
Abstract
Bizarre parosteal osteochondromatous proliferations, also known as Nora’s lesions, are rare benign tumors with a high recurrence rate. They are often difficult to identify because of their similar appearance to other tumors. We describe a 25-year-old healthy female patient with bizarre parosteal osteochondromatous proliferations in an uncommon location on the pelvic ilium, presenting with unique clinical findings of abdominal pain and femoral paresthesia and showing atypical radiographic findings. To the best of our knowledge, this is one of the very few cases ever reported in the literature of Nora’s lesion in this particular location and possibly the first case ever with this specific presentation. The lesions’ radiographic images, combined orthopedic and general surgery procedures, and histological analysis are detailed. The patient’s continued 4-year follow-up has demonstrated no symptoms or evidence of recurrence.
Introduction
Bizarre parosteal osteochondromatous proliferation (BPOP), first described by Nora et al. in 1983 (and therefore also known as Nora’s lesion), is an extremely rare tumor. It is defined as a “well-marginated mass of heterotopic mineralization arising from the periosteal aspect of an intact cortex, without medullary changes.” 1 There is limited epidemiological data on the incidence of BPOP due to its extreme rarity (less than 350 cases described in literature since its discovery). 2 The tumor has an unexplained remarkable tendency to recur after excision with reported rates between ~30% and 60%3–5 BPOP typically affects the surfaces of bones in the hands and feet, usually the phalanges, metacarpals, and metatarsals. However, in the literature, uncommon sites have also been reported, such as the distal humerus, radius, ulna, fibula, hallux sesamoid, tibia, and greater trochanter of the femur. It does not usually cause significant symptoms and has a low risk of morbidity and negligible mortality. It can cause local symptoms attributable to a mass effect on adjacent anatomical structures. 3
In this article, we report a clinical case of this rare BPOP diagnosed on the ilium of a patient with a unique symptomatic presentation from the tumor’s protrusion into her abdomen. To the best of our knowledge, this is one of a few individual cases of this tumor to ever be reported being located in the pelvis.
Case report
A 25-year-old, single female student presented to our clinic with 6 years of lower back and right lower quadrant abdominal pain. In addition, the patient described a worsening anterior right leg numbness after walking short distances. The patient had no medical history of note and no significant family history. She had no history of fever, trauma, night sweats, or weight loss. On physical exam, the patient had a large palpable mass on her right iliac wing, which protruded inwards in the direction of the psoas muscle. The abdomen was non-tender, and the remainder of her physical exam was unremarkable.
The abdominal computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated an exophytic mass with no obvious bone destruction and with clear, well-defined borders. The expansile lesion originated from the superior-medial aspect of the right iliac crest with a maximum diameter of about 7 cm. There was a narrow and short continuity of the medullary canal of the ilium to the base of the lesion (discussed further in the Discussion section). Both intramedullary and soft tissue edema were present, and the lesion demonstrated enhancement with a contrast agent. There was a mass effect with pressure on the right psoas muscle (Figures 1(a)–(c) and 2(a), (b)).

(a–c) Axial, sagittal, and coronal computed tomography slices of the mass protruding from the right ilium. The red arrow shows the small medullary continuity at the base of the tumor (green star = BPOP, yellow arrow = psoas muscle, orange circle = colon, blue rectangle = kidney).
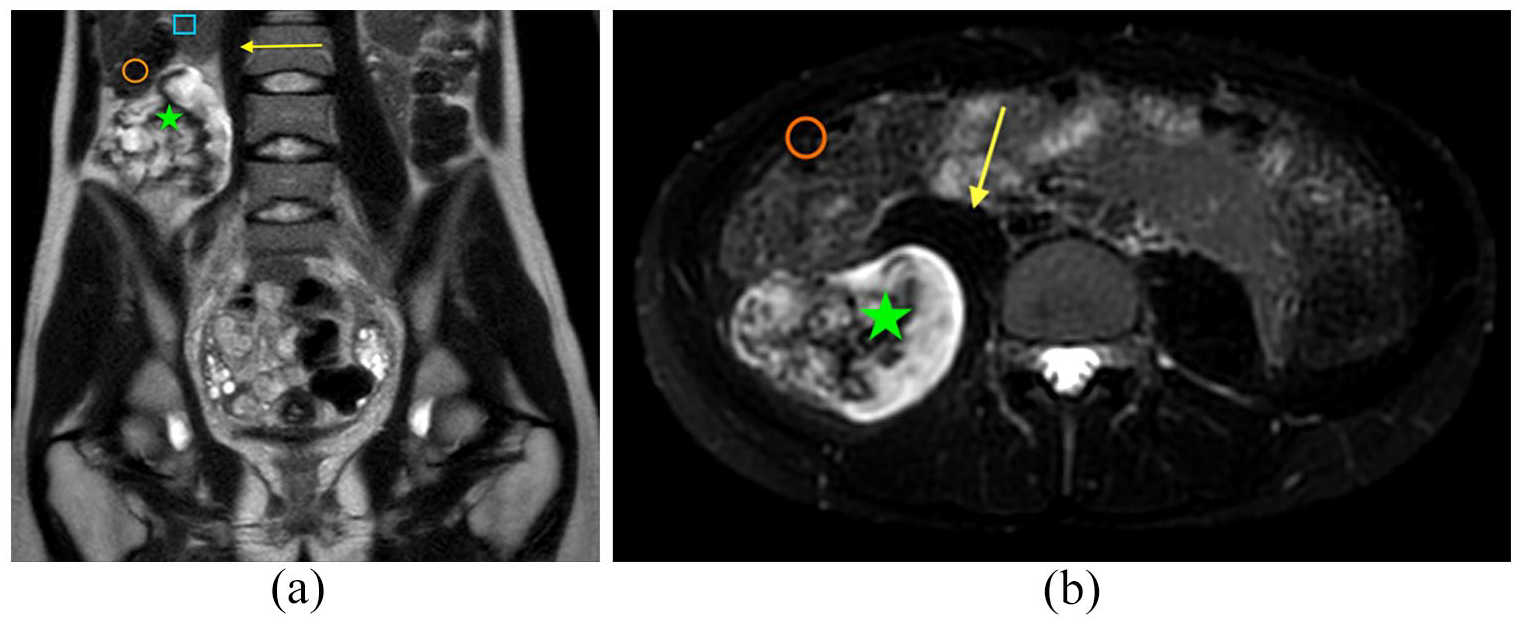
(a and b) Magnetic resonance imaging T1 and T2 images of the lesion (green star = BPOP, yellow arrow = psoas muscle, orange circle = colon, blue rectangle = kidney).
After a multidisciplinary meeting as well as in-depth discussions with the patient, it was decided to proceed with surgical excision. A joint general surgery and orthopedic procedure was planned to remove the tumor. Under general anesthesia, with the patient lying on her left side, a laparoscopically assisted open marginal excision was performed: Two laparoscopic portals were introduced on the right side of the abdomen, and the tumor was found to be pushing on the right colon anteriorly and the right kidney superiorly. It extended beyond the psoas muscle and reached the right retroperitoneum. The right colon was mobilized, and the tumor was divided off the right kidney, mesocolon, and the psoas muscle. At this stage, a separate incision was made over the posterior right ilium, and dissection extended to the base of the tumor, which was removed with an osteotome (Figures 3–5). Hemostasis was achieved, and a laparoscopic self-fixating mesh (ProGrip, manufactured by Medtronic) was positioned prophylactically to prevent a hernia between the ilium and lateral abdominal muscles. The wound was closed with monocryl. Post-operative recovery was unremarkable.
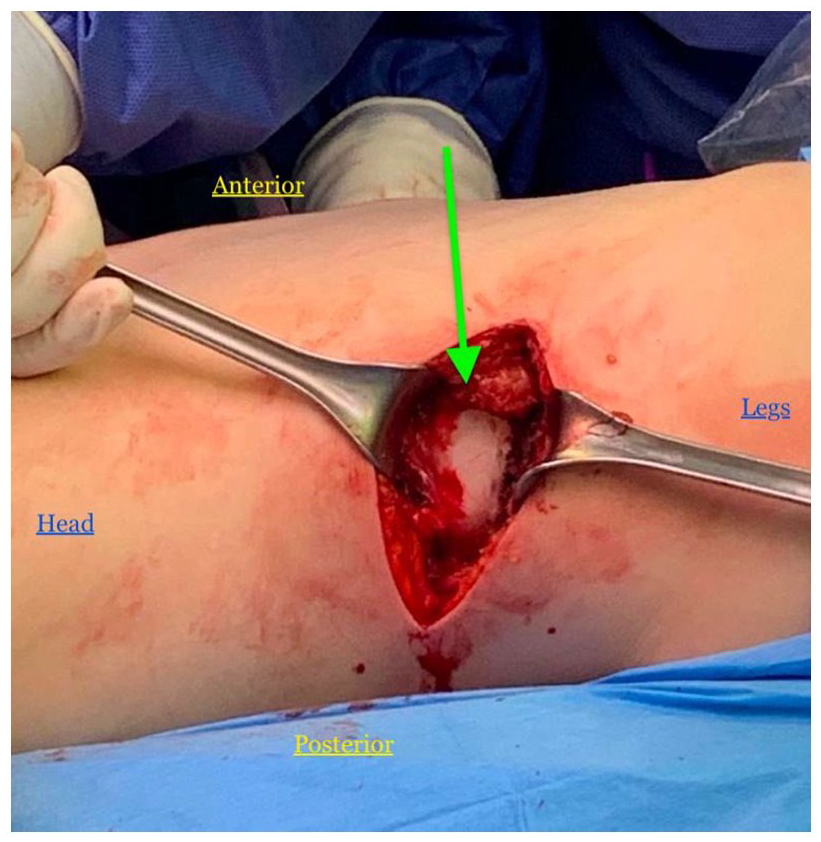
View of the lesion through the incision over the posterior right ilium. The patient was lying on her left side (position and direction labeled). The head of the BPOP tumor is visualized (arrow).

Retractors holding the incision open as the BPOP (a star is next to the base of the tumor) is marginally excised with an osteotome.

The fully excised Nora’s lesion before being sent to pathology analysis.
The tumor was sent for pathological analysis. Macroscopic examination revealed a sessile exophytic mass measuring 8 × 6 × 5.5 cm and composed of a thick, exuberant cartilage cap and bone tissue at the base of the lesion. On the microscopic examination, the lesion consisted of a heterogenous disorganized mixture of cellular cartilage, bone, and loose fibrovascular stroma. The cartilage was irregularly calcified and composed of enlarged, bizarre chondrocytes. The maturation of the cartilage into the chondro-osteoid matrix with characteristic blue quality, known as “blue bone,” was also evident. The spindle cell proliferation in the fibrovascular stroma was without atypia. The pathology and histology report of the right ilium mass demonstrated characteristics compatible with a BPOP, confirming the diagnosis. (Figures 6–8)

Panoramic view: Mixture of cellular cartilaginous tissue and bone (H& E, original magnification × 12.5).

Bizarre binucleated chondrocytes (H& E, original magnification × 100) (red arrow indicates example).

Characteristic transition from one tissue type to another (chondro-osseous metaplasia), resulting in the formation of the “blue bone” (H& E, original magnification × 40).
The patient’s wounds healed well, and the patient had an uneventful post-op follow-up with no complications. The femoral paresthesia subsided, and the abdominal discomfort resolved. There were no renal/urinary symptoms or complications observed following the surgery. The patient was closely followed up jointly in the orthopedic and general surgery clinics through physical exams and imaging. Every 6 months, an X-ray or advanced imaging (CT or MRI) was performed. At the 4-year follow-up, the patient was symptom-free and showed no evidence of recurrence.
Discussion
We have presented a case of BPOP with an extremely rare presentation that underwent surgical management and an uneventful follow-up with no recurrence. This case’s details, compared to the typical characteristics of a BPOP, demonstrate the uniqueness of this patient’s tumor.
The patient presented at the age of 25 with no significant trigger or trauma. BPOP is most common in the second and third decades of life, with a few case reports affecting infants and the elderly. 1 There does not appear to be a sexual predominance either. Additionally, it is noteworthy that the patient had no history of trauma, as BPOP has been reported as resulting from a previous trauma in close to 50% of the cases.2,6 That being said, preceding traumatic events are found inconsistently in the literature, and the etiology of BPOP is still uncertain. 7 Recent articles have described chromosomal rearrangements and, in particular, of a translocation t (1; 17) in some BPOP tumors, which would favor a neoplastic nature etiology. 3
Although mostly described as an asymptomatic tumor,2,5 the patient in the case presented complained of both abdominal and leg symptoms. To the best of our knowledge, this is the first case in the literature of Nora’s lesion causing femoral nerve paresthesia, as well as right lower quadrant abdominal pain. The BPOP tumor was pushing on the psoas muscle, causing nonspecific numbness and tingling in the right anterior thigh.
BPOP does not usually cause significant symptoms. It has a low risk of morbidity and negligible mortality. If there are symptoms at all, they are usually local due to mass effect. 8
The literature describes BPOPs most commonly located in the small bones of the hands and feet. There are a handful of other cases in long bones and on the skull. There have been under 350 cases of BPOP ever reported, let alone only two cases of pelvic origin.2,5,9,10 To the best of our literature research, this is the third ilium (pelvis) originating BPOP ever reported.
Radiologically, early-stage BPOP presents as a small soft tissue mass with inconsistent calcification, which may be partial or complete. The mass seems to arise from the cortex of the underlying bone, generally leaving the cortex intact. In the advanced stages, BPOP manifests as a sessile or pedunculated heterotopic bone formation that exhibits continuity with the adjacent bone cortex.6,8 CT imaging provides enhanced visualization of the features seen on X-rays. MRI is an essential tool in the diagnosis. It generally shows a heterogeneous tumor, with a tendency to have a high signal in T2 and a low signal in T1, distinguishing between the cartilaginous and osseous components of the lesion. 11 Normal cortical appearance and absent marrow signal changes are typical features of BPOP. Typically, there is an absence of cortical breakthrough or extension into the medullary involvement. This lack of medullary continuity into the cavity of the lesion is a distinguishing quality of BPOP, differentiating it from an osteochondroma.12,13 However, it is noteworthy that a few isolated cases have been documented with atypical findings, including cortical destruction and medullary continuity.10,14 In the patient presented, the imaging shows a small medullary continuity at the base of the tumor (see Figures 1A + 1C). The uncommon radiographic characteristics (coupled with the tumor’s location) posed a challenge for radiologists in arriving at a conclusive initial diagnosis. This atypical finding further contributes to the unique nature of this BPOP case.
Histological examination is mandatory as it confirms BPOP diagnosis. Microscopically, the BPOP is characterized by the disorganized entanglement of cartilage, osseous, and fibrous components. The cartilaginous component is arranged either in a cap, like in an osteochondroma, or in lobules. It can, in some cases, be hypercellular3,6,7 and contain chondrocytes with a large nucleus with moderate nuclear atypia and aspects of binucleation. Spindle cells, without atypia, actively proliferate but do not show atypical mitoses. Newly formed bone develops by endochondral ossification from cartilaginous lobules. Furthermore, the bone seen in Nora’s lesion is hypercalcified and is characterized by the purplish-blue mineralization of cartilaginous tissue by the blue dye used during staining(which is absent in parosteal osteosarcoma). This “blue bone” is a defining pathognomonic and specific diagnostic feature of BPOP 15 and is found (as well as with other findings mentioned above) in the case being presented.
Nora’s lesion has a recurrence rate between ~30% and 60%,3–5 within 2 years post excision. In order to reduce these high recurrence rates, when surgery is needed, en bloc resection of the lesion followed by the decortication of the underlying cortical bone is performed. In the case presented, the surgery performed was wide marginal excision of the tumor with careful attention to remove the lesion with clean borders. The pathology report demonstrated tumor-free margins, which was important to reduce the chance of recurrence. The patient is so far still been followed up for over 4 years, consisting of repeated physical exams and imaging, with no indication of recurrence.
Nora’s lesion can be misdiagnosed as other tumors, most commonly as an osteochondroma with malignant transformation, as well as a parosteal osteosarcoma or a periosteal osteosarcoma.2,3,12 It is important to note the differences between BPOP and these other similar appearing tumors as it aids in their respective diagnoses and treatment.
Learning about BPOPs contributes to medical education, enhances clinical practice, supports ongoing research, and ultimately improves patient care. Even though BPOP may be uncommon, the insights gained from studying them contribute to the overall advancement of medical knowledge and practice. This knowledge is essential for medical professionals, including orthopedic surgeons, radiologists, and pathologists, to accurately diagnose and manage patients with such conditions. BPOP can present challenges in diagnosis and management due to its unique characteristics. Being aware of this condition allows healthcare professionals to consider it in the differential diagnosis when evaluating patients with bone tumors, ensuring timely and appropriate treatment. Additionally, knowledge of BPOP helps treating physicians communicate effectively with patients, providing them with accurate information about their condition, prognosis, and treatment options.
The case presented has unveiled a unique instance of a BPOP, manifesting in an exceptionally uncommon location, the pelvic ilium. Furthermore, the patient delineated represents an unprecedented presentation, as it is, to the best of our knowledge, the first reported case of BPOP with these particular symptoms (femoral nerve paresthesia along with concurrent right lower quadrant abdominal pain). This case serves as a distinctive addition to the clinical knowledge base, emphasizing the importance of heightened vigilance toward even the rarest tumors and clinical presentations.
Conclusion
BPOP is a rare tumor with a high recurrence rate. We report a clinical case of this uncommon Nora’s lesion on the ilium, with a unique symptomatic presentation of abdominal pain and femoral paresthesia, as well as atypical radiographic findings. To the best of our knowledge, this is the third case ever to be reported in the literature of Nora’s lesion in this location and the first case ever with this presentation. A joint disciplinary approach was used between orthopedic surgeons and general surgeons to remove the tumor by laparoscopically assisted open marginal excision. The pathology and histology report confirmed the diagnosis of BPOP. The patient’s continued 4-year follow-up has demonstrated no symptoms or evidence of recurrence. This case contributes uniquely to the clinical literature and underscores the significance of increased awareness regarding uncommon tumors and clinical presentations.
Footnotes
Acknowledgements
The authors would like to thank LDK for her help in editing and proofreading the manuscript.
Authors’ note
This is to confirm that the listed authors have authorized the submission of this manuscript and approved any statements or declarations.
Author contributions
The authors declare that the 1st author (A.K.) and the 2nd (J.C.) have equal contributions.
Data availability statement
The data that support the findings of this study are available from the corresponding author, [A.K.], upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from SHAARE ZEDEK MEDICAL CENTER ETHICS/HELSINKI COMMITTEE (0248-23-SZMC).
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.