
Abstract
This case report presents the clinical journey of a 28-year-old nulliparous woman from Dar es Salaam, Tanzania, who sought medical attention due to lifelong urinary leakage since birth, profoundly impacting her emotional well-being and sexual encounters. Clinical examination revealed urinary leakage from the vagina, with unremarkable abdominal and genital findings. Laboratory investigations were normal. Computed tomography intravenous urography revealed a left duplex collecting system with significant hydroureteronephrosis in the left upper moiety, suggestive of an ectopic ureter. Intraoperative exploration confirmed a duplicated left ureter, with the upper moiety implanted into the vaginal canal. Surgical re-implantation of both left ureters into the bladder was successfully performed, correcting the anatomical anomaly. Postoperative follow-up demonstrated marked improvement in urinary symptoms, restoring the patient’s confidence and alleviating emotional distress. This case underscores the complexity and rarity of congenital urinary tract anomalies, particularly in resource-constrained settings, and highlights the importance of a stepwise diagnostic and management approach.
Introduction
Congenital anomalies of the urinary tract encompass a broad spectrum of conditions ranging from common functional disturbances to rare organic abnormalities, collectively referred to as congenital anomalies of the kidney and urinary tract (CAKUT). 1 The incidence of CAKUT is approximately 1 in 500 live births, with duplicated ureters occurring in 0.5%–2% of the population. Among these, ureterovaginal fistula (UVF) and duplicated ureters are particularly noteworthy due to their potential to significantly impact patients’ quality of life and necessitate specialized management. 2 The incidence and occurrence of these conditions vary between developed and underdeveloped regions, largely due to differences in healthcare infrastructure, prenatal care, and diagnostic capabilities.1,3 In developed countries, advanced prenatal screening allows for early detection and management of CAKUT, leading to more accurate incidence reporting. 3 Conversely, in underdeveloped regions, limited access to healthcare and diagnostic facilities often results in underreporting and delayed diagnosis, with conditions like UVF going undetected until they present clinically, often with severe complications.
UVF is characterized by an abnormal connection between the ureter and the vagina, which often leads to urinary leakage and recurrent infections, posing considerable challenges in both diagnosis and treatment. 3 Similarly, duplicated ureters, a condition where the ureteral bud undergoes bifurcation resulting in two ureters draining a single kidney, introduce complexities in the anatomy and function of the urinary tract. 2
Functional disturbances causing urinary incontinence in childhood are relatively common and may result in unsatisfactory treatment outcomes. However, organic causes such as ectopic ureter (EU) offer the potential for cure through surgical correction. 4 EU is a condition where the ureter does not insert into the bladder but into different parts of the genitourinary system, such as the urethra, ejaculatory tract, vas deferens, seminal vesicles, vagina, or uterus, affects 1 in 2000 individuals and often necessitates surgical correction for symptomatic relief. 5 This underscores the importance of precise diagnosis and tailored management strategies.
According to Weigert–Meyer’s rule, in cases of ureteral duplication, the upper pole ureter tends to insert ectopically, often associated with obstruction, whereas the lower pole ureter typically inserts normally but can be prone to reflux. 6 This rule is critical for understanding the presentation and potential complications associated with duplicated ureters. 7
Imaging studies, including ultrasound, magnetic resonance imaging (MRI), and computed tomography (CT), play a crucial role in diagnosing EU and delineating associated anomalies. 3 Surgical intervention, guided by factors such as renal function and the location of the EU, aims to restore urinary continence and preserve renal function. 8
In this context, we present a rare case of UVF with a duplicated left EU in a Tanzanian patient, highlighting the challenges and successful management of this complex congenital anomaly. Through meticulous diagnostic evaluation and tailored surgical intervention, we aim to emphasize the importance of early recognition and comprehensive care in addressing rare urinary tract anomalies.
Case presentation
A 28-year-old nulliparous woman from Tanzania presented to our clinic with a chief complaint of lifelong urinary leakage, which had significantly impacted her emotional well-being and intimate relationships. She reported experiencing urinary leakage since birth, with no significant episodes of recurrent urinary tract infections or loin pain. The embarrassment associated with her condition had led her to avoid sexual encounters, further exacerbating her distress.
Despite her condition, she had not sought medical help earlier due to a series of misdiagnoses and ineffective treatments. She had visited various health centers where she was diagnosed with urinary tract infections and given antibiotics, which did not improve her symptoms. Over time, she learned to live with the condition, believing it was a part of how she was born.
Two months ago, an trained urogynecologist ambassador of fistula visited her village, raising awareness about the obstetric fistula. This encounter prompted her to seek care at Comprehensive Community Based Rehabilitation Tanzania (CCBRT) Hospital, hoping for a more accurate diagnosis and effective treatment. Her journey highlights the challenges faced by individuals with congenital anomalies in accessing appropriate healthcare, often due to misdiagnoses and lack of awareness.
Diagnostic evaluation
Upon physical examination, the abdomen was soft, non-tender, and without any palpable masses or organomegaly, indicating no overt abdominal pathology. On vaginal examination, a bimanual pelvic exam revealed a normal-sized, anteverted uterus, with no adnexal masses or tenderness. Continuous urine leakage from the vagina was observed, strongly suggesting a UVF. Despite the absence of visible genital abnormalities such as fistulous openings, scarring, or masses, the persistent urinary leakage raised significant suspicion of underlying urinary tract anomalies. A sterile speculum examination confirmed that the urine appeared to be coming from the lateral vaginal wall, further supporting the suspicion of UVF. Although a range of functional imaging techniques, such as retrograde pyelogram and cystoscopy, would have provided additional insights, these modalities were not available at our center. Consequently, computed tomography intravenous urography (CT IVU) was the only imaging study performed. CT IVU was chosen for its ability to provide a detailed evaluation of the urinary tract, allowing for the confirmation of the diagnosis, the precise location of the fistula, and the assessment of any associated anomalies.
Laboratory investigations, including complete blood count, renal function tests, and urinalysis, returned within normal limits. However, given the clinical suspicion of a congenital urinary tract anomaly, further imaging studies were warranted.
Imaging studies
CT IVU was performed, revealing a left duplex collecting system with significant hydroureteronephrosis of the left upper moiety, suggestive of an EU. This finding confirmed the presence of a duplicated left ureter, with the upper moiety ectopically implanted into the vaginal canal. Renal maldevelopment, commonly associated with EU, was evident, further complicating the clinical picture.
Kidney function and vesicoureteral reflux
The left kidney’s upper pole was significantly affected by hydroureteronephrosis, indicating compromised function due to the EU. The lower pole ureter, although appearing normal in size on imaging, was not draining into the urinary bladder. Scintigraphy to assess kidney function was not done due to unavailability in the country.
Figure 1 shows the CT IVU, demonstrating the presence of a left hydroureter. In contrast, Figure 2 illustrates the CT axial IVU, displaying the left duplex collecting system (double ureter), with the left moiety ureter implanted into the vagina.
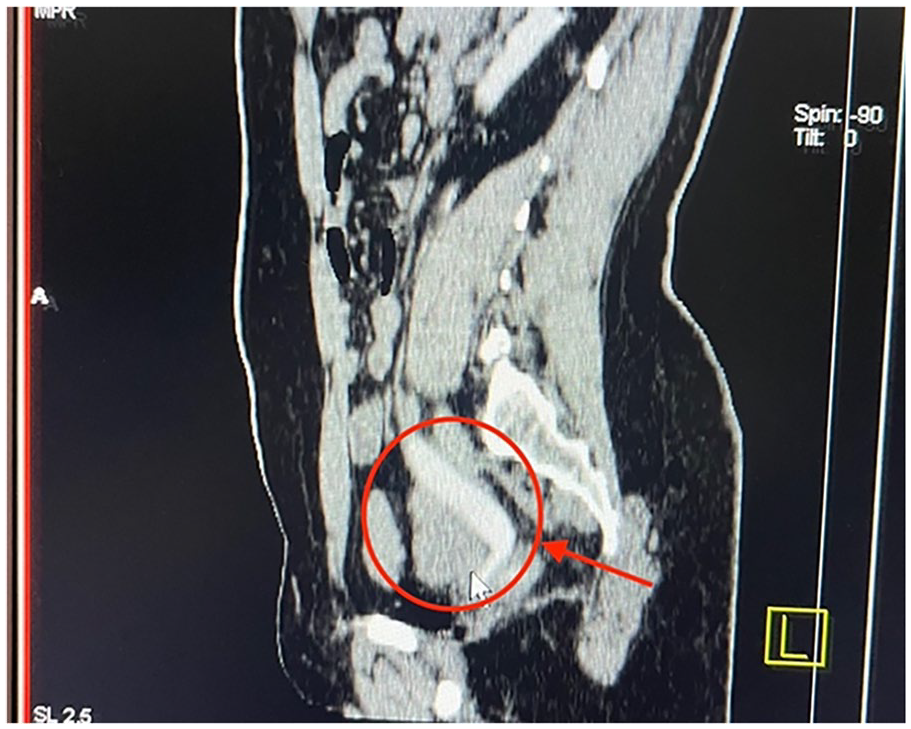
Above shows the CT IVU, demonstrating the presence of a left hydroureter.

Above illustrates the CT axial IVU, displaying the left duplex collecting system (double ureter), with the left moiety ureter implanted into the vagina.
The image presented as Figure 3 above depicts the CT IVU, providing visual evidence of the hydronephrosis affecting the left upper moiety (ectopic) ureter.

Above illustrate the CT IVU, providing visual evidence of the hydronephrosis affecting the left upper moiety (ectopic) ureter.
Intraoperative exploration under spinal anesthesia revealed the presence of a duplicated left ureter, with the upper moiety dilated and ectopically implanted into the vaginal wall. Surgical intervention was undertaken to address the anomaly, aiming to restore urinary continence and preserve renal function.
Findings: The examination revealed a left duplex collecting system (double ureter), with the left upper moiety ureter dilated (hydroureter) and draining into the vagina, as depicted in Figure 4. In contrast, Figure 5 shows the left lower ureter appearing normal in size; however, there is no evidence of drainage into the urinary bladder. Therefore, re-implantation of both ureters was performed.

The above examination revealed a left duplex collecting system (double ureter), with the left upper moiety ureter dilated (hydroureter) and draining into the vagina.

Shows the left lower ureter appearing normal in size; however, there is no evidence of drainage into the urinary bladder.
The surgical approach involved re-implantation of both left ureters into the bladder, meticulously ensuring proper positioning to facilitate adequate drainage and restoration of urinary tract function. The procedure was conducted without complications, and to aid in postoperative monitoring and drainage, ureteric catheters were inserted.
In Figure 6, you can see the placement of catheters in both ureters.
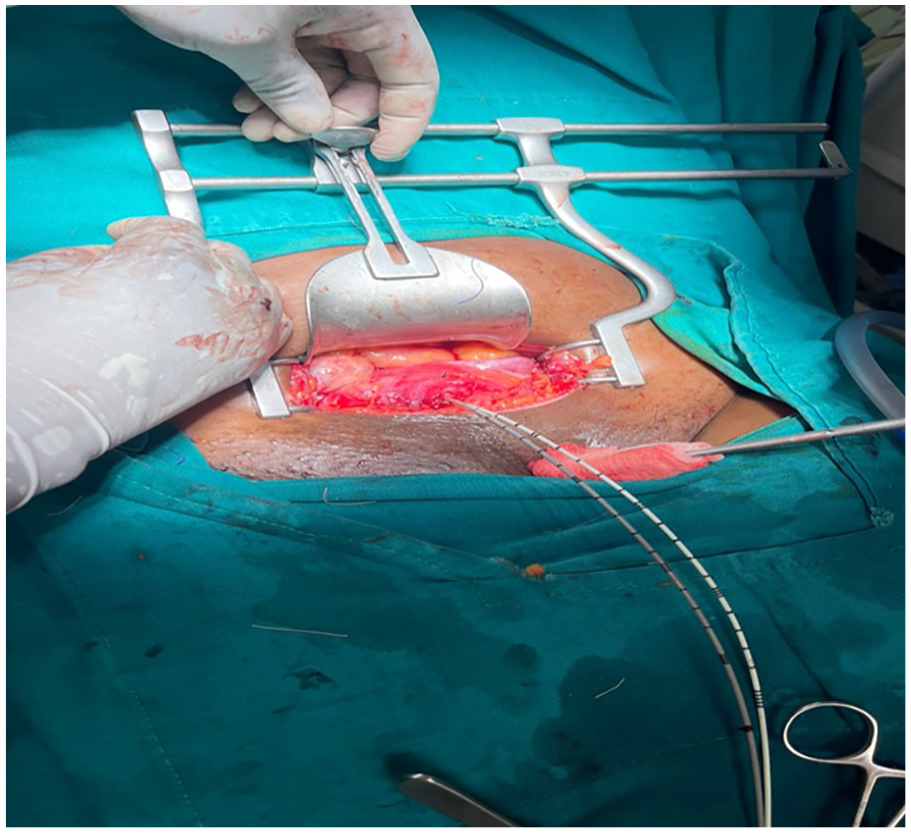
Above illustrate the placement of catheters in both ureters.
Postoperative evolution
In the immediate postoperative period, the patient received a tailored regimen of medications aimed at promoting healing and preventing complications. Intravenous (IV) Ceftriaxone 1 g was administered every 12 h for 2 days, along with IV Metronidazole 500 mg every 8 h for 2 days, to prevent potential infections and ensure the integrity of the surgical site. Additionally, IV Paracetamol 1 g was given every 8 h for 2 days to manage postoperative pain effectively, promoting comfort and facilitating early mobilization.
The ureteric catheter was removed after 10 days to facilitate the patient’s recovery process. Subsequently, the urinary bladder catheter was removed after 14 days, indicating successful healing and restoration of normal urinary function. These steps in postoperative care were essential in ensuring optimal recovery and minimizing the risk of complications.
Following the initial postoperative period, the patient underwent follow-up appointments to monitor her progress and assess the long-term outcomes of the surgical intervention. Two weeks after the procedure, the patient reported a significant improvement in her symptoms, with the urinary leakage resolved entirely. This positive development marked a crucial milestone in her recovery journey.
During follow-up visits, it was noted that the patient’s self-esteem began to improve progressively. The resolution of urinary leakage not only alleviated physical discomfort but also had a profound impact on her emotional well-being and self-perception.
Discussion
Maintaining a high index of clinical suspicion is crucial in young female patients presenting with recurrent urinary symptoms, such as urinary incontinence. These symptoms may be indicative of underlying congenital anomalies of the urinary tract, such as UVF and EUs. A thorough and systematic diagnostic approach is essential to accurately identify these anomalies and guide appropriate management.3,7
The diagnostic evaluation should begin with a detailed patient history and physical examination, focusing on identifying signs of urinary tract anomalies. In patients with suspected genitourinary anomalies, imaging studies are pivotal. Ultrasound is often the initial imaging modality used due to its non-invasive nature and ability to identify gross anatomical abnormalities. 8 However, for detailed anatomical delineation and to confirm suspicions, advanced imaging techniques are necessary.
CT IVU is highly effective in visualizing the anatomy of the urinary tract, detecting duplicated ureters, and identifying ectopic ureteral insertion sites. 9 MRI can also be used for detailed anatomical imaging, especially in complex cases. Additionally, voiding cystourethrography can help detect vesicoureteral reflux and assess bladder function.10,11
Assessing kidney function is critical in patients with congenital urinary tract anomalies. Scintigraphy, such as a dimercaptosuccinic acid scan, provides a functional assessment of each renal moiety, helping to determine the differential function of the upper and lower renal poles. 11 This information is vital in guiding surgical decision-making and planning.
Surgical intervention for UVF and EUs aims to restore urinary continence and preserve renal function. The choice of surgical technique depends on the patient’s specific anatomy and kidney function. 12 Common surgical options include ureteral re-implantation, where the EU is repositioned into the bladder. 6 In cases where the renal moiety associated with the EU is non-functional, heminephrectomy may be considered.
For patients with duplicated ureters, the surgical approach may involve ureteroureterostomy, where the upper pole ureter is connected to the lower pole ureter, or ureteral re-implantation of both ureters into the bladder.6,9 The surgical plan should be tailored to the individual patient’s anatomy and functional capacity of the renal units.
In recent years, minimally invasive techniques have gained popularity in the management of congenital urinary tract anomalies. Laparoscopic and robotic-assisted surgeries offer the advantages of reduced postoperative pain, shorter hospital stays, and faster recovery times compared to open surgery. Laparoscopic ureteral re-implantation and laparoscopic clipping of non-functional upper pole ureters are emerging as effective treatment modalities. 9 These techniques require careful consideration of the patient’s kidney function and the anatomical complexity of the anomaly.
Laparoscopic clipping involves occluding the EU, preventing urine flow into the ectopic site, which can be a suitable option for patients with non-functional upper pole moieties. This approach minimizes surgical morbidity while addressing the patient’s symptoms effectively. Robotic-assisted ureteral re-implantation offers enhanced precision and control, making it a valuable option for complex reconstructive surgeries.7,9
Conclusion
A high index of clinical suspicion and a comprehensive diagnostic approach are essential in managing young female patients with recurrent urinary symptoms suggestive of congenital urinary tract anomalies. Advanced imaging and functional assessments are crucial in diagnosing and planning the appropriate surgical intervention. Tailored surgical treatments, including new minimally invasive techniques, offer promising outcomes for patients with UVF and EUs, emphasizing the importance of individualized care based on the patient’s anatomy and kidney function.
Footnotes
Acknowledgements
We extend our sincere gratitude to the Senior Gynecologists at CCBRT, the Radiologist, and the Medical Officers, all of whom dedicated their expertise and efforts to the care of this patient. Their collaboration and diligent work were instrumental in achieving successful outcomes. Additionally, we express our heartfelt appreciation to our patient for graciously allowing us to learn from her clinical presentation.
Authorship contributions
Brenda Moshi: Study conception, production of initial manuscript, collection of data. Daudi Gidion: Production of initial manuscript, revision of the manuscript, proofreading. Muzdalifat Abeid: Revision of the manuscript, proofreading. Munawar Kaguta: Production of initial manuscript, collection of data. James Chapa: Revision of the manuscript, proofreading. Peter Majinge: Study conception, revision of the manuscript, proofreading.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.