
Abstract
Background:
The risk of chronic metformin pharmacotherapy to cause vitamin B12 deficiency and its associated medical complications has been of immense concern among diabetic patients. Some studies have postulated that vitamin B12 deficiency is highly prevalent among chronic metformin-treated adult diabetic patients.
Aim:
This study aimed to determine the prevalence of vitamin B12 deficiency among metformin-treated and metformin-naïve type 2 diabetes mellitus patients.
Materials and methods:
This was a case-control, prospective, analytical, observational study of 200 adult participants (100 per group) attending the Endocrinology, Medical Out-patients Clinic of Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria. The participants’ serum vitamin B12 levels were determined using an immunoassay technique. Data were presented using tables and charts. Chi-square test was used to compare non-continuous proportional variables.
Results:
The prevalence of vitamin B12 deficiency was 41% and 20% among metformin-treated and metformin-naïve type 2 diabetes mellitus groups, respectively (p = 0.001). Borderline vitamin B12 status was present among 59% of metformin-treated group and 80% of metformin-naïve group (p = 0.001). Neither metformin-treated nor metformin-naïve groups had normal serum vitamin B12 levels.
Conclusion:
The prevalence of vitamin B12 deficiency was significantly high in diabetics, especially the metformin-treated patients. We advocate for vitamin B12 supplementation among this group of patients in order to prevent the occurrence of vitamin B12 deficiency complications such as macro-ovalocytic anemia, impaired immunity with hypersegmented neutrophils, peripheral neuropathy and subacute degeneration of the spinal cord.
Introduction
Diabetes mellitus (DM) refers to a group of common metabolic disorders that share the phenotype of hyperglycemia. 1 Several clinically distinct types of DM are caused by a complex interaction of genetics and environmental factors. Regardless of the etiology of DM, factors contributing to hyperglycemia include reduced insulin secretion, decreased glucose utilization and increased glucose production.2,3
The prevalence of DM both globally and in Nigeria has been found to be on the increase. The International Diabetes Federation estimated the prevalence of DM to be 4.6% in Nigeria.4,5 In 2016, an estimated 422 million adults globally are said to be living with DM according to World Health Organization. 3 Diet, less physical activity and increase in life expectancy are the major contributing factors to the rise in the prevalence of type 2 DM.6,7
Management of type 2 DM involves the use of several oral hypoglycaemic agents; however, metformin, which belongs to biguanide group of drugs, is widely used as the first line agent alone or with dietary modification.5,8,9 It acts by reducing hepatic glucose production and improving peripheral glucose utilization. 10 Side effects of metformin include nausea, abdominal discomfort and lactic acidosis. 11 It has been found to alter vitamin B12 absorption by various mechanisms, such as alteration of calcium-dependent membrane action required for intrinsic factor vitamin B12 complex uptake by the ileal cell membrane receptors. 12 Vitamin B12 exerts its physiological function by mediating two principal enzymatic pathways, that is, the methylation process of S-adenosyl homocysteine (SAH) to S-adenosyl methionine (SAM) and the conversion of methylmalonyl coenzyme A (CoA) to succinyl CoA 9 which enters into the Krebs cycle. The prevalence of vitamin B12 deficiency has been reported to be between 5.8% and 31%, in the United States of America, Nigeria, Netherlands and Pakistan.13,14 Metformin is one of the first-line oral hypoglycaemic agents used for the management of type 2 DM.15,16 Apart from its intensive glucose control quality, it is associated with less weight gain and fewer hypoglycaemic attacks when compared with insulin and the sulphonylureas. 17 Despite having these advantages, its potential to cause vitamin B12 deficiency has been widely reported, thereby contributing to the problems of DM such as anemia, impaired immunity, distal sensory polyneuropathy, depression disorder and cognitive impairment.18,19 More studies are needed to document the clinical impact of the deficiency in these patients. Metformin has been reported to lower vitamin B12 levels in a dose-dependent manner and based on duration of use; however, some studies did not find this to be significant. The mechanism by which metformin causes vitamin B12 deficiency has not been clearly defined; however, proposed mechanisms include alterations in small bowel motility due to hypocalcemia which results in stimulation of bacterial overgrowth with consequential vitamin B12 deficiency and competitive inactivation of vitamin B12 absorption.8,20,21 While some clinical studies have reported that metformin lowered vitamin B12 levels, other studies have reported otherwise.12,15,22 A study done in Ibadan, Nigeria found the prevalence of vitamin B12 deficiency in metformin-treated type 2 DM patients to be 8.6%.12,18 Metformin is one of the most widely used medications for the treatment of type 2 DM patients, but it has been associated with vitamin B12 deficiency and its complications such as megaloblastic (macro-ovalocytic) anemia, hypersegmented polymorphs causing immune dysfunction, peripheral neuropathy, cognitive impairment, depression and rarely subacute degeneration of the spinal cord.16–18 Furthermore, supplementation with vitamin B12 has been shown to reverse symptoms caused by vitamin B12 deficiency. 16 In sub-Saharan Africa, including Nigeria, there has been an increase in the prevalence of DM. 22 Screening tests for vitamin B12 are not readily available, and the deficiency of this vitamin has to be corrected parenterally. Overt vitamin B12 deficiency in type 2 DM patients can be detrimental, with the consequence of irreversible neuropathy; therefore, some studies have advocated for supplementation of this vitamin in DM patients with low vitamin B12 status, as this has been found to potentially reverse these complications and has been found to associate with improved patient outcomes.16,20,21 The prevalence of vitamin B12 deficiency among metformin-treated type 2 DM patients has been reported in different parts of the world;10,13,22 however, there is a paucity of data in sub-Saharan Africa, especially Nigeria.
This study was designed to determine the prevalence of vitamin B12 deficiency among metformin-treated and metformin-naïve type 2 diabetic patients attending the outpatient endocrinology clinic of Irrua Specialist Teaching Hospital (ISTH), Irrua, Edo State, Nigeria with the rational purpose of alleviating the associated morbidity and mortality.
Materials and methods
Study location and population
This study was conducted at the ISTH. It is a tertiary teaching hospital located in Irrua town, Esan Central Local Government Area in Edo State, Nigeria. The hospital is at a distance of about 87 km north of Benin City, the Edo state capital. The ISTH is a 343-bed capacity hospital involved in the management of patients and training of medical students, resident doctors and nursing students. The endocrinology clinic holds once a week with about 46 diabetic patients seen per clinic day. The study population comprised adult medical patients with type 2 DM attending the Endocrinology Out-patients Clinic at ISTH, Irrua, Edo State. Their ages were ⩾30 years and were fulfilling the inclusion criteria for recruitment, evaluation and follow-up.
Inclusion and exclusion criteria
The inclusion criteria for evaluation in this study were known adult medical patients with type 2 DM attending the Endocrinology Out-patients Clinic at ISTH, Irrua, Edo State after commencing the study, provided they granted their informed consents to participate in the study and were ⩾30 years of age. They also fulfilled the diagnostic inclusion criteria used to define type 2 DM according to the American Diabetes Association (ADA).
The exclusion criteria for this study were as follows:
Known type 1 DM patients.
Diabetic patients <30 years of age whose diagnosis of whether type 1 DM or type 2 DM were highly ambiguous and uncertain.
Patients who do not fulfill the diagnostic inclusion criteria used to define type 2 DM according to the ADA.
Adult type 2 DM patients who did not grant their informed consents to participate in the study.
Adult type 2 DM patients who, at the time of recruitment for the study, were pregnant women; purely vegetarians; receiving vitamin B12 containing supplement or chronic alcoholics (>21 units and >14 units per week for male and female for >10 years, respectively); taking cytochrome P450 microsomal enzyme inducer/inhibitor substances such as omeprazole and other proton pump inhibitors (PPIs), rifampicin, barbiturates, cimetidine, grapefruit juice, ritonavir, ketoconazole, carbamazepine or phenytoin; taking neomycin or having comorbidities such as undernutrition (body mass index (BMI) < 18.5 kg/m2), tuberculosis, benign/malignant neoplasms on chemotherapy, human immunodeficiency virus infection/acquired immunodeficiency syndrome (HIV/AIDS), chronic liver disease (CLD) and chronic kidney disease (CKD)/acute kidney injury (AKI) with estimate glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2; and having a history of irritable bowel syndrome, pernicious anemia or inflammatory bowel disorders such as Crohn’s disease or ulcerative colitis.
Adult type 2 DM patients who had done previous surgeries such as bariatric surgery, partial/total gastrectomy or partial/total ileal resection.
Patients without DM taking metformin for other medical reasons/conditions such as polycytic ovarian syndrome (PCOS) or insulin resistance syndrome.
Study design
This was a case-control, prospective, analytical, observational study.
Sample size determination
The formula for estimating sample size is as follows: 14
n = (Za2p (1–p)/e2), where n is the required sample size, Z is the critical value at 95% confidence level (1.96), p is the prevalence of vitamin B12 deficiency in patients with type 2 DM on metformin obtained from a previous study (5.8%), 15 e is the error margin that the investigator was willing to accept, and in this instance, was equal to 0.05. Note that (1–p) = q, which was the proportion of the sample population not covered by the study.
Substituting the values, we get n = 1.96 × 1.96 × 0.058 (1–0.058)/0.05 × 0.05; n = 84; n = 96 (with 10% attrition). This was rounded up to 100 patients for each group.
Sampling method
Consecutively, consented adults with type 2 DM who met the inclusion criteria for cases and controls were selected from the outpatient’s clinic at ISTH until the desired sample size was achieved. Both cases and controls were matched for age and sex.
Clinical examination
A structured questionnaire was administered to the selected participants by the researchers. The structured questionnaire contained information about socio-demographic characteristics, possible co-morbidity, surgery, alcohol ingestion, diet (vegetarian or not vegetarian), symptoms of anemia and gastrointestinal symptoms associated with vitamin B12 deficiency and medication information including the dose and duration of therapy.
All participants were made to undergo thorough clinical examination in order to document the presence of relevant hematological signs. Evidence of pallor was examined in areas like the conjunctiva, oral mucosa and palms.
Subjects’ preparation and sample collection
The laboratory assessments comprised baseline hematological parameters (hematocrit/pack cell volume (PCV) with hemoglobin concentration (Hb)) and serum vitamin B12 levels. Venepuncture site was cleaned with 70% methylated spirit and allowed to dry. In total, 10 mL of whole blood was collected from the antecubital vein of each participant. Out of this, 4 mL of venous blood was collected into a labeled vacutainer sample bottle coated inside with potassium ethylenediaminetetraacetic acid (EDTA) for PCV and Hb. The remaining 6 mL of whole blood was dispensed into a labeled plain vacutainer sample bottle, allowed to clot, centrifuged for 15 min at 3000 r/min and separated into another plain bottle for vitamin B12 assay. Freshly prepared sera were stored in aliquots of at least 4 mL at a temperature of −20°C and pooled until the desired sample size was met for analysis. Repeated freezing/thawing cycles were avoided due to constant power supply at the storage unit.
Baseline hematologic parameters
PCV and Hb were obtained using an autohematology analyzer which required blood sample drawn by the instrument (PCE-210N; ERMA Inc., Tokyo, Japan). The reference intervals for PCV and Hb parameters are as follows: Hb = 13–18 g/dL male and 11.5–16.5 g/dL female; PCV = 40%–52% male and 36%–48% female.
Measurement of vitamin B12
Vitamin B12 enzyme-linked immunosorbent assay (ELISA) assay kit (cat. no. EE-L-0010, lot AK0017APRO1014; Elabscience Biotechnology Company Ltd, China) was used for the measurement of serum vitamin B12 levels. The vitamin B12 quantitative test is based on the principle of the ELISA. The lower limit of normal for serum vitamin B12 depends on the technique used for the assay, and it is set at about 200 pg/mL (148 pmol/L). 20
Serum vitamin B12 levels less than 200 pg/mL are diagnostic of vitamin B12 deficiency, values greater than or equal to 400 pg/mL confirms absence of vitamin B12 deficiency, while values from 200 to 399 pg/mL are considered as borderline vitamin B12 status levels.21
Ethical consideration
Ethical approval for this study was obtained from the Health Research Ethical Committee of ISTH, and the assigned protocol identification number was ISTH/HREC/2016/March/026. Duly written informed consents were obtained from all cases and controls. These written informed consents were documented in the respective medical case file for each of these patients and then countersigned by each of them for appropriate record purposes. All the study participants were counseled before and after clinical assessment and serum vitamin B12 screening. In addition, they were assured of the confidentiality of all their records. This study also served to notify and treat those participants with vitamin B12 deficiency and borderline vitamin B12 status.
Data analysis
The Statistical Package for Social Sciences (SPSS®) software, version 21.0 was used for data entry, validation and analysis. Frequency distribution tables and charts were generated for the categorical variables. Tests of significance were generated for different variables. Chi-square test was used to test categorical variables, and independent t-tests were used to test the significance of means between the two groups. The level of statistical significance was defined by a value of p < 0.05.
Results
A total of 200 participants, comprising 100 metformin-treated and 100 metformin-naïve type 2 DM patients, were recruited into this study from November 2016 to September 2017. The socio-demographic parameters include age with its categorization and gender distribution. The age of the participants ranged from 31 to 80 years with a mean of 55.80 ± 9.3 years. Majority of the participants, 39 (39%) for metformin-treated type 2 DM patients and 37 (37%) for metformin-naïve type 2 DM patients, were between the age group of 51–60 years. Both groups were matched for age and gender. This is represented in Table 1 alongside with other socio-demographic profiles of the participants. Furthermore, Table 1 shows that 49% versus 51% among the metformin-treated group were males and females, respectively; the opposite was recorded for the metformin-naïve group. Majority of the participants were married (96%) and had income less than 100 dollars per month.
Socio-demographic profiles of metformin-treated and metformin-naïve type 2 DM groups.

Chi-squared test, p < 0.05 is statistically significant.
The mean for age, height and weight was higher for male participants when compared with their female counterparts ((58.8 ± 8.9 years versus 56.1 ± 9.4 years; p = 0.316), (1.62 ± 0.08 m versus 1.59 ± 0.07 m; p = 0.512), (67.5 ± 8.9 kg versus 66.7 ± 8.8 kg; p = 0.408) for males and females, respectively). However, the opposite was observed concerning the mean for BMI (25.7 ± 2.8 kg/m2 versus 26.4 ± 3.6 kg/m2; p = 0.491) and duration of DM diagnosis (4.92 ± 4.5 years versus 5.14 ± 4.9 years; p = 0.705) for males and females, respectively, although all their p-values were not statistically significant.
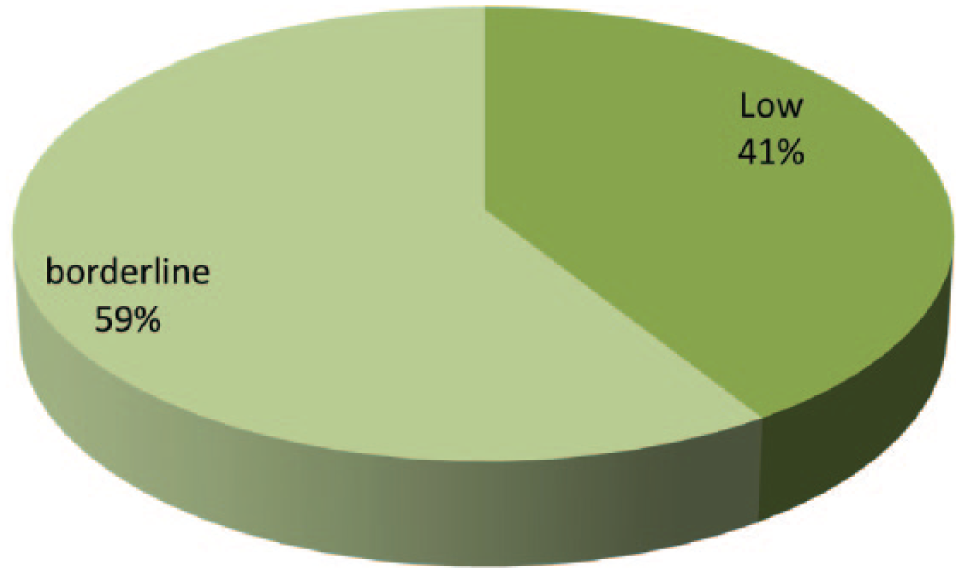
Figures 1 and 2 show the respective prevalence rates for vitamin B12 deficiency among metformin-treated and metformin-naïve type 2 diabetes patients. The prevalence rates for vitamin B12 deficiency among the metformin-treated and metformin-naïve type 2 diabetes patients were 41% and 20%, respectively, which revealed a statistically significant association between both groups (p = 0.001).

Prevalence of vitamin B12 deficiency among metformin-treated type 2 diabetic patients.
Prevalence of vitamin B12 deficiency among metformin-naïve type 2 diabetic patients.
Table 2 shows the frequency distribution and mean for serum vitamin B12 levels between the metformin-treated and metformin-naïve type 2 DM groups. The frequency of serum vitamin B12 deficiency was 41% versus 20% for metformin-treated and metformin-naïve groups, respectively (p = 0.001). Borderline status was recorded for 59% versus 80% for metformin-treated and metformin-naïve groups, respectively. In participants with frank vitamin B12 deficiency (i.e. mean serum vitamin B12 level ⩽ 199 pg/mL), the mean serum vitamin B12 for metformin-treated group was lower compared with that for metformin-naïve (158.29 ± 29.27 pg/mL versus 173.95 ± 14.21 pg/mL, respectively, p = 0.028), as with borderline status and total serum vitamin B12 values too.
Frequency distribution and mean for serum vitamin B12 levels between the metformin-treated and metformin-naïve type 2 DM groups.

SD: standard deviation.
p < 0.05 is statistically significant.
Independent t-test.
Chi-squared test.
The peripheral neuropathy components assessed during this study comprised pain sensation, light touch sensation, vibration sense, joint position sense, knee and ankle jerks and planter reflex response. So, peripheral neuropathy assessment is not a single entity. The statistically significant components of peripheral neuropathy evaluated during this study were impaired pain sense (paraesthesias), impaired light touch sense and impaired vibration sense among the metformin-treated group versus metformin-naïve group with their respective prevalence rates of 86% versus 39% (p < 0.001), 83% versus 39% (p < 0.001) and 83% versus 43% (p < 0.001). Table 3 depicts this illustration.
The respective prevalence rates for statistically significant components of peripheral neuropathy evaluated during this study.

p < 0.05 is statistically significant.
In addition, the prevalence rates for frank anemia (PCV value < 30% with Hb < 10 g/dL) among the metformin-treated and metformin-naïve type 2 diabetes patients were 29% and 14%, respectively, which revealed a statistically significant difference between both groups (p < 0.05).
Concerning the occurrence of oval macrocytic red blood cells in the peripheral blood films of the study participants, the prevalence rates of ovalocytosis among the metformin-treated and metformin-naïve participants were 18% versus 6%, respectively (p = 0.009), while the prevalence rates of macrocytosis were 5% versus 0% among the metformin-treated and metformin-naïve participants, respectively (p = 0.06). A high mean cell volume (MCV) was recorded for very few participants (i.e. 5%) in the metformin-treated group, but it was normal for all the participants in the metformin-naïve group.
Both case and control groups had fair glucose control using their mean fasting plasma glucose (FPG) at presentation during diagnosis versus recruitment contact for sample collections in this study. The mean FPG at presentation during diagnosis versus recruitment contact for sample collections in this study among the metformin-treated group was 167.8 ± 29.1 mg/dL versus 140.8 ± 60.2 mg/dL (p ⩽ 0.001), respectively, while among the metformin-naïve group, it was 186.8 ± 33.4 mg/dL versus 128.1 ± 42.1 mg/dL (p ⩽ 0.001), respectively. Therefore, the glycaemic index for the participants at the recruitment contact for sample collections in this study may not have likely impacted the outcome of our findings, since their mean FPG levels revealed that they were better controlled.
Moreover, there was no statistically significant correlation (r = 0.77, p = 0.45) between the increasing doses of metformin and serum vitamin B12 levels. In addition, there was no statistically significant correlation between the duration of metformin use and serum vitamin B12 levels (r = 0.002, p = 0.98).
In this study, regarding the metformin-naïve participants, 70% were on insulin alone, 10% were on pioglitazone and vidagliptin, 10% were on pioglitazone and glibenclamide, 5% were on pioglitazone and glimepiride, while the remaining 5% were on glibenclamide alone. Concerning the metformin-treated participants, 70% were on metformin and glibenclamide; 10% were on metformin and glimepiride; 5% were on metformin and vidagliptin; 5% were on metformin, vidagliptin and pioglitazone; 5% were on metformin, glibenclamide and pioglitazone; while the remaining 5% were on metformin, glimepiride and pioglitazone. All the participants were also on dietary measures too.
Discussion
This case-control, prospective, analytical, observational study aimed at determining the prevalence of vitamin B12 deficiency among metformin-treated and metformin-naïve type 2 DM patients; it also compared the prevalence rates of frank anemia (which is one of the clinical and laboratory features of vitamin B12 deficiency) among both groups. The study enrolled 200 participants for about 11 months, which comprised 100 metformin-treated and 100 metformin-naïve type 2 DM patients. The specific socio-demographic parameters were age, gender, occupation and income. Both groups of participants were matched for age and gender. The mean age of metformin-treated group was 59.20 ± 8.92 years, compared to metformin-naïve group with a mean age of 55.33 ± 9.19 years. Matching both groups for age was quite important because the risk of developing metformin treatment–induced vitamin B12 deficiency was significantly being influenced by increasing age, as 20% of elderly people without DM in a previous study were reported to have vitamin B12 deficiency. 8 The prevalence rates for vitamin B12 deficiency among type 2 DM patients attending endocrinology clinic at ISTH were 41% versus 20% in metformin-treated and metformin-naïve participants, respectively. Majority of the participants had borderline vitamin B12 status, that is, 59% for metformin-treated group and 80% for metformin-naïve group. The implication of this finding is that these categories of patients may be tilted into vitamin B12 deficiency if started on metformin pharmacotherapy. A study done by Osifo et al. 22 on serum cobalamin reference values among 240 healthy Nigerians revealed a mean cobalamin level of 554 ± 202 pmol/L (150.89 ± 55.02 pg/mL) with a reference value of 290–1150 pmol/L (78.9–313 pg/mL) versus 615 ± 258 pmol/L (167.51 ± 70.27 pg/mL) with a reference value of 280–1400 pmol/L (70.3–381.33 pg/mL) among males and females, respectively; however, no cut-off for vitamin B12 deficiency was defined. The mean total serum vitamin B12 level of 210.22 ± 58.18 pg/mL and 273.57 ± 84.44 pg/mL for metformin-treated and metformin-naïve groups, respectively, (p = 0.0001) was reported in this study, with vitamin B12 deficiency defined as values below 200 pg/mL. The prevalence of vitamin B12 deficiency among metformin-treated type 2 DM patients in this study (i.e. 41%) is significantly higher than the value reported by Akinlade et al. 12 of the University College Hospital Ibadan, who found a prevalence of 8.6% in a cross-sectional study of 81 metformin-treated type 2 DM patients. Other studies by Reinstatler et al., 10 De Groot-Kamphuis et al. 11 and Iftikhar et al. 13 also reported lower prevalence of vitamin B12 deficiency in metformin-treated type 2 DM patients. The differences in the prevalence of vitamin B12 deficiency among this study’s participants could be attributed to rural dwelling and low income of the participants, methodological differences in serum vitamin B12 determination and different cut-off values for vitamin B12 deficiency. This study employed the use of ELISA for serum vitamin B12 assay, which is the standard recommended screening modality for suspected cases of vitamin B12 deficiency. 20 Vitamin B12 deficiency was also reported for 20% of the participants who were metformin-naïve. Though it appears that there is paucity of adequate data regarding vitamin B12 deficiency in adult Nigerians without diabetes, it has been well documented in approximately 20% elderly patients aged 60 years and above in developed countries. 8 This study revealed that 9.8% of elderly diabetic patients aged 60 years and above were vitamin B12 deficient. It may therefore be appropriate to advocate for vitamin B12 screening prior to metformin use, as administration of metformin in the presence of preexisting vitamin B12 deficiency or borderline vitamin B12 status will likely worsen deficiency state and treatment outcomes. 16 The mean total serum vitamin B12 level for metformin-treated type 2 DM participants was significantly lower than the value for metformin-naïve type 2 DM participants (210.22 ± 58.18 pg/mL versus 273.57 ± 84.44 pg/mL; p = 0.0001). This finding was also consistent with the report by Reinstatler et al., 10 who analyzed data from American adults who were more than 50 years of age with type 2 DM taking metformin, type 2 DM not taking metformin and those without diabetes.
Finally, the limitation of this study was that the patients were not followed up for a longer period of time to ensure drug compliance. In addition, the serum vitamin B12 measurement was done at one particular point in time as it was a short time prospective observational study of about 11 months. It also aimed to look at the effect of chronic metformin therapy on serum vitamin B12 levels, but not folate. Chronic metformin therapy does not contribute to folate deficiency; however, folate deficiency may have contributed to megaloblastic (macro-ovalocytic) anemia among some of the participants, but this was not within the scope of our study design. This study did not assess for the level of HbA1c among the participants since it was not part of the scope of this research work. In addition, the glycaemic index for the participants at recruitment contact for sample collections in this study may not have likely impacted the outcome of our findings, because their mean FPG levels revealed that they were better controlled.
Conclusion
This study has brought to limelight the sub-normal serum levels of vitamin B12 among all patients with type 2 DM, which was more profound among metformin-treated participants compared to metformin-naïve participants. We recommend vitamin B12 supplementation in metformin-treated type 2 diabetes patients in order to prevent the occurrence of vitamin B12 deficiency complications such as macro-ovalocytic anemia, impaired immunity with hypersegmented neutrophils, peripheral neuropathy and subacute degeneration of the spinal cord.
Footnotes
Acknowledgements
The authors would like to thank and appreciate all the staff at outpatient Endocrinology Clinic of Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria for their immense assistance during the course of this study. Their support was of paramount importance to the completion of this study.
Author contributions
The authors alone are responsible for the contents and writing of this research manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Health Research Ethical Committee of Irrua Specialist Teaching Hospital Irrua (ISTH), and the assigned protocol identification number was ISTH/HREC/2016/March/026.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Duly written informed consents were obtained from all cases and controls. These written informed consents were documented in the respective medical case file for each of these patients and then countersigned by each of them for appropriate record purposes. All the study participants were counseled before and after clinical assessment and serum vitamin B12 screening. In addition, they were assured of the confidentiality of all their records. This study also served to notify and treat those participants with vitamin B12 deficiency and borderline vitamin B12 status.