DM. These results strongly suggest a possibility for an etiologic role of T2DM in the pathogenesis of PC.44,45
The implications of the findings of this study on public health are clear. The incidence of obesity, metabolic syndrome and T2DM is rising and may explain the rising incidence of PC in the United States and other developed countries. Hence, any preventative program for PC must address these risk factors. Chemoprevention using drugs that decrease insulin resistance and hyperinsulinemia may have a role in preventing PC. Data to support this hypothesis, however, are lacking, and research in this area is needed.
Footnotes
Acknowledgements
The authors thank the CAVHS for its support in providing access to its database and its administrative support. Authors also thank Dorothy Graves for reviewing this manuscript.
Author contribution
I.M. helped in the study idea, protocol writing, data analysis and manuscript writing. A.Y. helped in the protocol writing, data collection and analysis. E.S. helped in the protocol writing, data analysis, statistical analysis and manuscript writing.
Availability of data and materials
A request was submitted to the VA to allow us to share the dataset that was used to conduct our analysis. The VA refused “because it contains protected health information and it is not feasible without funding to create a de-identified dataset.” Readers who are interested in more information about these analyses may contact the author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The CAVHS Institutional Review Board has reviewed this study and granted it the “exempt from individual consent” status, as it is a retrospective database review with partially de-identified data (only date of birth of the subjects was left in the dataset). Consequently, no individual consent was needed. The investigators did not have direct access to the actual medical records and all information provided to them was in the partially de-identified format. Ethical approval for this study was granted by Central Arkansas Veteran Health System Institutional Review Board as low risk study because the study is a database review with de-identified data.
Funding
This study was supported administratively by the Central Arkansas Veterans Healthcare System (CAVHS), but no funding was provided by the agency.
Informed consent
Written informed consent was waived because this study is a database review with de-identified data.