
Abstract
Takayasu arteritis (TAK) is a rare large-vessel vasculitis of unknown etiology that leads to arterial wall thickening, stenosis, and occlusion, which may complicate cerebrovascular ischemic events. Ischemic stroke is a potentially devastating complication of TAK at a young age, but the occurrence is still rarely reported in Ethiopia. Although it occurs late in the course of the condition, it may be the initial presentation and suggest an unfavorable prognosis. Herein, we address the case of a 25-year-old woman who presented to a university hospital while on follow-up after 2 years of stroke with deterioration in clinical symptoms, absent brachial artery pulses, and unrecordable blood pressure in both arms. At the time of admission in 2021, the contrast brain computed tomography scan revealed an ischemic infarction in the right middle cerebral artery territory. However, the etiology of the stroke could not be defined at that time due to ambiguity in the clinical picture and the inability of clinicians to incorporate TAK into the differential diagnosis, resulting in a delay in the early diagnosis of the case. Two years later, in 2023, she underwent computed tomography angiography and was diagnosed to have TAK based on American College of Rheumatology criteria, with Numano type IIb angiographic extent of disease, ischemic stroke, and stage II systemic hypertension. The patient was treated by a field of experts. This case highlights the need to consider TAK in the differential diagnosis of stroke in young patients in the absence of traditional risk factors; appropriate tests should be performed to confirm or rule out this diagnosis, and management should be modified accordingly.
Introduction
Takayasu arteritis (TAK) primarily affects young women in their thirties and causes fibrotic wall thickening, obstructive lesions, and aneurysm formation in large arteries. TAK is an extremely rare cause of stroke, and most cases are due to cerebral hypoperfusion resulting from obstructive lesions in the carotid, vertebral, and subclavian arteries. In patients with TAK, involvement of the aortic arch and its major branches that extend to the carotid and vertebrobasilar circulations can serve as a main cause of large vessel occlusion. 1 It presents as ischemic pain, claudication, carotidynia, the difference in systolic blood pressure (BP) between arms, absence to reduced brachial artery pulse, bruit over the affected arteries, and stroke due to arterial lumen occlusion. 2
In Ethiopia, TAK was first diagnosed, and one case was reported in 1990. 3 There is a dearth of epidemiological data on TAK from Africa, an exception being a large retrospective study conducted by Kaawan et al. 4 in 2020 that documented 388 TAK cases from the African continent: 303 cases were reported from South Africa, 38 cases from Tunisia, and 47 cases from Morocco. 4 In addition, there have been a few cases of these conditions published from Niger, Senegal, and Kenya. 5
TAK has been described worldwide, with an incidence of 0.2–2.6 new cases per million people each year. However, these studies are mainly limited to Asian and Western countries.6–8
Case presentation
Herein, we are reporting the case of a 25-year-old woman who presented to Jimma University Medical Center with a history of sudden onset of left-side weakness and 3-day anepia by 2021. In association with this, she had a history of vomiting, palpitation, and loss of appetite. A month prior to onset, she had intermittent holocranial headaches and fatigue. Otherwise, there was no history of loss of consciousness and abnormal body movement, jaw and/or tongue pain during mastication, myalgia, arthralgia, low back pain, neck discomfort and limitation of joint movement, dizziness, diplopia, and tinnitus. She was free of any medication and had no history of khat chewing or smoking.
Medical evaluation at the time of admission in 2021 her vital signs remained stable: BP:125/85 mmHg; pulse rate: 88 bpm full in volume and palpable on both radial and brachial arteries. Cardiovascular and neurologic examination revealed right carotid bruit and left-side nasolabial flattening; motor examination showed 0/5 throughout the left-side extremities and 5/5 throughout the right-side extremities; and the left-side plantar response was equivocal. Initial blood tests were unremarkable (Table 1). Echocardiography and electrocardiogram were normal. A contrast brain computed tomography (CT) scan showed ischemic infarction (Figure 1). The initial Doppler ultrasound of the neck showed bilateral carotid artery thrombosis; the Doppler ultrasound of the lower and upper extremities was normal. The patient was diagnosed with left hemiparesis secondary to ischemic stroke, supranuclear facial palsy, and bilateral carotid artery stenosis. During her hospital stay, she was given unfractionated heparin 7500 IU subcutaneous twice daily, oral aspirin 81 mg/day, atorvastatin 40 mg/day, and physical therapy. After a week, she was discharged with improvement and linked to chronic outpatient visits for monthly follow-up care.
Laboratory data on admission and follow-up visit, 2021 to 2023.

MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; VDRL: Venereal Disease Research Laboratory; TSH: thyroid stimulating hormone; HDL/LDL: high-/low-density lipoprotein; HIV: human immunodeficiency virus; AST/ALT: aspartate transaminase/alanine transaminase; ALP: alkaline phosphatase; NA: not available.

An axial view of the contrast-enhanced CT scan showed a right middle cerebral artery territory basal ganglia infarction involving the caudate nucleus and cortical region, which is a large, poorly defined hypodensity, as indicated by the arrow.
After about a year of therapy by 2022, the patient showed marked clinical improvement in the form of increased extremity motor strength and wellness, but after a total of 2 years of therapy while on follow-up by 2023, she began to experience easy fatiguability, intermittent holocranial headache, blurring of vision, intermittent syncope, and pain and fatigue of both arms while in use.
Her medical re-evaluation (by 2023) revealed that BP was unrecordable in both brachial arteries; popliteal BP was systolic BP: 165–175 mmHg; diastolic BP: 90–100 mmHg; pulse rate was reduced or faint pulse on both brachial and radial arteries; body mass index was 24.2 kg/m2. Cardiovascular arterial examination revealed 1+ over both radial, brachial, and carotid arteries and 3+++ over the femoral, popliteal, posterior tibial, and dorsalis pedis arteries on both sides. There was no bruit heard over the carotid and subclavian arteries. Neurological motor evaluation indicated a score of 3/5 in the left upper limb, a score of 4/5 in the left lower limb, and 5/5 over the right limbs. Her blood tests were normal except for a raised erythrocyte sedimentation rate (Table 1). Echocardiography and electrocardiogram were normal. Doppler ultrasound of the neck showed circumferential thickening of the carotid arterial wall with luminal narrowing and completely occluded with echogenic intraluminal focus and absent Doppler flow (Figure 2(a) and (b)).

(a) B-mode transverse view of carotid artery Doppler ultrasound showed moderately echoic circumferential arterial wall thickening and completely occluded right carotid artery with echogenic intraluminal focus, demonstrating the “macaroni sign” as indicated by the black arrows. (b) B-mode longitudinal view of right carotid artery Doppler ultrasound showed long, smooth, homogeneous, and relatively echoic circumferential thickening of the arterial wall, indicated by the white arrows, and completely occluded with echogenic intraluminal focus, as indicated by the black arrow.
She underwent CT angiography (CTA) by 2023 and showed enhancing aortic wall thickening and multiple aortic arch branch obstructive diseases (Figure 3(a) and (b)). Based on American College of Rheumatology criteria, TAK with Numano type IIb angiographic extent of disease, ischemic stroke, and stage II systemic hypertension was diagnosed10,11 (Table 2). Treatment decision was made by a field of experts including an internist, neurologist, vascular surgeon, and rheumatologist. She was started on oral prednisone 1 mg/kg/day with tapering to 10 mg/day within 3 months, aspirin 81 mg/day, methotrexate 20 mg/week, folic acid 5 mg/day, amlodipine 10 mg/day, and cotrimoxazole 960 mg three times weekly (discontinued after 3 months). The patient was put on the aforementioned medications with strict follow-up, and her symptoms were under control. On the subsequent visits, her symptoms had improved, and she was functioning well. Until now, the patient has been under our supervision.
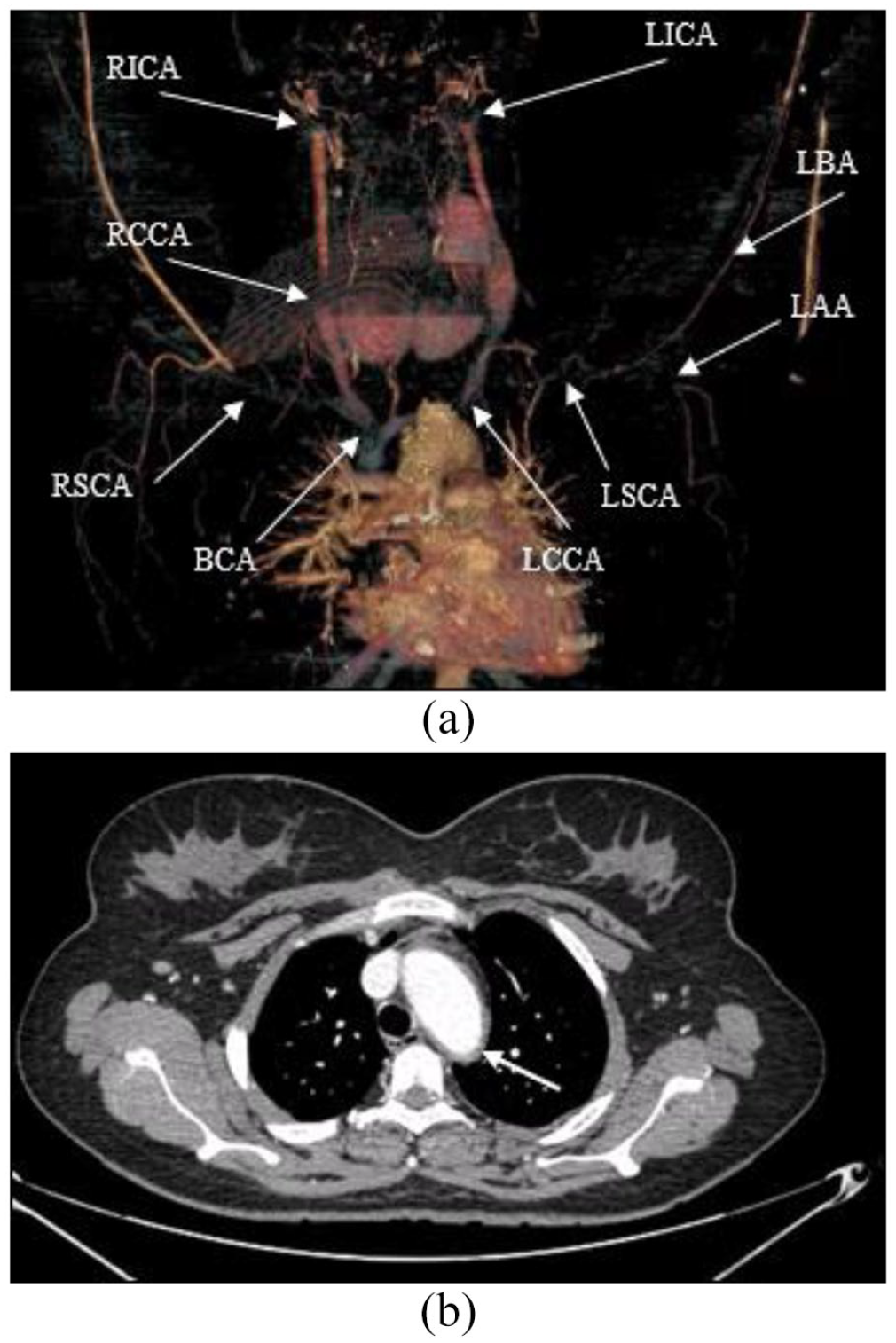
(a) CTA showed (1) long segment occlusion of bilateral CCA. (2) Occlusion of the cervical and intracranial segment of bilateral ICA with thickened enhancing wall. (3) Long segment occlusion with significant smooth luminal stenosis of the LSCA (9.1 cm), proximal and distal RSCA measuring 2.5 cm and 5.6 cm in length, respectively. (4) Left proximal AA long segment occlusion measuring 9.1 cm in length; (5) LBA long segment significant luminal narrowing with thickened and enhancing wall measuring 14.9 cm in length. (6) BCA luminal narrowing with thickened enhancing wall, as indicated by the arrows. (b) An axial view of the CTA showed a typical aortic arch and descending thoracic aorta concentric wall thickening, as indicated by the arrow.
Numano angiographic classification system for Takayasu arteritis.

Discussion
TAK is a systemic, idiopathic, inflammatory vasculopathy that involves the aortic arch and its main branches, often coronary and pulmonary arteries. It primarily affects women at an early age and is often not detected until late since the case is rare, often indolent course, has an unclear early clinical picture, and lacks specific investigative markers.10,12
The etiological factors are unknown. Likewise, the exact mechanism of this condition remains not clearly established. However, infection, auto-immunity, and genetic predisposition are possibly involved in the pathogenesis of TAK. The elastic media of arteries are an immune-privileged site, and studies in mice have shown that it may provide a site for the persistence of pathogens or self-antigens leading to chronic vascular disease.13–15 Furthermore, recent studies indicate an immune-mediated inflammatory condition that results in vessel wall inflammation and fibrosis. This eventually leads to extensive vessel occlusion and stenosis, which is a main risk factor for strokes. 16
TAK has three general phases of causing acute ischemic stroke. An initial inflammatory phase, associated with vague constitutional symptoms and increased inflammatory markers, is frequently overlooked. Left uncontrolled disease progression results in the vessel inflammation phase, which is clinically manifested by reduced or absent pulses, vessel pain, and ischemic events or symptoms and is characterized by arterial wall thickening, stenotic lesions, or aneurysm formation, and later a burnt-out phase, potentially devastating vascular complications such as blindness, stroke, hypertension, aortic regurgitation, and mortality.16,17 More than half of the patients have neurologic involvement, manifesting as lightheadedness, visual problems, and stroke, which can result in serious neurological damage in about 10% of cases.18,19A recent meta-analysis indicated that the prevalence of ischemic stroke among TAK patients is around 15.8%, and it is one of the leading causes of hospitalization and mortality.20,21
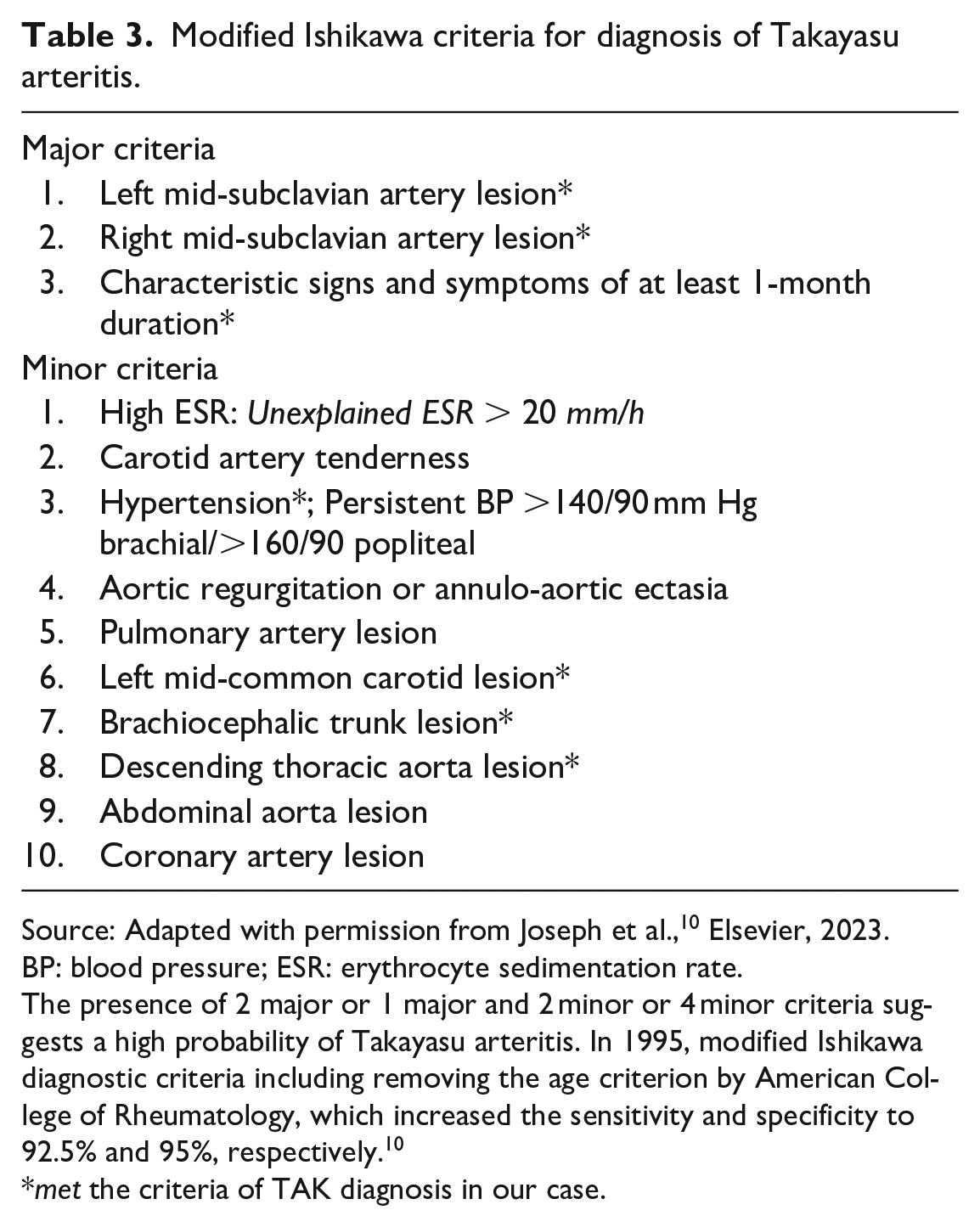
Delay in the diagnosis of TAK is not uncommon. The diagnosis is merely clinical and often delayed due to its rarity, physicians’ inability to consider it in the differential diagnosis, and its conspicuous characteristics of inflammation that overtake relatively more recognized vascular abnormalities. Early diagnosis at the phases of inflammation is a window of opportunity to control the disease progression. The modified Ishikawa criteria for TAK diagnosis have been endorsed as the standard criteria for making a diagnosis. 10 Similarly, in the case presented here, it met three major and five minor modified Ishikawa criteria10,22 (Table 3).
Modified Ishikawa criteria for diagnosis of Takayasu arteritis.
Source: Adapted with permission from Joseph et al., 10 Elsevier, 2023.
BP: blood pressure; ESR: erythrocyte sedimentation rate.
The presence of 2 major or 1 major and 2 minor or 4 minor criteria suggests a high probability of Takayasu arteritis. In 1995, modified Ishikawa diagnostic criteria including removing the age criterion by American College of Rheumatology, which increased the sensitivity and specificity to 92.5% and 95%, respectively. 10
met the criteria of TAK diagnosis in our case.
On the other hand, the diagnosis of TAK is established by the characteristic pattern of magnetic resonance angiography or CTA. Duplex Doppler ultrasonography also aids in the detection of early extracranial lesions of TAK and may provide supportive evidence to CTA about hemodynamics. In the case presented here, it delineates artery wall thickening, which is moderately echoic circumferential, long-segmented, and homogeneous, described as the “macaroni sign,” commonly noted over the common carotid artery. Currently, it is an emerging tool and has greater sensitivity in detecting intima-media thickness as compared to CTA, demonstrating stenotic lesions, and estimating their severity.23,24
Different treatment modalities of TAK have been proposed. Recently, advances in medical therapy have tremendously improved the quality of life and outcomes of patients with TAK. In the past, systemic steroids were the cornerstone of active TAK treatment. However, the current guidelines conditionally recommend a combination therapy of synthetic disease-modifying antirheumatic drugs (DMARDs) and corticosteroids as a first-line therapy to provide both a steroid-sparing benefit and longer-term disease control.25,26 In particular, in the case of a refractory condition, another reasonable approach would be to combine glucocorticoid and biologic DMARDs, which have shown promising outcomes.10,25,27,28 In a recent guideline, antiplatelet therapy is also indicated in patients with active TAK and cerebrovascular ischemic event or vertebrobasilar involvement but is not routinely administered.10,25,27,29
Timely diagnosis and treatment of TAK are important, as effective immunosuppressive therapy prevents the progression of vascular damage. Moreover, in the presence of advanced stenotic lesions, vascular surgery with either endovascular or open approaches is predominantly used.29–31 However, in the case presented here, surgery was challenging, in part due to extensive multiple vessel involvement and complete long-segmented stenotic lesions. Furthermore, the lack of adequate surgical services in our country is also a determinant factor.
The long-term outcome of TAK has varied greatly between studies. Recently, the prognosis for patients with TAK has improved strikingly as a result of advances in treatment. 32 However, advanced cases are associated with considerable morbidity and mortality. Poor neurological outcomes are usually ascribed to late diagnosis and treatment, and nearly half of them are permanently impaired if therapy is delayed.21,33
Conclusion
To the best of our knowledge, ischemic stroke is an unusual initial presentation of TAK, and a delay in early diagnosis frequently occurs. The diagnosis of TAK is confirmed by arteriography. However, it is still a challenge for clinicians to recognize it early due to vague early symptoms, a dearth of specific diagnostic markers, and an indolent course in nature. Recognizing vague symptoms such as headaches and easy fatiguability as an important feature to suspect TAK in a young patient with a previous stroke is crucial. Therefore, this case highlights the need for clinicians to be aware of the varied clinical presentations of TAK so that it is not excluded from diagnostic consideration in appropriate situations, thus avoiding delays in early diagnosis and treatment.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
There is no need for institutional authorization to publish the case details. The patient has consented to the publication of the case report.
Informed consent
The authors received the necessary written informed consent form. The patient offered a written informed agreement to the publication of the case’s details and accompanying images.