
Abstract
Bizarre parosteal osteochondromatous proliferation (BPOP), also termed Nora lesion, is a rare, benign tumor most often located in the hands and feet. We herein present the second reported case of BPOP affecting the spine, an uncommon location. One year after surgical excision, the patient was pain-free and showed no evidence of recurrence. We reviewed a total of 323 cases of BPOP among 101 articles, providing the first systematic update on the latest knowledge of BPOP. The age of patients with BPOP ranges from 3 months to 87 years, peaking in the second and third decades of life. The hands are the most common location of BPOP (58.39%), followed by the feet (20.81%). Imaging features play a key role in the diagnosis of BPOP, but histopathologic diagnosis remains the gold standard. Differential diagnosis of BPOP should be based on the epidemiologic and clinical features as well as clinical examination findings. Surgical resection is the most extensively used treatment for BPOP. Recurrence is common (37.44%) and can be treated with re-excision. This article can deepen our understanding of BPOP and will be helpful for the diagnosis and treatment of BPOP in clinical practice.
Keywords
Introduction
In 1983, Nora et al. 1 reported 35 cases of radiologically and histologically distinctive peripheral skeletal osteochondromatous lesions, terming them “bizarre parosteal osteochondromatous proliferation” (BPOP) or “Nora lesion.” BPOP is a rare tumor with no sex predilection, mostly presenting in the third decade of life and primarily affecting the hands and feet. 2 Although BPOP is benign on imaging, it shows locally aggressive characteristics and mixed histopathological features, making it difficult to differentiate from some malignant tumors (such as parosteal osteosarcoma and periosteal chondrosarcoma) and benign lesions (such as periosteal chondroma, osteochondroma, myositis ossificans, subungual exostosis, and florid reactive periostitis). In this report, we present a rare case of BPOP involving in the spine with typical imaging and histological characteristics. We also systematically review the literature on BPOP and compile the most up-to-date knowledge of BPOP, including its epidemiology, clinical features, imaging features, histopathology, differential diagnosis, treatment, and prognosis.
Case report
A woman in her twenties presented to our outpatient clinic with a 4-year history of a back mass and pain. No lower limb pain, numbness, or weakness was reported. She had no history of trauma or infection. On physical examination, a tender, hard, immobile, 20- × 40-mm mass was detected around the right mid-thoracic region. No dermal lesions were present. Muscle force, muscle strength, and neurologic examination findings of all four limbs were normal.
The results of the laboratory work-up, including a routine blood examination, C-reactive protein concentration, erythrocyte sedimentation rate, and electrolyte concentrations, were unremarkable. Radiographs of the thoracic vertebrae showed a heterogeneous density in the vertebral body and vertebral appendix at the Th7–8 level (Figure 1(a), (b)). Computed tomography (CT) revealed a 30- × 17-mm mass with soft tissue density and irregular bone density behind the right vertebral body and vertebral appendix at the Th7–8 level. The bone integrity of the right transverse process and spinous process at the Th7–8 level was compromised. The boundary of the lesion was not well defined (Figure 1(c), (d)). Magnetic resonance imaging (MRI) of the thoracic vertebrae detected an isointense lesion on T2-weighted imaging behind the right vertebral body and vertebral appendix at the Th7–8 level, measuring 19 × 28 × 44 mm (right–left diameter × anteroposterior diameter × vertical diameter). An abnormal signal was observed in the vertebral appendix of Th7, but the signal of the other spinal structures was normal (Figure 1(e), (f)). The radiologists provided a descriptive result based on the CT and MRI findings without rendering a definitive preliminary diagnosis, recommending further pathological examination.

Imaging findings in the present case. (a, b) Preoperative X-ray images of the thoracic vertebrae. (c, d) Preoperative computed tomography images of the thoracic vertebrae. (e, f) Preoperative magnetic resonance images of the thoracic vertebrae and (g, h) one-year follow-up X-ray images of the thoracic vertebrae.
Core biopsy was performed and revealed that the lesion was composed of well-differentiated cartilage tissue, fibrous connective tissue, and mature bone tissue, suggestive of ectopic ossification with chondrometaplasia (Figure 2(a)). Surgical excision was then performed with the patient under general anesthesia. The lesion was accessed through a straight posterior midline skin incision at Th6–8 level. The mass was resected completely, and the spinous process and right outer lamina of T7 were excised. In addition, abnormal cortical bone at Th7–8 level was partially removed by abrasive drilling. A pedicle screw fixation system was applied to enhance the mechanical stability of the thoracic vertebrae, which had been affected by destruction of the facet joints of Th6–8, and bone grafting and fusion of the facet joints was then performed. The excised specimen was sent for histopathological examination. Histopathological analysis revealed a proliferative lesion with well-differentiated cartilage tissue, fibrous connective tissue, and mature bone tissue, the three characteristic components of BPOP. The lesion had partly wrapped around muscle and other soft tissues and eroded the surrounding normal bone. Moreover, the cartilage component exhibited enlarged and bizarre chondrocytes with deep blue mineralization, also called “blue bone,” a characteristic of BPOP lesions (Figure 2(b)). The combination of the medical history, imaging characteristics, and pathology results led to a definitive diagnosis of BPOP. At 1 year of postoperative follow-up, the patient was pain-free and showed no signs of local recurrence (Figure 1(g), (h)).
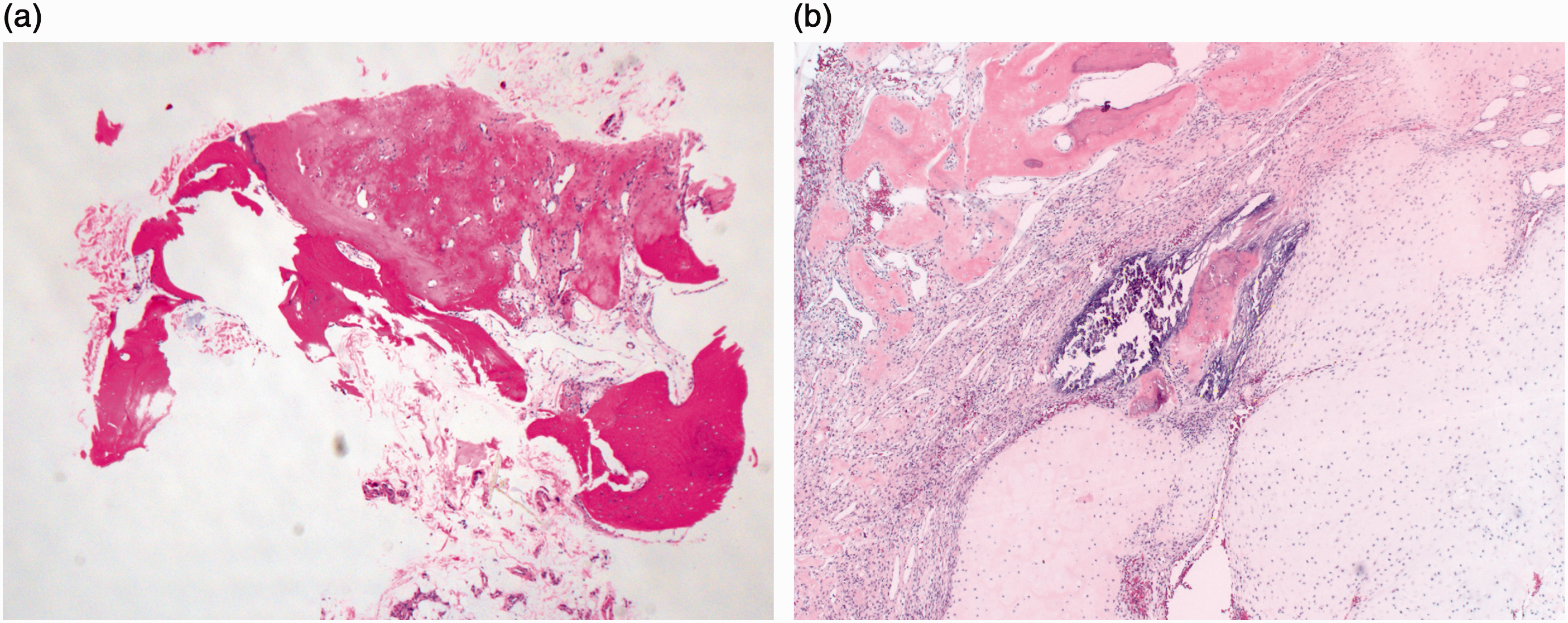
Histopathologic findings in the present case. (a) Hematoxylin–eosin staining of the specimen obtained from the core biopsy. Original magnification 40× and (b) Hematoxylin–eosin staining of the specimen obtained from the excision. Original magnification 40×.
The reporting of this study conforms to the CARE guidelines. 3 Ethics committee approval was not required for this case report. However, board approval was received for publication of the report. The patient provided written informed consent to publish the report, and the patient’s personal details have been de-identified. Prior to the study, the patient had also provided consent for treatment.
Discussion
We used the keywords “bizarre parosteal osteochondromatous proliferation” or “Nora’s lesion” to retrieve articles about BPOP from PubMed. The article retrieval ended on 2 April 2024. Articles were excluded if they were not written in English, did not contain the full text, involved repeated cases, were reviews, involved non-human research, or described laboratory studies. Further evaluation was conducted by carefully reading the full text, and 101 articles were finally included in the analysis (Supplementary Table 1).
Epidemiology and clinical features
To date, 323 cases of BPOP have been reported in 26 countries. The following countries have reported ≥10 cases: the United States (n = 160), the United Kingdom (n = 44), the Netherlands (n = 25), India (n = 17), Australia (n = 11), China (n = 11), and Japan (n = 10) (Figure 3(a)). Clinically, BPOP usually presents as a slowly progressive, firm, painless swelling that can lead to local symptoms secondary to a mass effect, such as tenderness, stiffness, edema, paresthesia, limb weakness, and deformity. 4 Some patients with BPOP have a history of trauma. Most BPOP lesions are <3 cm in size, 4 but some reach 10 cm. 5 The sex was recorded in 318 patients; they comprised 168 (52.83%) male patients and 150 (47.17%) female patients, indicating no sex predilection of BPOP (Figure 3(b)). The patients’ ages ranged from 3 months 6 to 87 years. 7 Based on the available age information, the mean age was 35 years, and most patients were in their second and third decades of life (Figure 3(d)). Notably, our patient was younger than this mean age because many patients in previous reports did not visit the hospital for months or even decades after appearance of the lesion. 8

Epidemiology and prognosis of bizarre parosteal osteochondromatous proliferation. (a) Numbers of lesions reported in different countries globally. (b) Sex-related information of the lesion. (c) Recurrence information of the lesion. (d) Age distribution of patients with the lesion and (e) locations of the lesion.
The specific lesion site was known in 321 cases (Figure 3(e)). One patient had lesions involving two sites (finger and toe), 9 whereas the other patients had lesions involving only one site. In 188 (58.39%) patients, the lesion involved the bones of the hand, including the phalanx of a finger (n = 119), a metacarpal bone (n = 30), and bones without more specific information (n = 39). In 67 (20.81%) patients, the lesion involved the feet, including a metatarsal bone (n = 24), phalanx of a toe (n = 22), sesamoid of a foot (n = 4), talus (n = 2), calcaneus (n = 1), talonavicular joint (n = 1), and bones without more specific information (n = 13). In 51 (15.84%) patients, the lesion involved the long bones of the limbs, including the ulna (n = 15), radius (n = 11), femur (n = 9), tibia (n = 7), fibula (n = 5), and humerus (n = 4). In 8 (2.48%) patients, the lesion involved the head, including the mandible (n = 3), maxilla (n = 2), zygoma (n = 1), parietal bone (n = 1), and nasal dorsum (n = 1). In other cases, the lesion involved the clavicle (n = 2), spine (n = 2, including our case), patella (n = 2), scapula (n = 1) and ilium (n = 1). These results demonstrate that most BPOP lesions are located in the hands and feet; however, the lesion can also affect other uncommon sites, such as the spine as reported in our case. Therefore, we should pay particular attention to the diagnosis of BPOP originating in atypical locations.
Clinical examinations
The results of laboratory examinations were only sporadically reported in these cases of BPOP, suggesting that laboratory workup may not play a significant role in the diagnosis of BPOP. Among the available cases, the routine laboratory examination data showed mostly normal results of the full blood count, serum biochemistry indices, and erythrocyte sedimentation rate, with occasional elevation of the C-reactive protein concentration.10,11
Imaging features play a key role in the diagnosis of BPOP.4,12–14 On plain radiographs, the lesion appears as a well-marginated swelling with varying degrees of heterotopic mineralization, arising from the bone surface and situated adjacent to the underlying cortex. The cortex of the involved bone often remains intact. CT can provide more anatomical detail of BPOP than can radiographs. On CT, typical BPOP lacks continuity with the adjacent cortex and shows no communication with the underlying medullary canal. On MRI, BPOP lesions are hypointense to isointense on T1-weighted imaging and isointense to hyperintense on T2-weighted imaging. As on CT, BPOP lesions on MRI typically show a normal cortex without extension to the marrow. In addition, contrast-enhanced MRI reveals contrast enhancement of the lesions. Apart from plain radiographs, CT, and MRI, some previously reported cases also involved other imaging examinations, such as ultrasound, bone scintigraphy, and single-photon emission computed tomography(SPECT)/CT. However, these examinations provided limited information for the diagnosis of BPOP. Ultrasound examination revealed that the BPOP lesion was hyperechoic, 15 and abnormal uptake in the lesions was detected by bone scintigraphy and SPECT/CT.7,16 Notably, atypical imaging findings were also reported in some BPOP cases, including reactive signal changes in the adjacent tissue, cortical destruction, and corticomedullary continuity with the underlying bone.17,18 Therefore, BPOP cannot be identified by imaging examinations alone.
Histopathologic examination is still the gold standard for diagnosis of BPOP.4,12–14 Macroscopically, the lesion has a nodular surface with a disorganized cartilaginous covering and a blue hue inside the bone. Histologically, the lesion comprises three distinct structures: bone, cartilage, and fibrous tissue. The superficial layer of the lesion is composed of fibrocartilaginous and hyaline cartilage tissue. The intermediate part is composed of cartilage-to-bone transition by endochondral ossification. The innermost layer consists of trabecular bone and intertrabecular spaces containing hypervascular tissue and spindle cells. Whereas minimal cytological atypia is observed in the proliferative spindle fibroblasts and osteoblasts within trabecular bone, the cartilage component exhibits enlarged and bizarre chondrocytes with deep blue mineralization; this is the origination of the term “blue bone,” a characteristic of BPOP lesions.
Differential diagnosis
Differential diagnostic considerations for BPOP include malignant tumors (such as parosteal osteosarcoma and periosteal chondrosarcoma) and benign lesions (such as periosteal chondroma, osteochondroma, myositis ossificans, subungual exostosis, and florid reactive periostitis).4,13
Similar to BPOP, parosteal osteosarcoma most often affects patients in their second to fourth decades of life. Unlike BPOP, however, parosteal osteosarcoma is more common in the metaphysis of long bones; it rarely affects the hands and feet. In terms of imaging features, parosteal osteosarcoma typically appears as a heavily ossified lobular exophytic lesion with a soft tissue component. It is attached to the cortex by a broad-based pedicle and usually shows an incomplete and irregular cartilaginous covering. Parosteal osteosarcoma can also show characteristics of medullary involvement and cortical erosion.19,20 In addition, severe cell atypia, not observed in BPOP, can be seen in parosteal osteosarcoma.
Like BPOP, periosteal chondrosarcoma commonly affects young adults. Unlike BPOP, however, periosteal chondrosarcoma mainly occurs in the femur and humerus, and it usually measures >3 cm. Radiographically, periosteal chondrosarcoma typically presents as a lobular juxtacortical lesion with ring-like or popcorn calcification. 20 In addition, it often exhibits intramedullary extension, cortical erosion, aggressive periosteal reaction, and invasion of surrounding soft tissues. Histologically, periosteal chondrosarcoma shows well-differentiated hyaline cartilage with a lobular structure. Mitosis is not seen in grade I periosteal chondrosarcoma, but increased cellularity and cell necrosis can be observed in grade II. 4
Like BPOP, periosteal chondroma often occurs in young adults and measures <3 cm. Unlike BPOP, however, periosteal chondroma is frequently located in the metaphysis and diaphysis of the femur and humerus. With respect to its radiographic appearance, periosteal chondroma appears as a calcified chondroid matrix with a scalloping and sclerotic edge of the underlying cortex. 21 In addition, periosteal chondroma can exhibit dense periosteal reaction lacks medullary bone. Histologically, periosteal chondroma is composed of lobulated hyaline cartilage, lacks bony trabeculae, and exhibits cellular pleomorphism and atypical mitoses. 22
Osteochondroma usually affects patients in their first three decades of life and arises from the metaphysis of long bones, such as the tibia and femur. Unlike BPOP, however, osteochondroma shows corticomedullary continuity with the underlying bone and has a cartilaginous cap exhibiting uniform alignment of chondrocytes. Moreover, osteochondroma shows a regular arrangement of the trabecular bone, oriented at 90 degrees to the cartilaginous cap and extending parallel to the long axis of the native bone.21–23 In addition, typical osteochondroma contains no fibrous tissue.
Myositis ossificans is a reactive lesion, typically presenting with pain and resulting from injury. This lesion can occur at any age depending on the time of trauma and rarely involves in the hands and feet, making it distinct from BPOP. Myositis ossificans can be easily differentiated from BPOP because it ossifies from the periphery to the center; this is called a zoning phenomenon.19,23 In addition, the lesion is often separated from the adjacent bone, which can lead to periosteal reaction. 22
Subungual exostosis often affects patients during the second or third decades of life, similar to BPOP. 4 Most subungual exostosis occurs adjacent to or beneath the nail bed on the dorsal aspect of the distal phalanx of the big toe. In terms of imaging characteristics, subungual exostosis appears as an osteocartilaginous proliferation, exhibiting no corticomedullary continuity with the underlying bone. Histologically, subungual exostosis consists of mature trabecular bone surrounded by a fibrocartilage cap.
Like BPOP, florid reactive periostitis often affects the phalanges of the hands and feet in the second or third decades of life. However, florid reactive periostitis is frequently associated with injury and is characterized by a periosteal reaction and juxtacortical soft tissue swelling as well as calcification.19,22 Unlike BPOP, florid reactive periostitis histologically lacks cartilage.
Treatment and prognosis
The etiology of BPOP is unknown. It has been reported that recurrent clonal chromosomal abnormalities, including t(1;17)(q32-42;q21-23) and inv(7)(q21.1-22q31.3-32), may be the cause of BPOP.24–26 A recent study further revealed that genetic fusions COL1A1::MIR29B2CHG and COL1A2::LINC-PINT might be involved in BPOP. 27 In addition, an animal experiment indicated that the Jmjd3/p16Ink4a signaling pathway might play an important role in the development of BPOP. 28 Although the above studies suggest some therapeutic targets for BPOP, no specific drug is applied in the clinical setting. Because BPOP is a slowly growing benign lesion, conservative treatment is suggested when patients have no symptoms. One report indicated that the lesion could regress spontaneously. 29 Surgical resection is indicated for patients with symptoms. The most extensively used surgical resection methods for BPOP are excisional biopsy, intralesional excision, marginal excision, wide excision, and amputation. Wide excision is curative in most cases. The lesion has no characteristics of metastasis, but its postoperative recurrence rate is relatively high. It has been reported that the recurrence rate may reach 55% 2 and that patients may develop up to five recurrences. 30 Among all previously reported cases, information on recurrence was provided for 203 patients; 76 (37.44%) of these patients developed recurrence (Figure 3(c)). The primary treatment for recurrence is surgical resection.
In summary, BPOP is a rare lesion that is commonly treated by surgical excision. Diagnosis of BPOP is the basic prerequisite for treatment; however, diagnosis is challenging not only because of the rare occurrence of BPOP, but also because of the existence of atypical BPOP. Although BPOP most frequently involves the hands and feet, there are reports of cases in other unusual locations, such as the spine as described in the present article. In addition, the radiological and histopathological features in some cases of BPOP are atypical. Therefore, careful clinical examination, imaging evaluation, and histopathological analysis should be performed to distinguish BPOP from the above-mentioned differential diagnoses.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241259752 - Supplemental material for Bizarre parosteal osteochondromatous proliferation (Nora lesion) involving the spine: a case report and systematic review
Supplemental material, sj-pdf-1-imr-10.1177_03000605241259752 for Bizarre parosteal osteochondromatous proliferation (Nora lesion) involving the spine: a case report and systematic review by Chao Chen, Bing Wei, Sheng Liu, Zengwu Shao and Sheng Chen in Journal of International Medical Research
Footnotes
Author contributions
SC and CC conceptualized the study and wrote the outline of the manuscript. SL and BW searched the literature. SC, BW, and CC wrote the draft of the manuscript. CC and ZS reviewed and edited the manuscript. All authors have read and approved the final manuscript.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was supported in part by the National Natural Science Foundation of China (Grants 82302767 and 81803917), the Hubei Provincial Natural Science Foundation of China (Grants 2024AFB610 and 2024AFB651), and the Science Foundation of Wuhan Union Hospital (Grant 2022xhyn032).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.