
Abstract
Chronic subdural hematoma is a common condition in neurosurgical practice. It is usually treated by burr-hole surgery. Patients with coagulopathies such as antiphospholipid syndrome, are at increased risk of complications, and careful consideration of the patient’s specific risk of both bleeding and thromboembolic complications must guide medical management. We present the case of a 34-year-old who presented to the neurosurgical department with a chronic subdural hematoma. She had a medical history of triple-positive antiphospholipid syndrome, lupus, and mechanical aortic valve replacement due to Libman-Sacks endocarditis. It was considered of high risk to proceed with traditional burr-hole surgery, so instead embolization of the middle meningeal artery was performed. Postoperatively the patient gradually improved, and a scan at 6 months showed complete regression of the hematoma. She later presented with a contralateral subdural hematoma, which was also successfully treated with middle meningeal artery embolization. Unfortunately, she suffered from an intracerebral hemorrhage shortly afterward, which was treated conservatively by careful management of her anticoagulant therapy. She has now made a full recovery at 4 months follow-up.
Keywords
Introduction
Chronic subdural hematoma (cSDH) is a condition characterized by the accumulation of fluid, blood, and blood degradation products in the subdural space, usually seen 4–7 weeks after head trauma. 1 It is a common condition in neurosurgical practice with increasing prevalence in the elderly. The disease is rare in patients under the age of 50. 2 Traditionally cSDH has been treated with burr-hole irrigation and drainage, but in recent years middle meningeal artery (MMA) embolization has gained attention as an alternative treatment. 3
Antiphospholipid syndrome (APS) is an autoimmune disease associated with an increased rate of thromboembolic events. It is often associated with other autoimmune diseases, most commonly systemic lupus erythematosus (SLE). 4 The triple-positive profile, defined by the presence of lupus anticoagulant, anticardiolipin antibodies, and anti-β2 glycoprotein-I antibodies, is associated with a further increased risk of thrombosis. 4 A retrospective cohort study found a prevalence of neurological manifestation of thromboembolic events of 46.4% in patients with both SLE and APS. 5 Treatment of APS usually involves a combination of anticoagulant and antiplatelet agents. 6
There are no current international guidelines for patients with APS undergoing surgery. The management of pre- and postoperative antithrombotic therapy should consider both the patient-specific risk of thromboembolic events and weigh it against the peri- and postprocedural risk of bleeding complications.7,8 In the specific case of APS patients undergoing neurosurgery, it is advisable to bridge with heparin and to aim for a preoperative international normalized ratio (INR) below 1.5. 8
We present a case of a young woman, with triple-positive APS, who suffered a minor head injury resulting in a cSDH, which was successfully treated by MMA embolization.
Case
Presenting complaints
A 34-year-old female was admitted to the hospital with a 2-week history of headache and dizziness. Three weeks prior, she had sustained a minor head injury. The patient was seen in the emergency department, where a computed tomography (CT) scan was performed revealing a right-sided cSDH (Figure 1).

CT scan at hospitalization showing a right-sided cSDH.
Medical history
She had a past medical history of SLE, triple-positive APS, and a mechanical aortic valve due to previous Libman-Sacks endocarditis. She also had a history of mechanical valve thrombosis, requiring thrombolysis. Her current anticoagulant regimen was phenprocoumon (a vitamin K antagonist), with a target therapeutic INR interval between 3.0 and 3.5. Her antiplatelet therapy was 75 mg of acetylic salicylic acid (ASA) daily.
Initial management
On arrival at the neurosurgical department, she had a Glasgow Coma Scale of 15 and had no focal neurological deficits. Her primary symptoms were severe headache and dizziness. Initial medical management included discontinuation of the vitamin K antagonist and ASA treatment, and she was bridged with heparin due to her history of APS and mechanical valve thrombosis. Her initial INR was 4.4, and the plan was to wait for it to drop below 1.5 before proceeding with surgery.
The risk of evacuating the hematoma by burr-hole was considered high. We draw this conclusion both because of the increased risk of postoperative acute subdural hematoma (SDH), and because of the increased risk of recurrence, as anticoagulant treatment would have to be resumed shortly after surgery. A prolonged period without anticoagulation would be associated with a high risk of thromboembolic events.
Three days after admission, a control CT scan showed additional acute components in the chronic hematoma, despite the expected increase in her clotting ability from the discontinuation of her usual anticoagulant regimen. It was therefore decided to proceed with endovascular embolization of the right-sided MMA.
Intraoperative details
In general anesthesia, under ultrasound guidance, a 6 French sheath was inserted in the right femoral artery and exchanged for a BALLAST 80 cm sheath. Selective catheterization and angiography of the right internal and external carotid artery (ECA) were performed through an HH1 5-French diagnostic catheter. Following this, a 5-French Sofia guide catheter was placed in the right ECA, with angiography here showing a large subdural filling defect due to pressure from the SDH. Superselective right-sided MMA catheterization was performed with microcatheter (MC) and Microwire, and a possible meningo-orbital variant was identified. A selective embolization was performed in both the frontal and parietal branches with Squid 12 0.8 ml, thereby ensuring a position distal to the ophthalmic artery supply (Figure 2). Both MCs were evacuated without technical complications.
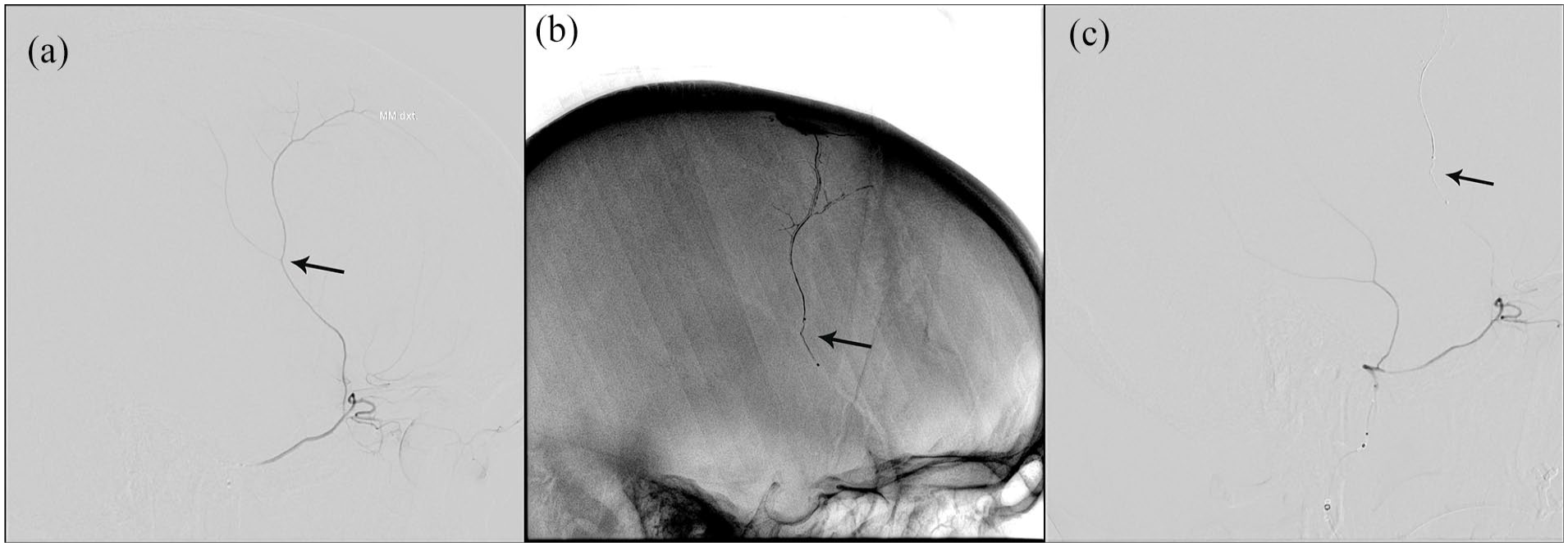
(a) Lateral angiography showing the right-sided anterior branch of the MMA. (b) Lateral radiograph showing the penetration of the embolisate. (c) Lateral angiography showing no flow in the anterior branch of the MMA after the evacuation of the embolisate. The black arrows mark the same branching point of the artery in all three images.
Angiography at the end of the procedure showed complete occlusion of the right MMA and unhindered flow in the ophthalmic artery.
Postoperative course
A new CT scan was performed 4 days after embolization and showed a slight regression of the hematoma. Further scans at 11 and 25 days showed further reduction in the hematoma size. The patient was discharged from the hospital 25 days after the embolization procedure. At the 2-month follow-up, a new CT scan was performed and showed further regression of the hematoma. At this time, the patient experienced an improvement in her symptoms in the form of a reduction in her headaches and a subjective increase in her ability to concentrate. A CT scan at the 6-month follow-up showed complete resolution of the hematoma (Figure 3).
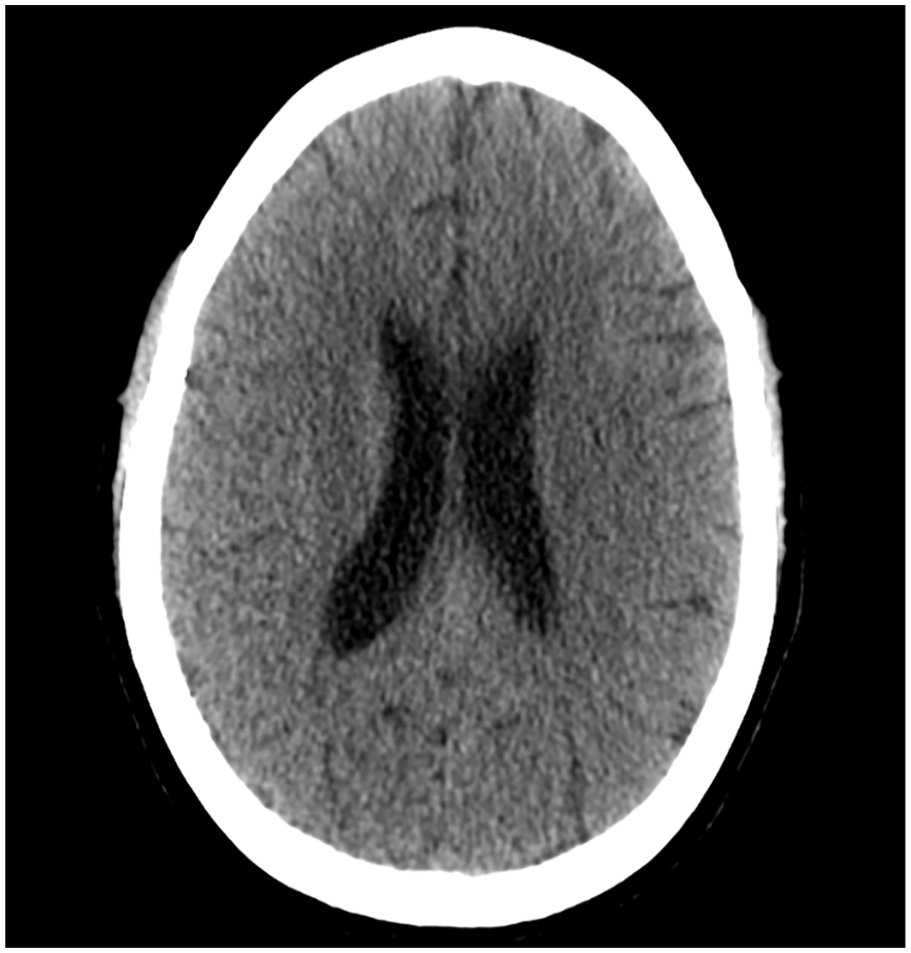
CT scan after 6 months showing complete resolution of the hematoma.
Unfortunately, 2 months following the 6-month follow-up scan, the patient was readmitted to the hospital. Her symptoms at this time were right-sided weakness and mild aphasia. She was initially admitted with a suspicion of stroke and as such an MRI was performed, which showed a left-sided cSDH (Figure 4). There was no residual hematoma on the right side. Given the good results of the first embolization, it was decided to proceed with embolization on the left side. Her vitamin K antagonist and ASA treatment were stopped, and she was again bridged with heparin.

T2 weighted MRI shoving a left-sided cSDH.
The procedure was performed 3 days later, and her anticoagulant regimen was restarted. 3 days after the procedure, she continued to have mild aphasia, and a new CT scan was performed showing a slight regression of the hematoma. She was discharged 6 days after the procedure.
She was scheduled for a 1-month follow-up scan, but after 2 weeks she experienced increasing headaches, nausea, sensitivity to light, and pain behind her left eye. She was admitted to the hospital, and another CT scan was performed. Unfortunately, this scan showed a left-sided intracerebral hemorrhage (ICH) at the temporal pole and associated edema. Her anticoagulants were discontinued, and she was given 5 mg of vitamin K. An MRI was performed the next day, and showed no evidence that this hemorrhage was the result of a hemorrhagic transformation of an infarct. Another scan was performed the next morning, but this scan showed further progression of the size of the ICH (Figure 5).

CT scan showing a left anterior temporal lobe ICH.
In collaboration with the cardiology department, it was decided to aggressively reverse her anticoagulation, aiming for an INR of 1–1.2. However, this would put her at high risk of clot formation on the mechanical valve. Her INR was lowered with a combination of additional vitamin K, prothrombin complex concentrate, and fresh frozen plasma. After 2 days, her INR was at the appropriate level. Another CT scan 5 days after admission showed that the bleeding had stopped, and she was improving clinically. She was then restarted on heparin. An echocardiogram at this time fortunately showed no evidence of clot formation on the mechanical valve.
Follow-up
She was discharged from the hospital 10 days after admission, at this time with short-term memory deficits, and mild aphasia. She was scheduled for a follow-up scan 1 month later. This scan showed slight regression of the ICH and regression of the edema. The patient had experienced gradual improvement with a decrease in her headaches. However, she still had some difficulty with concentration and memory.
A final follow-up was performed 4 months after discharge. At this time, the patient had returned to school and experienced only a slight decrease in her concentration and memory. A final CT scan showed complete resolution of cSDH bilaterally, and that the ICH had resolved, leaving behind a hypodense area (Figure 6).
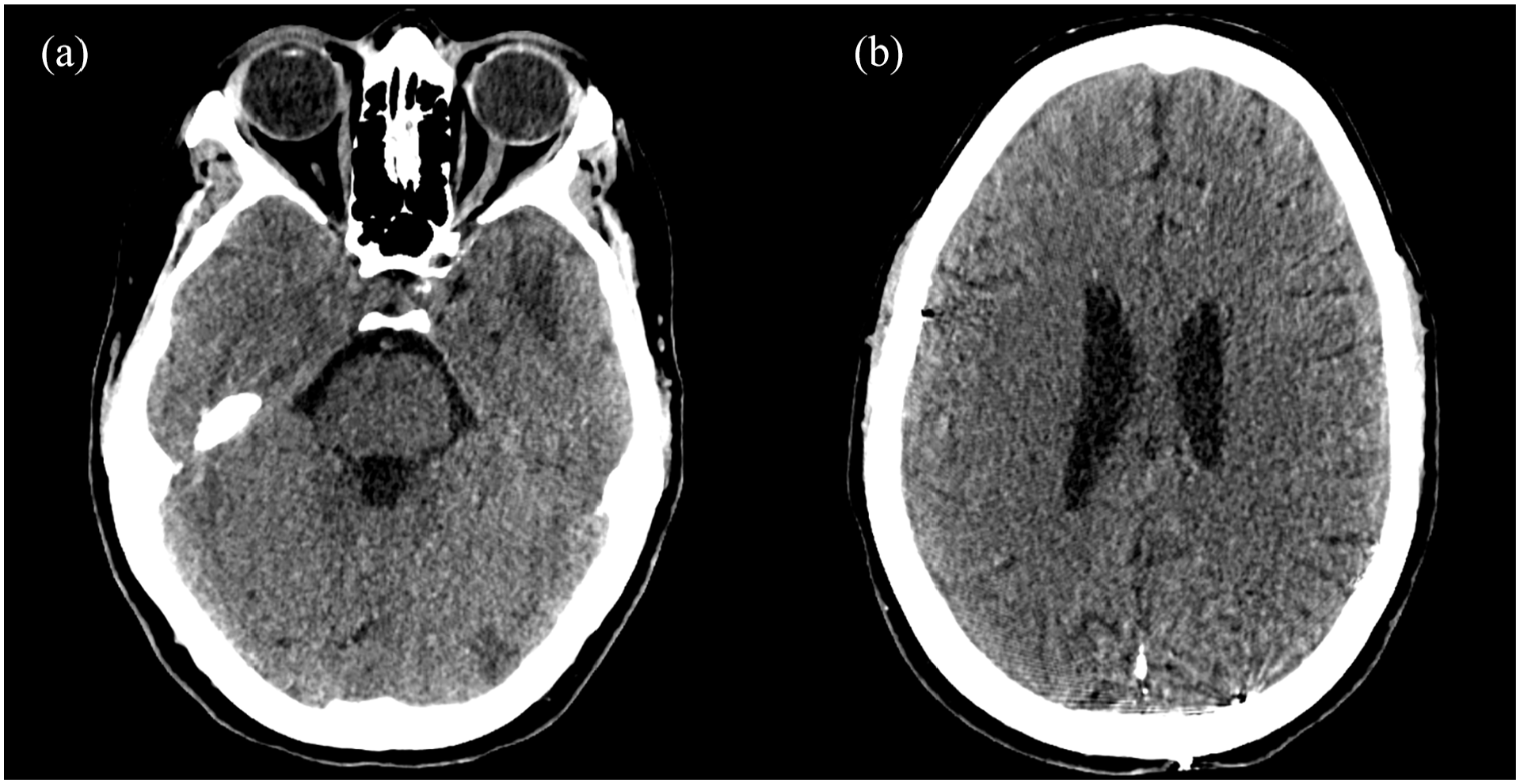
CT scan 4 months following the last admission. (a) Slice at the level of the previous temporal ICH, showing that the hematoma has been absorbed, leaving behind a hypodense area. (b) Slice at a level at the top of the ventricles, showing no residual cSDH.
Discussion
cSDH is a common neurosurgical condition, with a projected increase in incidence due to the aging population. 9 The usual treatment is conservative in asymptomatic or mildly symptomatic patients with low hematoma volume, 3 and surgical evacuation in symptomatic patients. 10 In recent years a new treatment modality has emerged in the form of MMA embolization on the afflicted side. 3
Embolization is a specialized procedure that requires an interventional radiology department with a neurointerventionalist experienced with the procedure. In contrast, burr-hole evacuation is a relatively simple procedure, available in all neurosurgical departments. Embolization does not provide immediate relief of the pressure effect caused by the cSDH and will probably only be considered as a stand-alone therapy in patients with mild symptoms, or in patients with a high risk associated with surgery, such as presented in our report.
Complications associated with MMA embolization are rare. Because catheterization is only performed in the ECA, the risk of stroke is low. 3 There is a risk of vision loss due to anastomosis between the MMA and ophthalmic artery, but this risk can be reduced by careful procedural technique. 3
A large multicenter study of 138 patients, showed a median reduction in hematoma size at the last follow-up of 71%, and only 6.5% of patients required further cSDH treatment. 11 In comparison, burr-hole surgery is associated with recurrence rates ranging from 3% to more than 30%. 3 The recently published STEM trial found that embolization as an adjunct to standard treatment (both surgical and conservative), reduced the risk of treatment failure: OR 0.36. 12 The MAGIC-MT trial, conducted in a similar fashion, did not reach statistical significance, but subgroup analysis showed a reduced risk of serious adverse events in the embolization group: relative risk (RR) 0.58. 13 The EMBOLISE trial showed that supplementing traditional burr-hole surgery with embolization reduces the risk of hematoma recurrence: RR 0.36. 14 Following these promising results, a recent consensus-based statement was released, recommending that MMA embolization should be considered as a treatment for both de novo, and recurrent cSDH in patients with coagulopathy or on antithrombotics, as in this case. It should also be considered as an adjunct to surgery in all recurrent cSDH. 15
The literature on cSDH in patients with APS is sparse. A recent meta-analysis comparing direct oral anticoagulants and vitamin K antagonists in this patient group shows a risk of major bleeding (of which cSDH is a subgroup) of 4.2%–4.3%, 16 indicating that cSDH is a relatively rare complication. In Danish patients in general, treatment with a combination of vitamin K antagonists and low-dose aspirin is associated with an increased risk of cSDH: OR, 4.00 (95% CI, 3.40–4.70). 17
Conclusion
While the development of cSDH in patients on anticoagulants is a common neurosurgical problem, this case describes the challenges of managing a patient with APS. Complete discontinuation of anticoagulant therapy carries a high risk of thromboembolic events, and traditional burr-hole surgery in the anticoagulated patient would also be associated with a high risk. Embolization of the MMA is an emerging treatment modality that was successfully applied in this complicated case. We suggest that embolization should be considered in similar cases of cSDH, where a prolonged period of discontinued anticoagulant therapy is associated with a high risk.
Footnotes
Author contributions
K.A.A.: writing—original draft, writing—review & editing, visualization. H.B.E.: writing—review & editing, supervision. H.V.G.N.: writing—review & editing, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.