
Abstract
Treatment of post-dissection arch and thoracoabdominal aortic aneurysms presents significant therapeutic challenges. True lumen collapse or take off of aortic branches from the false lumen makes endograft alignment difficult, if not impossible. We present herein the first successful case of an extensive thoracoabdominal electro aortic septotomy of the entire dissection membrane from the aortic arch down to the aortic bifurcation during an open redo aortic arch replacement employing the frozen elephant trunk technique. The procedure was performed on a 59 years old female patient presenting with a progressive post-dissection aortic aneurysm during follow-up with a maximum diameter of 6 cm 11 years after operating on an acute type A aortic dissection. Due to the extensive longitudinal aortic electric septotomy, we created a new “common lumen” for subsequent endovascular completion of the repair.
Introduction
Aortic dissection is one of the most acute life-threatening diseases. Despite improvements in diagnostics, medical therapy, and surgical technique, patient mortality and morbidity remain high. 1 Surgery is the treatment of choice for patients with type A aortic dissection. Replacement of the ascending aorta with resection of the entry site leaves the downstream dissected aorta untouched. In the majority of patients, a residual dissection membrane remains with a patent false lumen. Due to the patent false lumen in the descending aortic segments, a proportion of patients will develop post-dissection aneurysms requiring further therapy during follow-up due to aortic dilatation. 2
Management of aortic arch and thoraco-abdominal dissecting aneurysms is complex, and the best treatment option depends on many factors. Besides patient comorbidities, there are some technical and anatomical issues. The proximal sealing zone often involves the aortic arch. Furthermore, a narrow true lumen does not allow endograft release because of the risk of aortic obstruction. Even aortic branches may take off from the false lumen. This may limit endovascular options in these patients while open thoraco-abdominal replacement remains a highest-risk surgery.
To the best of our knowledge, we present herein the first successful case of a hybrid approach (patent pending) with electrocautery septotomy of the entire dissection membrane from the aortic arch down to the aortic bifurcation to create a common lumen for proper subsequent endovascular completion of the thoraco-abdominal aortic repair.
Case report
A 59-year-old woman with a history of hypertension and chronic renal insufficiency presented with an acute aortic dissection Typ A in 2010. Replacement of the ascending aorta was performed in a standard fashion with an open distal anastomosis. On follow-up, she was found to have a persistent false lumen which compressed the true lumen at the level of the distal descending and abdominal aorta. Over the last 6 months, there was a substantial increase in aortic diameter (>10 mm) (Figures 1 and 2). Against this background, we decided to go for a novel hybrid approach. Written informed consent of the patient was obtained and our institutional review board approved the procedure.
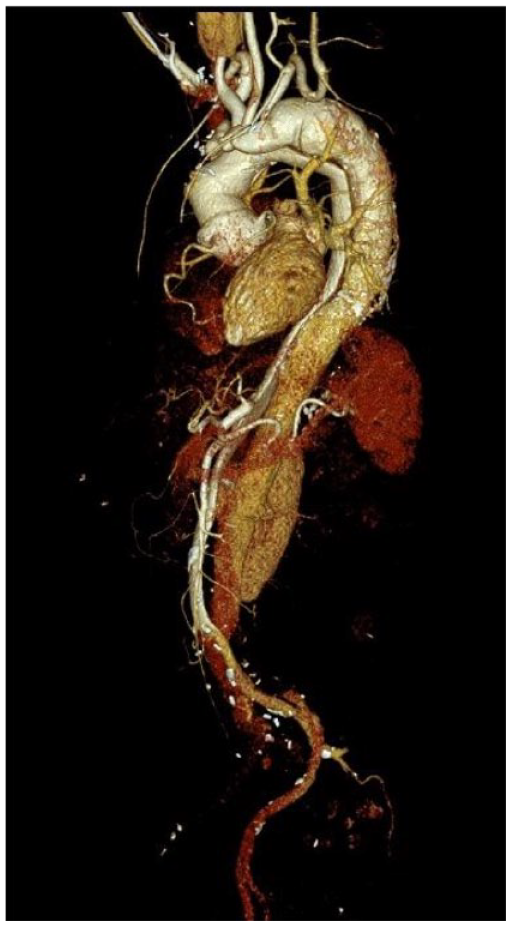
Contrast-enhanced computed tomography prior fenestrating the aortic dissection membrane showing a narrow true lumen and take-off of side branches from the false lumen.

Axial contrast-enhanced CT scan showing the situation prior surgery. (A) Overall diameter measuring 62 mm at the level of the suprarenal aorta. This image reveals the narrow true lumen and the patent false lumen. (B) Offspring of the left renal artery from the false lumen.
On May 12, 2021 the redo-arch procedure took place in our hybrid OR. During selective bilateral antegrade cerebral perfusion at 28° bladder temperature, the aortic arch was resected sparing the island of the supra-aortic vessels. In a second step, both femoral arteries were punctured and two guiding catheters were positioned in the true and false lumen, respectively. An Astato Wire (Asahi Intecc, USA) was advanced through the catheter within the false lumen and inserted into the catheter within the true lumen under direct vision during (Figure 3(a)). The sharp V-shaped Astato Wire was insulated in a microcatheter (Piggyback Wire Convertor, Teleflex, Wayne, PA, USA) to confine the electrical current to the tip and electrified using a radiofrequency generator (ForceFx Valley Lab, Minneapolis, MN, USA) to fenestrate the dissection membrane. As a first step, this was done under direct vision and angioscopy guidance during circulatory arrest down to the level of the mid-descending aorta (Figures 3(b) and 4). Following this maneuver, surgical completion of the FET implantation was accomplished in a standard fashion with the E-vita open NEO straight 30/30/120 mm prosthesis (ARTIVION, Hechingen, Germany). At the end of surgery, as a second step, we completed electrocautery fenestration of the dissection membrane down to the level of the aortic bifurcation under angiography guidance. This procedure was only done under two-dimensional fluoroscopy guidance. Radiopaque agent was administered approximately every 5 cm to check for proper alignment of the catheter. At this point, we were able to confirm a newly created common aortic lumen, including perfusion of all aortic branches. Then a descending thoracic endograft was placed with the distal TEVAR ending just proximal to the celiac trunk (Figure 3(c)). This way we created a perfect proximal landing zone for subsequent endovascular repair which was revealed in the postoperative CT scan. Furthermore, a successful septotomy was confirmed in the computed tomographic imaging. Final endovascular completion of the aortic repair was achieved 6 weeks later with a company-manufactured fenestrated endograft (Anaconda Terumo Aortic, Vascutek Ltd, Inchinnan, UK). Final imaging showed a satisfactory result with stent coverage of the entire descending and abdominal aorta and perfusion of all side branches (Figure 5). Currently, the patient is on follow-up in a routine fashion and she is doing well in daily life.
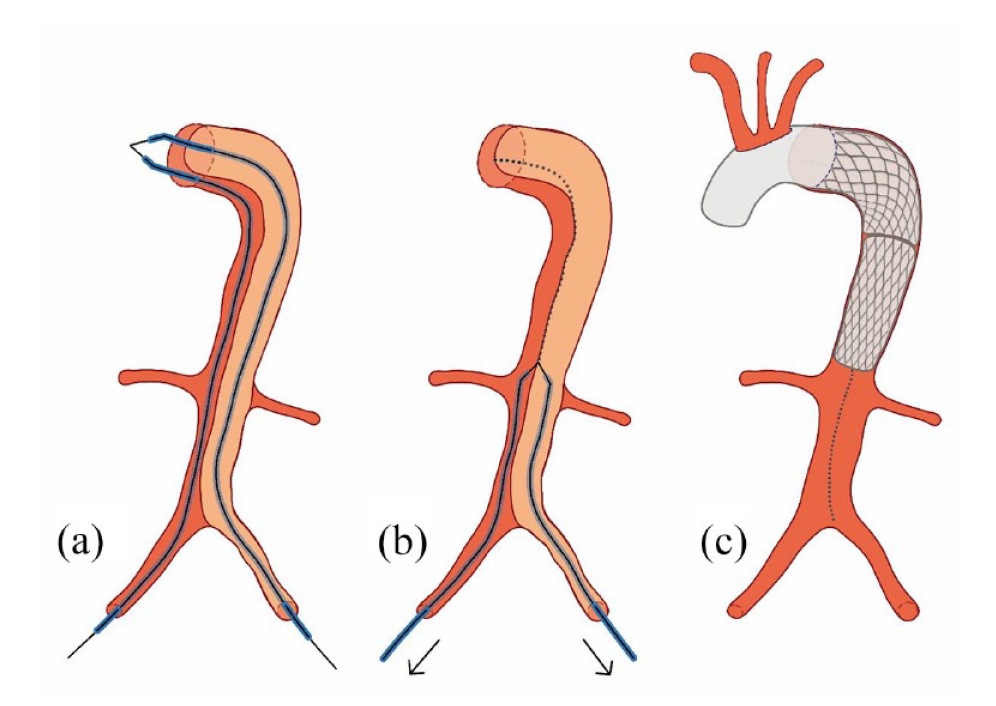
Schematic diagram of the procedure. Snaring under direct vision (a) and electrocautery fenestration of the aortic dissection membrane during circulatory arrest down to the mid-descending aorta (b). After aortic arch replacement with the FET technique, completion of electro-aortic slicing down to aortic bifurcation and implanting a thoracic endograft proximal to the celiac trunk (c). This hybrid approach was the first step in the complete aortic repair and was premising for subsequent fenestrated EVAR.

Endoscopic guided septotomy of the dissection membrane.

Final result after complete aortic repair.
Discussion
The treatment of post-dissection aortic aneurysms, both open and endovascular repair, is a challenging task, and it is associated with appreciable postoperative morbidity and mortality. 3 Indeed, open repair of thoracoabdominal aneurysm is associated with reported 30-day mortality rates as high as 19%–31%. 4 Planning of the procedure must consider all steps and possible obstacles to treatment success.
Often there is no appropriate proximal sealing zone. This makes a hybrid approach mandatory, as described in our case. As in our patient with a chronic aortic dissection, a narrow true lumen can be present. This may challenge positioning and releasing of the endograft. To overcome this difficulty, we made an electrocautery septotomy of the chronic dissection membrane similarly described by the BASILICA technique for degenerated surgical bioprosthesis. 5 This complete septotomy guarantees that all aortic branches take off from the newly created common aortic lumen.
To the best of our knowledge, a complete thoracoabdominal electrical septotomy of an entire dissection membrane from the aortic arch down to the level of the aortic bifurcation has never been done/described before. Accordingly, also the combination of the procedures (aortic arch replacement using FET technique, complete electrical septotomy, and subsequent EVAR) was not described until now and makes this case unique.
The only established alternative to the technique described herein is the “classic” cheesewire septotomy. This approach has been associated with a high risk of complications due to the fact that the septotomy itself can hardly be controlled in any manner. Electrosurgical septotomy to date has only been performed in combination with subsequent local balloon dilatation of the dissection membrane.
Our novel approach of controlled and complete thoracoabdominal electrical septotomy of the entire dissection membrane can potentially be employed in any patient with a chronic aortic dissection. This includes historical contraindications for endovascular aortic repair, such as a compressed true lumen or take-off of visceral arteries from the false lumen.
We hope that this new technique may help in successfully treating these most challenging cases.
Conclusion
The described method of an extensive thoracoabdominal electro aortic septotomy has been proofed to be feasible. The created new common lumen may facilitate subsequent total endovascular repair in patients otherwise only treatable with a high-risk surgical thoracoabdominal aortic replacement. Due to pending patents, we were not able to submit our manuscript in advance.
Footnotes
Acknowledgements
None.
Author contributions
All authors have made substantial contributions to the conception and design, have been involved in drafting the manuscript and revising it critically for important intellectual content, and have given final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Zierer is a proctor for ARTIVION and receives speaker fees from ARTIVION and an educational grant.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Prof. Zierer is a proctor for ARTIVION and receives speaker fees from ARTIVION and an educational grant.
Ethics approval
Ethical approval to report this case was obtained from *Ethics committee, Johannes Kepler University, Linz, Wagner-Jauregg-Weg 15, 4020 Linz; EK Nr:1281/2020.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.