
Abstract
Malignant otitis externa (skull base osteomyelitis) can be fatal and long-term antibiotic therapy is recommended. Despite being potentially fatal, this infection causes minor changes in inflammatory biomarkers (white blood cell count and C-reactive protein levels) upon blood testing. Computed tomography and magnetic resonance imaging changes persist over a long period. Therefore, it is difficult to determine the optimal time for the discontinuation of antibiotics. We present a 77-year-old male whose medical history included type 2 diabetes mellitus who suffered from chronic otitis media with Pseudomonas aeruginosa infection. His condition did not improve with proper treatment, and imaging revealed malignant otitis media. Intravenous cefepime treatment was administered. Antibiotic treatment was de-escalated to oral levofloxacin treatment after Gallium-67 scintigraphy showed less accumulation after 6 weeks of Cefepime administration; accumulation almost disappeared after 1 year. In this report, we describe the usefulness of gallium scintigraphy in the evaluation of malignant otitis externa.
Keywords
Introduction
Malignant external otitis is characterized by necrotizing otitis externa and typically occurs in elderly patients with diabetes or Pseudomonas aeruginosa infections. Recently, various fungi and bacteria have been reported as causative agents. This disease is also referred to as skull base osteomyelitis (SBO) because the inflammation extends to the surrounding tissues, especially to the bones of the skull base, causing a variety of cranial nerve symptoms. It is important to differentiate it from otitis media with antineutrophilic cytoplasmic antibody (ANCA)-associated vasculitis, eosinophilic otitis media, tumors, and tuberculosis. Disease outcomes are statistically poor; therefore, early differential diagnosis and intervention are important. If the disease is not diagnosed and treated appropriately at an early stage, it is likely to cause neurological symptoms and intracranial complications, leading to death. The mortality rate is 22.5%, and in Japanese reports the relapse rate is 42.5%. 1 Although long-term antibiotic therapy is recommended, it is difficult to determine the optimal time for the discontinuation of antibiotics, considering the high recurrence rates.
The usefulness of nuclear medicine examinations, such as gallium scintigraphy, has been reported 2 ; however, there are no reports on the chronological course of the disease assessed by gallium scintigraphy. We report a case in which the patient was treated with antibacterial agents for a long period of time, during which the course of treatment was evaluated by gallium scintigraphy. The patient was eventually cured.
Case report
A 77-year-old male presented with left-sided earache and otorrhea. The patient was treated for chronic otitis media at an ear-nose-throat clinic for 1 month. However, his condition did not improve, and he was referred to our department. His medical history included uncontrolled type 2 diabetes mellitus.
Otoscopic examination revealed purulent otorrhea and granulation tissue in the tympanic membrane. Pathological examination of the granulation tissue revealed no malignancy or inflammation. Initial laboratory examination revealed negative results for ANCA-associated vasculitis and tuberculous otitis media. Bacterial examination of the otorrhea revealed Pseudomonas aeruginosa. Temporal bone computed tomography (CT) revealed abnormal opacification in the middle ear cavity, but the cortical bone was not destroyed.
He was admitted to our hospital for surgical treatment and left tympanoplasty (IIIc), and mastoidectomy was performed for debridement of the middle ear. The middle ear and mastoid cavity were filled with inflamed granulation tissue.
Intraoperative middle ear specimens showed only inflammatory findings. The patient's symptoms were temporarily relieved after surgery; however, the pain soon recurred and worsened 12 days after the operation. Otoscopic findings revealed bone necrosis in the external auditory canal, and a temporal bone CT scan with contrast showed bone destruction of the cortical bone at the apex of the temporal bone and clivus (Figure 1). Contrast-enhanced magnetic resonance imaging (MRI) revealed a contrast effect on the left side of the nasopharynx (Figure 2), and gallium scintigraphy showed significant accumulation of the radiotracer in the left skull base (Figure 3). Cefepime (CFPM) treatment was initiated for a diagnosis of malignant SBO. No symptoms involving the lower cranial nerve were observed. Gallium-67 scintigraphy showed less accumulation after 6 weeks of intravenous CFPM treatment. There was a mild inflammatory response at the time of SBO diagnosis, which promptly improved. Antibiotic treatment was de-escalated to oral levofloxacin (LVFX) treatment, and the patient was discharged.

(a) Contrast-enhanced temporal bone computed tomography (CT). Bone destruction in the cortical bone at the apex of the temporal bone and clivus can be seen. (circle) (b) A heterogeneously enhancing soft-tissue lesion involving the left nasopharynx can be observed in contrast-enhanced CT (circle).

(a) Contrast-enhanced magnetic resonance imaging (MRI). Contrast effect observed on the left side of the nasopharynx in enhanced T1 weighted MR image. (circle) (b) Slight hyperintensity is shown on the nasopharyngeal soft tissue in diffusion-Weighted Imaging (DWI). (c) Relative low Apparent diffusion coefficient (ADC) values can be observed on the nasopharyngeal soft tissue in ADC. (d) No neoplastic lesions can be observed on the nasopharyngeal soft tissue in FLAIR.
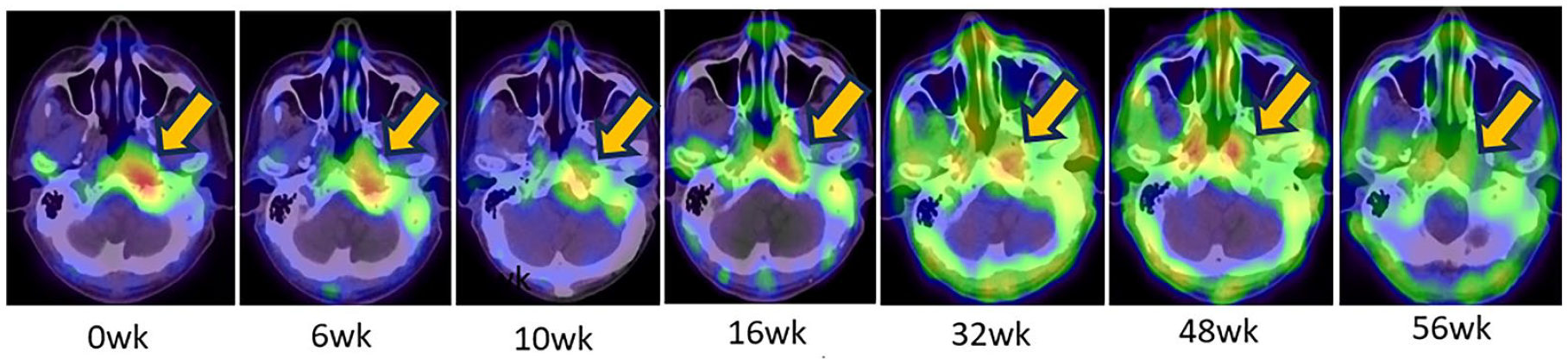
Ga scintigraphy Gallium scintigraphy was performed every 6–8 weeks. Gallium scintigraphy showed a reduction in the gradual accumulation (arrows), which almost disappeared after 1 year of cefepime administration.
The patient was closely monitored with gallium scintigraphy every 6–8 weeks, in addition to the monitoring of symptoms, otoscopic findings (Figure 4), and laboratory tests (Figure 5). Gallium scintigraphy showed a less gradual accumulation that almost disappeared after 1 year of CFPM administration. We considered that the patient was cured, and oral antibiotic treatment was discontinued. Gallium scintigraphy performed 8 weeks after discontinuation showed no recurrence.

Otoscopic findings. Bone necrosis was observed in the external auditory canal. Six weeks after skull base osteomyelitis treatment, the patient’s condition improved.

Antibiotic therapy and inflammation (0 weeks (wk): at the time of skull base osteomyelitis (SBO) diagnosis). There was a mild inflammatory response at the time of SBO diagnosis, which promptly improved. CFPM: cefepime, LVFX: levofloxacin.
Discussion
Malignant external otitis (SBO) is a rare refractory and potentially fatal disease. Temporal bone CT shows abnormal opacification in the middle ear and cortical dehiscence, which requires differentiation from malignancy. Biopsy of granulation tissue allows for the differentiation from nonmalignant granulomatous lesions (tuberculosis, ANCA-associated vasculitis, eosinophilic otitis media, etc.); however, comprehensive judgment is important when the samples are inadequate for diagnosis. Otorrhea should be cultured to identify causative agents and antimicrobial sensitivity. Adequate antimicrobial therapy is recommended for 3–6 months. 3
Pseudomonas aeruginosa accounts for 90% of the causative agents of SBO, and it is important to select antimicrobial agents that are effective against Pseudomonas aeruginosa. In recent years, there have been reports of other causative agents, including Staphylococcus aureus, Klebsiella spp., Salmonella spp., Mycobacterium tuberculosis, and Mycosis.4,5 In our case, the patient was elderly with diabetes mellitus and infected with Pseudomonas aeruginosa, which is generally accepted to cause SBO. Antimicrobial agents are the first choice of treatment, and there are many opinions that limit surgical treatment, such as not shortening the duration of antimicrobial therapy, 6 which can result in possible adverse effects through the spread of pathogens to normal bone. 7 Surgical intervention is useful for obtaining specimens for diagnosis, while it has limited value for treatment.8,9
In the present case, surgery was initially performed; however, the patient's condition worsened after only a temporary remission. Imaging evaluation may have been necessary before surgery. The use of lesion to non-lesion count ratios in 4-h, 24-h, or 24-h/4-h single-photon emission computerized tomography bone scintigraphy is reported to be useful in distinguishing between patients with malignant external otitis and external otitis in patients with early diabetes. 10 In addition, 99mTc-mononuclear leukocytes are reported to be highly specific for malignant external otitis diagnosis. 11 These alternative imaging methods might be considered in our case.
Although monthly/yearly long-term antibiotic therapy is recommended, it is difficult to determine the optimal time for the discontinuation of antibiotics, considering the high recurrence rates. Although potentially fatal, this infection causes minor changes in inflammatory biomarkers (white blood cell count and C-reactive protein levels) upon blood testing. CT is useful for the initial evaluation. 12 However, CT imaging changes persist over a long period; therefore, it is difficult to determine the inflammatory response using blood tests and CT imaging. 13 MRI is superior for evaluating the extent of soft-tissue and marrow involvement. In addition, MRI is useful for differentiating between carcinoma, lymphoma, and abscess. 2 However, it is considered unsuitable for disease assessment because of its long-term residual effect. As it is difficult to evaluate disease status by imaging changes, nuclear medicine is considered effective in assessing the functionality of the disease.
Nuclear medicine tests include gamma tracers, such as technetium and gallium, and beta tracers, such as fludeoxyglucose F18. Technetium scintigraphy reflects the activity of osteoblasts caused by the infection. Although it is sensitive and suitable for the initial diagnosis, it is not suitable for determining the efficacy of treatment because the activity of osteoblasts increases during the process of bone repair even after treatment, and abnormal findings persist for a long period of time. 14 Gallium scintigraphy targets the acute-phase reactant proteins and reflects the immune response to infection. Moreover, it can be evaluated over time to confirm that there is a decrease in the accumulation of the tracer in the lesion, and that the disease is considered to be cured. 2 The advantage of gallium scintigraphy is that its uptake disappears soon after the inflammation improves, and it has excellent spatial resolution. However, gallium scintigraphy may have a limited value for the initial diagnosis due to the poor specificity of nuclear medicine. 15
Recently, the usefulness of positron emission tomography-computed tomography (PET-CT) and PET-MRI using beta-tracers has been reported.9,16 However, PET-CT may yield false-negative results when a fungus is the causative agent. 17
The usefulness of dynamic contrast-enhanced MRI parameters and apparent diffusion coefficients as treatment response markers has also been reported 18 ; these may serve as markers for disease status assessment.
The suggestions regarding the timing of follow-up vary from imaging when new clinical symptoms present, to imaging every 6 weeks in order to monitor for relapse. 19 Due to the high mortality and relapse rate of SBO, especially during the first year after treatment, we should monitor the disease progression as frequently as we possibly can. However, radioprotection issues must be considered, as imaging needs to be repeated for disease monitoring.
Gallium provides patients with higher radiation doses compared to other white blood cell radiotracers (approximately 15 mSV in each imaging round). 20 Although the usefulness of gallium scintigraphy for disease monitoring has been demonstrated, this imaging approach exposes patients to high levels of radiation. Moreover, gallium scintigraphy is not a cost-effective imaging modality for monitoring the disease after the antibiotic treatment has been de-escalated. Considering the radiation exposure, we suggest that gallium scintigraphy should be repeated to determine the response to the first intravenous antibiotics treatment before discharge, or when disease relapse is suspected based on symptoms, otoscopic findings, and imaging (CT, MRI) findings after discharge.
PET/CT provides as high radiation exposure as gallium considering the radiation from CT,21,22 which is not suitable for long-term monitoring considering radiation exposure. PET/MRI is not widely available nowadays, but we believe that this modality is the most favorable imaging follow-up method considering radioprotection.
The findings of SBO on gallium scintigraphy persisted for a long period after treatment, even after the otoscopy findings resolved and the patient’s symptoms eased. This case suggests that evaluating the state of malignant external otitis based on inflammatory blood tests and otoscopic findings is difficult. In this case, the disease was evaluated using gallium scintigraphy, and the patient was cured without recurrence, even after discontinuation of antibiotics. Although the usefulness of gallium scintigraphy has been demonstrated, radioprotection issues should be considered as imaging needs to be repeated for disease monitoring. Therefore, we suggest that gallium scintigraphy should be repeated to monitor the response to the first intravenous antibiotics treatment before discharge, or when disease relapse is clinically suspected.
Conclusion
Here, we describe a case of malignant external otitis that was successfully controlled using long-term antibiotic therapy. Although long-term antibiotic therapy is often required, the high rate of recurrence makes it difficult to determine when antibiotic therapy should be terminated. Malignant external otitis is difficult to evaluate based on inflammatory and otoscopic findings, suggesting the importance of qualitatively evaluating inflammation using gallium scintigraphy. Considering radiation exposure, we suggest that gallium scintigraphy should be repeated to determine the response to the first intravenous antibiotics treatment before discharge, or when disease relapse is clinically suspected.
Footnotes
Acknowledgements
Author contributions
The paper was coauthored by R.T., T.I., R.A., K.M., S.A., and K.T. T.Y. contributed to the conception, design, and drafting the work. R.A., K.M., and S.A. contributed to the acquisition of data. R.T. and T.I. contributed to critically revising the work for important intellectual content. K.T. contributed to critically revising the work for important intellectual content and provided the final approval for the version of the manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Study approval statement
This case study followed the protocol of the World Medical Association Declaration of Helsinki. The paper was exempt from ethical committee approval, since case reports are exempt from committee review.
Informed consent
Informed consent, in written form, was obtained from the participants for the publication of the details of their medical case.