
Abstract
Chronic subdural hematoma is a known neurosurgical entity often associated with a spectrum of neurological manifestations. While primarily recognized for its characteristic accumulation of blood between the dura mater and arachnoid membrane, emerging literature suggests a rare association between chronic subdural hematoma and Parkinsonian symptoms. This report aims to underscore this unique neurological relationship by presenting a case of a 70-year-old male who developed Parkinsonism following chronic subdural hematoma post-head trauma. This case underscores the rare association between chronic subdural hematoma and Parkinsonian symptoms, emphasizing the importance of timely diagnosis and intervention in managing such cases.
Keywords
Introduction
Chronic subdural hematoma (CSDH) is a neurological condition characterized by the accumulation of blood between the dura mater and arachnoid membrane, commonly observed in the elderly and often attributed to minor head trauma. 1
CSDH post-traumatic brain injury can result in a range of neurological effects, from mild cognitive issues to severe deficits. The underlying mechanism of CSDH-induced parkinsonism has not been well understood.2,3 A mass effect on the basal ganglia or the midbrain might decrease the number of dopaminergic receptors and the nigro-striatal dopaminergic pathway, respectively, potentially leading to neurological impacts varying from mild cognitive issues to severe deficits. 4 Diagnosis typically involves neuroimaging modalities like computed tomography scan or magnetic resonance imaging, revealing the characteristic hematoma between brain layers. 5
Despite its significance, literature documenting CSDH-related Parkinsonian symptoms remains scarce, especially within Tanzanian medical contexts and broader Sub-Saharan African regions. This lack of comprehensive data impedes a thorough understanding of this rare neurological association in settings like Tanzania, limiting tailored management approaches and highlighting the need for detailed documentation and exploration of such complex manifestations in resource-constrained healthcare settings.
Case presentation
A 70-year-old male patient presented with a 2-month history of gradually worsening dysarthria, gait slowness, and difficulty manipulating utensils, predominantly affecting his left hand. The patient had a pertinent medical history significant for hypertension managed with medications and benign prostatic hyperplasia under medical therapy. Approximately 4 months prior to the presentation, he experienced head trauma resulting from a road traffic crush, although he did not report any loss of consciousness or subsequent neurological deficits.
The onset of the current symptoms was insidious, with no preceding illness or recent medication changes reported. Notably, the patient denied any history of anti-dopaminergic drug usage, exposure to toxins, or unusual environmental factors. No additional significant medical or family history relating to neurological disorders or movement abnormalities was reported. The symptoms gradually progressed in severity, prompting the patient to seek medical attention due to their interference with daily activities.
Upon examination, the patient presented with vital signs within normal limits. His mental state was alert; however, an impaired orientation for time and place was evident. A cranial nerve examination revealed no abnormalities. Evaluation of the motor system demonstrated mild hypomimia and rigidity predominantly on the left side, along with a mild weakness noted in the left arm, accompanied by pronator drift during arm stretching. Reflexes were unremarkable, and there were no signs of pyramidal involvement. Sensory examination revealed normal findings. The Unified Parkinson’s Disease Rating Scale (UPDRS) motor score 6 was 29.
Furthermore, coordination assessment revealed a mild decrease in finger and foot tapping speed on the left side. Gait examination disclosed reduced arm swing on the left but with a normal base and preserved velocity. Notably, there were no signs of tremor or postural instability observed during the assessment.
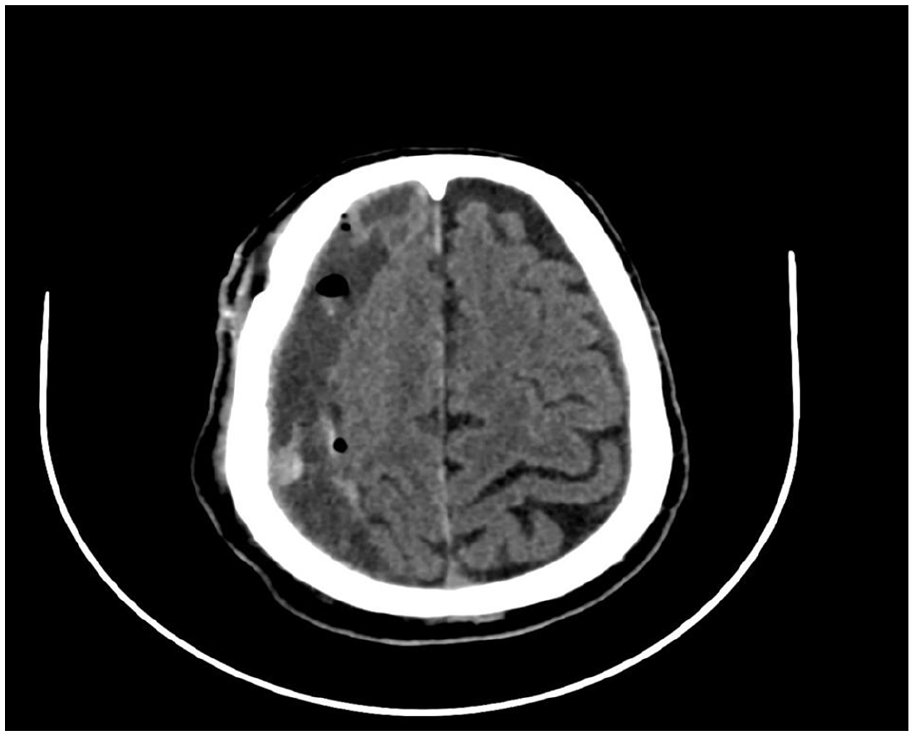
Following the neuroimaging diagnosis showing a CSDH in the right convexity with a slight midline shift to the left (Figure 1), immediate surgical intervention was initiated due to the patient’s clinical condition. Burr hole drainage was performed urgently to evacuate the hematoma and alleviate pressure on the brain.

Features of right subacute to chronic subdural hemorrhage with associated mass effect and subfalcine herniation.
Subsequent imaging, notably computed tomography (CT) scan findings post-surgery, indicated resolution of the hematoma and exhibited normal results (Figure 2), signifying successful evacuation and alleviation of the initial symptoms.
Right subdural hematoma has decreased in size and thickness, the largest measuring 15 mm in thickness at the posterior parietal region. No acute bleeding is visualized. There are multiple hyperdense septations noted with the subdural collection.
After the surgical intervention, he was not prescribed anti-dopaminergic drugs as his symptoms gradually improved and completely subsided after 4 weeks. The UPDRS motor score 6 improved to 10. The dysarthria, gait slowness, and difficulties using utensils, predominantly with his left hand, which had been progressively worsening over the preceding 2 months, notably subsided. The patient’s neurological deficits, including rigidity, bradykinesia, and other motor abnormalities, showed substantial improvement, nearly resolving. He was scheduled for clinic visits every 2 weeks. After 2 months, the patient’s symptoms completely resolved.
Discussion
CSDH is increasingly recognized as a rare yet significant cause of Parkinsonism, particularly among elderly individuals following minor trauma. 1 The association between CSDH and Parkinsonism has been documented in several case reports and studies, shedding light on the clinical characteristics, diagnostic challenges, underlying mechanisms, and treatment outcomes of this intriguing phenomenon. 7
Our presented case closely aligns with previous reports linking CSDH to Parkinsonism, emphasizing the importance of considering this etiology in elderly patients presenting with new-onset or rapidly progressive Parkinsonian symptoms following minor head trauma. 8 The clinical features observed in our 70-year-old male patient, including left-sided rigidity and bradykinesia, mirror those reported in other cases of CSDH-induced Parkinsonism, suggesting a consistent pattern of presentation across different instances.
Wiest et al. 2 and Sugie et al. 3 have reported similar cases of Parkinsonism secondary to CSDH, highlighting the challenge of diagnosing CSDH based solely on clinical features due to their nonspecific nature. These studies underscore the pivotal role of neuroimaging, particularly CT scans, in accurately identifying CSDH and guiding appropriate management strategies. Our case reinforces this notion, as prompt recognition and surgical intervention led to favorable outcomes, emphasizing the importance of early diagnosis and intervention in improving patient outcomes.
Moreover, the mechanisms underlying CSDH-induced Parkinsonism remain complex and multifaceted. Studies by Giray et al. 4 and Hsieh et al. 7 propose various mechanisms, including direct mechanical compression of basal ganglia structures, midbrain distortion due to herniation, and circulatory disturbances affecting dopaminergic pathways. These mechanisms are consistent with our observations and support the causal relationship between CSDH and Parkinsonian symptoms.
Interestingly, our case also shares similarities with previous reports regarding the reversibility of Parkinsonism following surgical evacuation of CSDH. Sandyk and Kahn 8 reported a case of Parkinsonism due to subdural hematoma, where surgical treatment led to the complete resolution of symptoms. This observation underscores the potential reversibility of Parkinsonian symptoms associated with CSDH, further highlighting the importance of timely surgical intervention in mitigating neurological deficits.
Furthermore, the utilization of drug therapies, as suggested by Chou et al. 9 and Suman et al., 10 has shown effectiveness in managing Parkinsonian symptoms pre-surgery, further emphasizing the importance of multidisciplinary approaches in addressing CSDH-induced Parkinsonism.
In summary, our presented case adds to the growing body of literature on CSDH-induced Parkinsonism, highlighting the clinical manifestations, diagnostic challenges, underlying mechanisms, and treatment outcomes associated with this rare neurological association. Comparative analysis with previous reports underscores the consistency of clinical presentations, the importance of neuroimaging in diagnosis, and the potential reversibility of Parkinsonian symptoms following surgical intervention. Continued research and collaboration are essential in further elucidating the pathophysiology and optimal management strategies for CSDH-induced parkinsonism, ultimately improving patient care and outcomes.
Conclusion
This case contributes to understanding the link between CSDH and Parkinsonism. Prompt recognition and neuroimaging evaluation in patients presenting with recent head trauma and new-onset motor symptoms are crucial. Timely surgical intervention can potentially reverse Parkinsonian symptoms associated with CSDH, offering promising outcomes in alleviating neurological deficits.
Footnotes
Acknowledgements
None.
Author contributions
W.K.: Study conception, production of initial manuscript, collection of data; F.S.: Production of initial manuscript, revision of the manuscript, proofreading; C.M.: Revision of the manuscript, proofreading, and performed surgical procedure; P.A.: Production of initial manuscript, revision of the manuscript, and proofreading.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article.
The patient was able to provide consent as he was fully conscious and had the decisional capacity to do so.