
Abstract
Ortner’s syndrome, also known as cardiovocal syndrome, is a rare presentation of aortic dissection. Symptoms occur as a result of recurrent laryngeal nerve compression. Our report describes a case of a patient who complained of hoarseness for a few months and was eventually diagnosed with chronic aortic dissection.
Introduction
Aortic dissection is a life-threatening disease and can present with a myriad of symptoms including back pain, stomach pain, loss of consciousness, and neurological symptoms. 1
Due to the anatomical location of the structures, the expansion of the aorta may compress the recurrent laryngeal nerve which leads to hoarseness of voice. This presentation is termed Ortner’s syndrome, also known as cardiovocal syndrome. 2 Our report describes a case of a patient who complained of hoarseness for approximately 3 months and was ultimately diagnosed with chronic aortic dissection.
Case
A 68-year-old male patient presented to his primary care provider with complaints of hoarseness for the past 3 months. He had a history of end-stage renal disease on hemodialysis, heart failure with reduced ejection fraction, atrial fibrillation with a Watchman device, which is a device that closes off the left atrial appendage to prevent thrombuses from forming in that location, a previously diagnosed Stanford type B aortic dissection that was treated non-surgically, peripheral arterial disease (PAD), bladder cancer, chronic obstructive pulmonary disease (COPD), hepatitis C, hypertension, obstructive sleep apnea on continuous positive airway pressure (CPAP), hyperparathyroidism, non-alcoholic fatty liver disease (NAFLD), and ongoing tobacco use. He did not have dysphagia to liquids or solids, weight loss, poor appetite, hemoptysis, night sweats, gastroesophageal reflux disease, or difficulty initiating swallowing.
He underwent further evaluation by an otorhinolaryngologist (ENT), where a nasolaryngoscopy revealed left vocal cord paralysis and incomplete vocal cord closure. Due to suspicion for malignancy with the patient’s smoking history, he underwent computed tomography (CT) scan with contrast of his neck. The scan demonstrated a partially visualized Stanford type A aortic dissection (Figure 1). A dedicated CT thorax with contrast confirmed the presence of a Stanford type A aortic dissection extending from the aortic root up to the arch (Figure 2). The aneurysmal dilatation of the ascending aorta measured up to 5.2 cm. Furthermore, the known chronic Stanford type B dissection involving the descending aorta was also visualized (Figures 1 and 2).
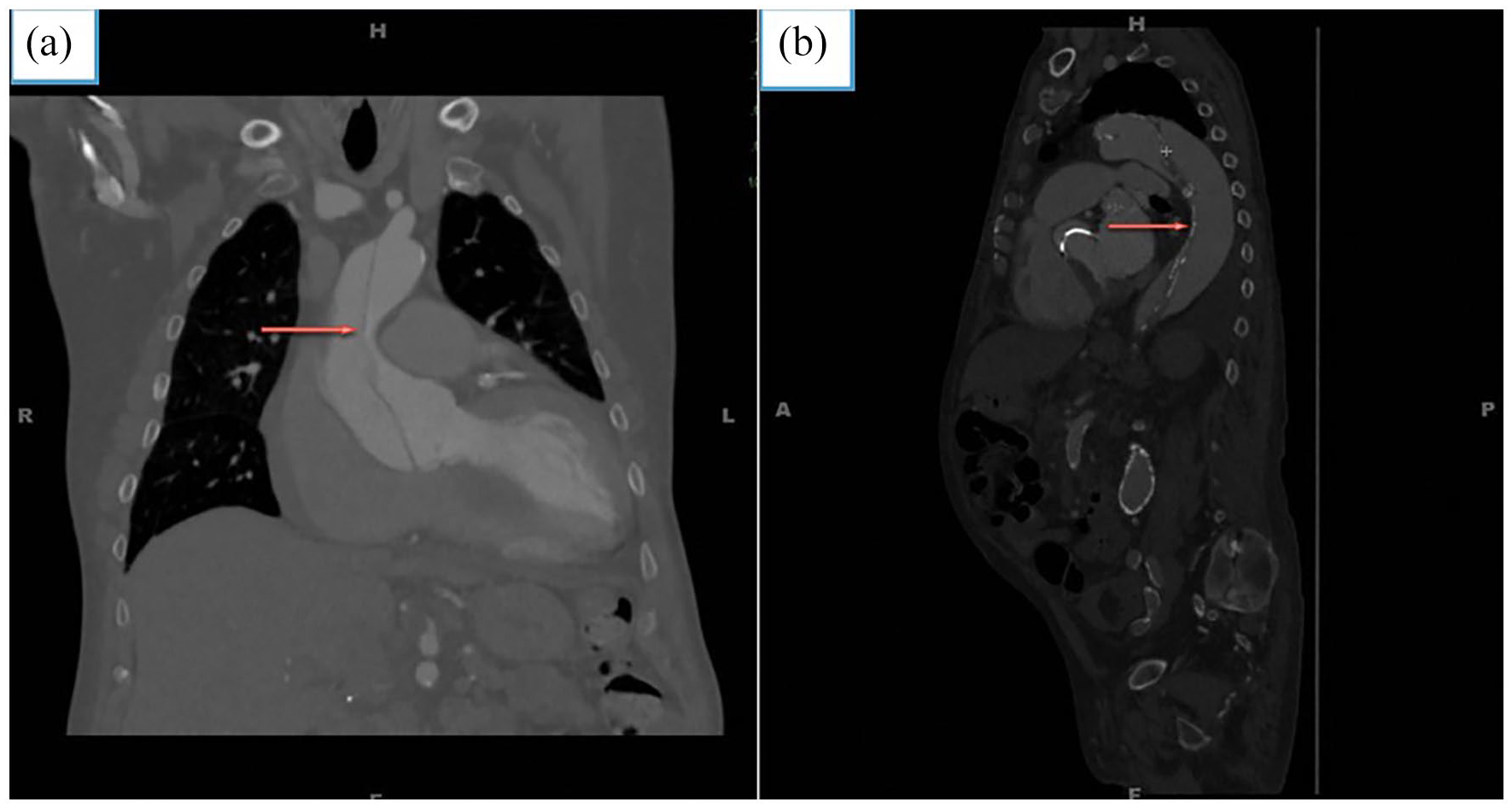
Contrast-enhanced computed tomography of the thorax in coronal (a) and sagittal (b) view showing aortic dissection with intimal flap (arrow) separating true anteriorly and false lumen posteriorly.

Contrast-enhanced computed tomography of the thorax in coronal section showing the presence of type A aortic dissection extending from the aortic root up to the arch with an aneurysmal dilatation of the ascending aorta measuring 5.2 cm (arrows).
He was urgently evaluated by cardiothoracic surgery and underwent repair of his type A aortic dissection. His hospital course was complicated by upper gastrointestinal (GI) bleeding that required a transfusion. The source of the GI bleed was found to be a duodenal ulcer. After surgery, he developed delirium and colonic ileus that resolved toward the end of his hospital stay. He also developed a recurrence of atrial fibrillation. He remained in atrial fibrillation post-discharge. His anticoagulation with warfarin was discontinued as the patient had previously undergone a Watchman device placement. The patient was discharged to physical therapy after 20 days. Subsequent outpatient follow-up revealed that the hoarseness was resolving slowly.
Discussion
Aortic dissection is a life-threatening cardiac emergency with an incidence rate ranging from 2.6 to 3.5 per case per 100,000 individuals.1,3 Aortic dissection is defined as the detachment of the aortic wall layers due to an intimal tear. 4 Aortic dissection can occur spontaneously or result from iatrogenic injury. Aortic dissection can arise in the ascending aorta (termed Stanford type A), descending aorta, and abdominal aorta (collectively termed type B). The treatment for the two types differs with Stanford type A treated surgically and Stanford type B treated medically. The ascending aorta is affected in 65% of the cases. 5
Several structures can be involved when aortic dissection occurs, such as the coronary arteries, aortic valve, or the thoracic/abdominal aorta branches. The location and structures involved frequently dictate the patient’s presenting symptoms, whether cardiovascular, neurological, GI, or a combination of the above. The most common clinical manifestation of aortic dissection is the severe and sudden retrosternal chest pain radiating to the back. Approximately, 10% of aortic dissections are painless and present with signs and symptoms resultant of the complications of the propagating dissection. About 20%–30% of these patients present with neurological complications, stroke being the most common manifestation.6,7
The factors contributing to aortic dissection include hypertension, cocaine use, atherosclerosis, prior cardiac surgery, known aneurysm, known connective tissue disorder, bicuspid aortic valve, and prior aortic surgery.4,8 The sudden increase in blood pressure creates an intimal tear that forces the intimal layer to separate from the muscular and/or the adventitial layer. Involvement of the coronary arteries, aortic valve, or the branches of the thoracic or abdominal aorta by the disseminating dissection results in chest pain or neurological complications. 9
The presented case illustrates the importance of including aortic dissection in the differential for a patient presenting with hoarseness. This very rare presentation is known as cardiovocal syndrome or Ortner’s syndrome. It was first described in 1897 and was due to recurrent laryngeal nerve involvement. 10 Due to the long course of the left recurrent laryngeal nerve and its association with the nearby cardiovascular structures in the mediastinum, left vocal cord palsy is most commonly reported. Ortner’s syndrome was seen in accordance with mitral stenosis, cor-pulmonale, pulmonary hypertension, aortopulmonary window, Ebstein’s anomaly, aortic aneurysms, and aortic dissections.5,10,11 Previously written case reports have highlighted varying presentations of patients with aortic dissections. These include stroke, paraplegia, syncope, transverse myelopathy, hoarseness, dysphagia, and lower extremity numbness.6,12– 16
As a minority of aortic dissections are painless, they are usually diagnosed within weeks to years of onset. 17 CT angiogram with contrast is the imaging modality of choice in the diagnosis of aortic dissection and should be performed from the skull base to mid-thorax when an unknown cause of newly diagnosed vocal cord palsy is noted. 18 A transthoracic echocardiogram or transesophageal echocardiogram may also aid in the diagnosis of an aortic dissection.
After appropriate management and treatment of aortic dissection, the prognosis of Ortner’s syndrome was noted to be better when the diagnosis and treatment were offered early in the disease course before fibrosis and perineural scarring of the recurrent laryngeal nerve occurred. 15 A study by Teixido and Leonetti, including 168 patients with aortic aneurysms, revealed that eight patients in the study population exhibited hoarseness secondary to recurrent laryngeal nerve palsy of which only one patient regained vocal cord function after surgical correction of the aneurysm. 19 Our patient reported mild improvement of his hoarseness post-aortic aneurysm repair confirming that the cause of his hoarseness was caused by the aortic dissection.
Conclusion
Aortic dissection is an entity that is associated with high mortality, and treatment should be initiated as early as possible. However, a minority of patients with aortic dissection may remain painless for weeks to years, delaying diagnosis and treatment. Aortic dissection can present with a wide spectrum of symptoms, including hoarseness, as seen in cardiovocal or Ortner’s syndrome. Early recognition and treatment are imperative in such cases.
Footnotes
Acknowledgements
All authors have participated in the drafting and revision of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.