
Abstract
A 40-year-old man underwent ascending aorta replacement for an acute type A aortic dissection. After the operations, methicillin-resistant Staphylococcus aureus was identified in sputum and blood cultures. Although anti-methicillin-resistant Staphylococcus aureus drugs were administered, most of the intermittent blood cultures remained positive. The focus of methicillin-resistant Staphylococcus aureus infection was not evident in the early stages, and no specific symptoms such as abscess or endocarditis were observed. However, abscesses in the brain, mediastinum and spleen were found 3 years after the operation. The minimum inhibitory concentration of vancomycin gradually increased from 1 to 4 µg/mL during the course of treatment. This case provides evidence for a potential role of combination therapy.
Introduction
Bacterial infection following cardiovascular surgery is sometimes fatal, and the prevention of infection is crucial. In particular, a methicillin-resistant Staphylococcus aureus (MRSA) infection often hampers treatment. In this article, we report a patient who had persistent MRSA bacteremia for 3 years following surgery for a thoracic aortic dissection despite various medical therapies.
Case report
Written informed consent was obtained from the patient’s parent for publication of this case and images in an international medical journal. Our institution does not require ethical approval for reporting individual cases.
A 40-year-old man with no pertinent past medical history was admitted to our hospital with severe chest and back pain. Enhanced computed tomography (CT) revealed dissection of the ascending aorta (Figure 1(a)). On admission (June 2009), emergency surgery was performed through a median sternotomy for vascular prosthesis placement. On the 6th post-operative day, the left leg and abdominal organs had become ischemic due to malperfusion, and femoral–femoral artery bypass was performed. Despite this intervention, the ischemia did not improve, so the patient underwent right subclavian artery to femoral artery bypass and amputation of the left leg. On the 8th day after the first operation, the body temperature increased to 39.5°C, and MRSA was identified in sputum and blood cultures. Intravenous arbekacin (ABK) administration was started but did not appear to be effective. The antibiotic was switched to vancomycin (VCM), and the general condition improved, but blood cultures remained positive for MRSA. ABK was restarted after the femoral–femoral artery bypass; however, the blood cultures remained positive. Renal impairment required an adjustment of the VCM dosage. After 2 weeks, serum C-reactive protein (CRP) was decreased and body temperature decreased to 36°C. Intravenous administration of VCM was continued for 4 weeks to prevent biofilm formation. The trough value of VCM was maintained at 15–20 µg/mL because the minimum inhibitory concentration (MIC) of VCM was 2 µg/mL as determined by automated antimicrobial susceptibility testing system VITEK2® (Sysmex bioMérieux, Tokyo, Japan). In August, body temperature rose again and MRSA was detected in the blood culture. Because the MIC of VCM remained 2 µg/mL, VCM was switched to linezolid (LZD). Although LZD seemed effective and body temperature fell, the platelet count dropped to 8.0 × 104/µL so LZD had to be discontinued. Soon after LZD was stopped, body temperature rose again, and teicoplanin (TEIC) was started. Body temperature remained high despite the adequate trough level (15–20 µg/mL), and LZD was restarted because the platelet count recovered. During these therapies, renal function gradually worsened, and hemodialysis (HD) was started in December 2009. After HD initiation, VCM was started again because of thrombocytopenia. Renal function improved and the patient was weaned off HD in January 2010. At that time, MRSA remained positive in blood cultures, and the MIC for VCM increased to 4 µg/mL. VCM was switched to a combination of LZD, erythromycin (EM), and rifampicin (RFP). After several weeks of this treatment, LZD was again switched to VCM because of thrombocytopenia. By continuing this therapy, blood cultures became negative. In April 2010, VCM was discontinued and inflammatory findings were controlled by EM and RFP treatment. The patient was discharged in July 2010 (the 390th hospital day) for outpatient follow-up care (Figure 2).

(a) On initial admission, enhanced CT revealed aortic dissection from the ascending (left arrow) to descending (right arrow) aorta and (b) on the third admission, CT scanning revealed an abscess around the artificial ascending aorta (arrows).

Clinical course of the first admission. Bars indicate duration of various anti-MRSA drug administrations.
In February 2011, the patient was readmitted to the hospital because of left hemiplegia due to a brain abscess (Figure 3). On this second admission, blood cultures were positive for MRSA, and VCM was administered to control infection even though the MIC was 2 µg/mL. In March, craniotomy for brain abscess excision was performed. After the operation, because of the MIC of VCM and the difficulty of intravenous administration, intramuscular administration of ABK was started. As renal function gradually worsened again (blood urea nitrogen (BUN) = 38.9 mg/dL, creatinine (CRE) = 4.26 mg/dL), ABK was switched to LZD. Because of subsequent thrombocytopenia, LZD was switched to TEIC, but renal function still worsened (BUN = 62.9 mg/dL, CRE = 8.20 mg/dL). Therefore, maintenance HD was introduced in April 2011. Afterwards, VCM was restarted, but fever occurred and CRP remained high in spite of an adequate VCM trough level. The MIC for VCM was then 4 µg/mL, suggesting presence of vancomycin-intermediate Staphylococcus aureus (VISA) which was confirmed with E-test® (Sysmex bioMérieux, Tokyo, Japan). LZD was restarted, but thrombocytopenia occurred within 20 days of the switch. Subsequently, VCM and LZD were used in turn because of the platelet count. To detect the focus of the MRSA infection, Gallium-67 scintigraphy was performed; abnormal uptake was detected in the spleen and right kidney (Figure 4). Therapy with VCM or LZD continued for 7 months. In December 2011, antimicrobial therapy was discontinued as CRP returned to normal levels as the blood cultures were negative; however, fever resumed shortly, and an increase in CRP was observed. Therefore, daptomycin (DAP) was started and body temperature was reduced. The patient was discharged in December 2011. At home, fever was observed again, and the patient was readmitted to the hospital in January 2012 (Figure 5).
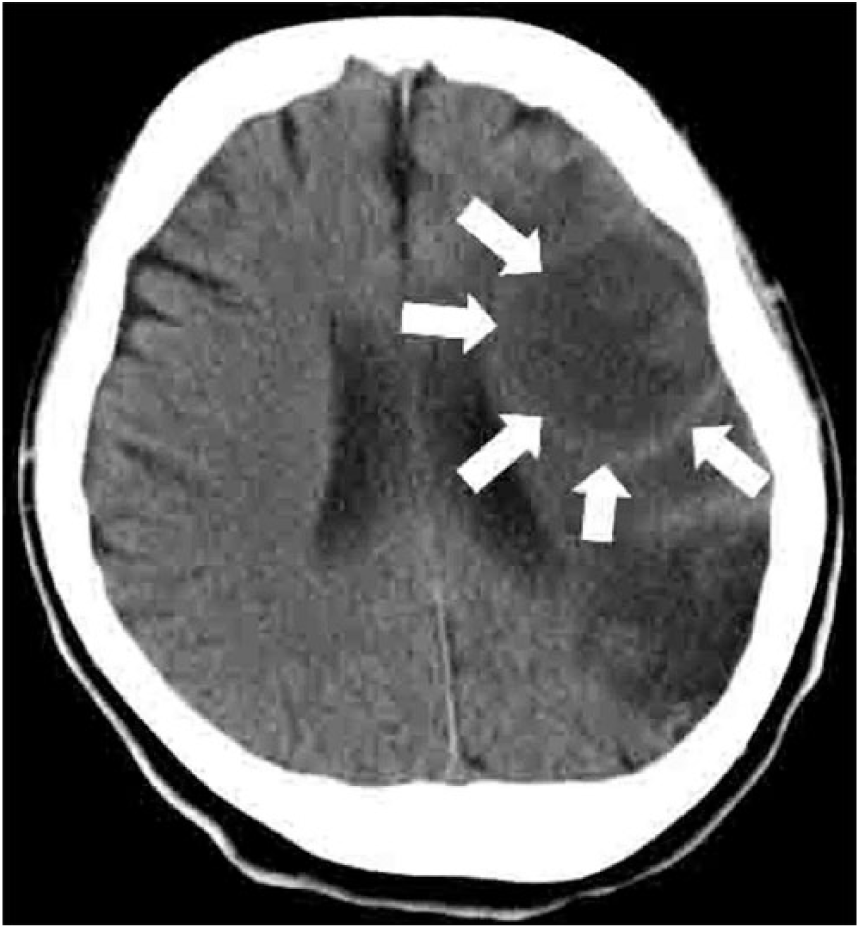
CT scanning due to left hemiplegia revealed brain abscess (arrows).

Gallium-67 scintigraphy revealed accumulation in the spleen and right kidney. The image is indicative of splenic abscess (right arrow) and pyelitis of the right kidney (left arrow).
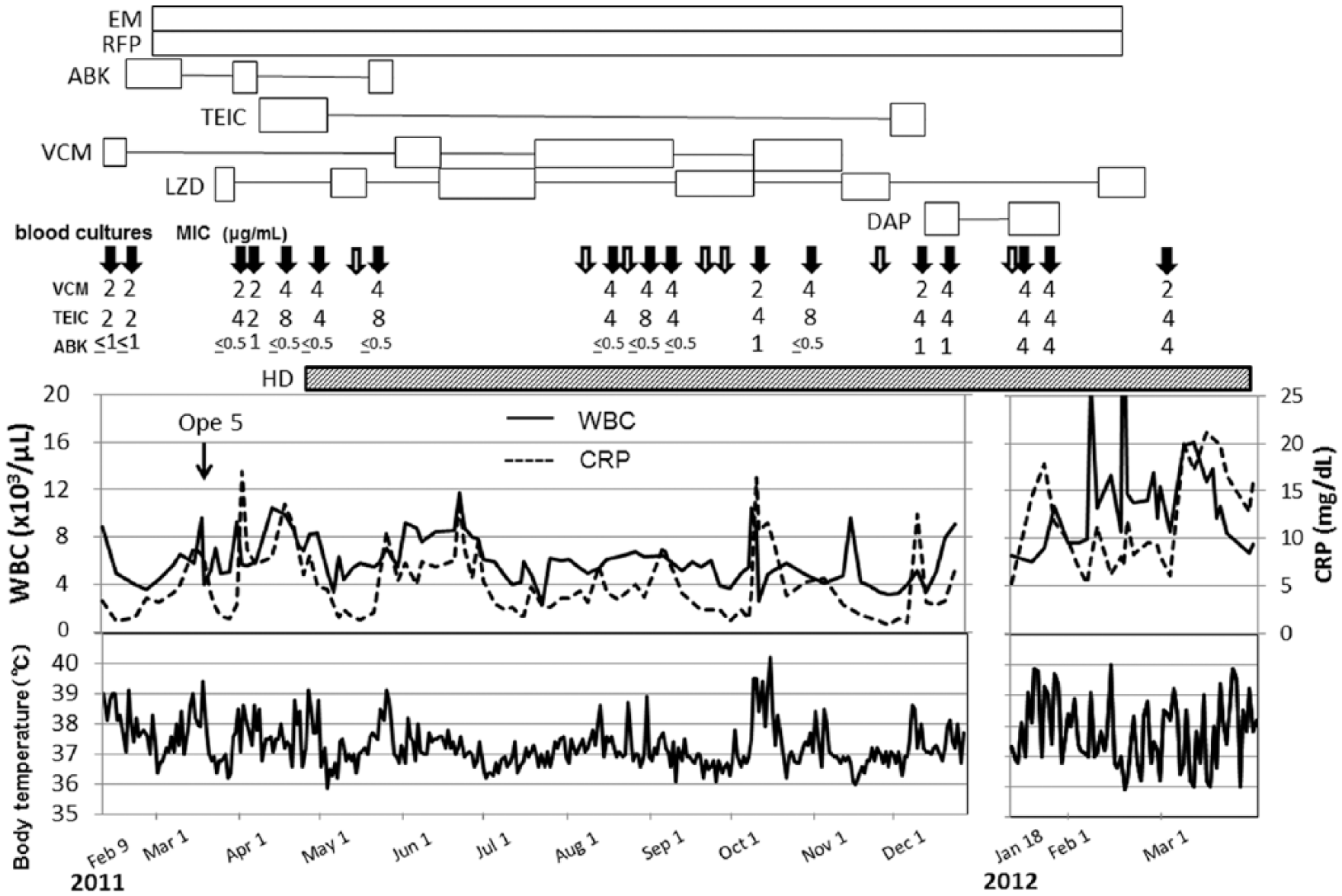
Clinical course of the second and third admissions. Bars indicate duration of various anti-MRSA drug administrations.
On the third admission, DAP was restarted but high fever continued. EM and RFP had been administered continuously since the previous hospitalization. VISA was detected in blood cultures. And then, enlargement of the chest surgical scar was found. CT scanning revealed an abscess around the artificial ascending aorta (Figure 1(b)). Incision and drainage were performed, and vacuum-assisted closure (VAC) therapy accompanied by VCM or LZD administration was started. However, control of the infection was not possible; therefore, best supportive care was chosen as the treatment course. Opioids were administered for the chest pain. Despite all treatment efforts, the patient expired in April 2012 (Figure 5).
Autopsy findings
Autopsy was performed, and the final pathological diagnoses were as follows: (1) septicemia, (2) dissecting aortic aneurysm with hematoma, and (3) status-post replacement by artificial vessel, femoral–femoral artery bypass, and right subclavian artery to femoral artery bypass. Infectious organisms (gram-positive cocci noted) were found in ulcerations around the artificial vessel. The liver (1950 g) and spleen (500 g) were enlarged with inflammatory cell infiltration. Purulent pericarditis and pleurisy were found with abscess, and microabscesses were found in the kidneys.
Discussion
In this case, MRSA bacteremia persisted for 3 years. Given the patient’s course, a vascular prosthesis was likely infected as a result of a surgical site infection (SSI). An MRSA infection during prosthesis insertion is likely to require removal of the prosthesis, 1 and this approach was considered in the current case. Because the patient had an aortic dissection with malperfusion, successful removal of the prosthesis seemed unlikely after the operation. The only reasonable option was to administer antibiotics. The patient was treated with various anti-MRSA drugs without lasting success, including ABK which was an aminoglycoside antibiotic available in our country and was reported to be effective for surgical MRSA infection. 2 LZD, which acts via a different mechanism from VCM and widely eradicates soft tissue, had the potential to be effective in our patient, but long-term administration was necessary because of its bacteriostatic performance.3–5 It later had to be abandoned due to adverse effects. 6 Thus, it was not likely to be a complete cure of an infection that had spread throughout the body, as in this patient. TEIC, which is a glycopeptide antibiotic similar to VCM, was also administered in turn because the nephrotoxicity is less than that of VCM, 7 but it was still difficult to control the infection.
MRSA developed into VISA during the patient’s first hospitalization, and use of VCM in combination with other drugs had to be carefully considered. Long-term use of VCM can readily lead to an elevated MIC. 8 In this case, the MIC of VCM was initially 0.5 µg/mL but ultimately increased to 4 µg/mL. In this case, genetic studies using pulsed field gel electrophoresis could not be performed, so it was difficult to determine whether the S. aureus had acquired resistance or if the patient had been infected with a new resistant strain; however, the latter scenario seems unlikely. Presumably, S. aureus gradually acquired resistance and the MIC increased. Cui et al. 9 and Hanaki et al. 10 reported that the low VCM susceptibility factor indicates activated synthesis and an increased rate of cell-wall turnover during long-term VCM use. Because of decreased renal function with long-term administration of VCM or ABK, combined therapy with RFP and EM was chosen. RFP kills surface-adhering, slow-growing, and biofilm-producing bacteria. 11 EM affects the immune response. 12 Administration of RFP alone can quickly enhance resistance so it should not be used alone.13,14 DAP, which had just become available in Japan, was used from the latter part of the second admission to the first part of the third admission; however, DAP was not effective in this case, indicating cross-resistance caused using VCM before DAP administration.15,16
Concerning the source of infection, formation of biofilm on the vascular prosthesis is the most likely explanation. Because the prosthesis was not replaced and the biofilm was not removed by additional surgery, the persistent MRSA infection could not be controlled. Regrettably, the patient’s general condition was poor, reducing the likelihood of surviving remedial surgery so we chose to continue antibiotic therapy for the MRSA infection. Although various tests were performed to identify the source of infection, we could not determine the initial MRSA infection site. CT scanning was performed several times, but there was no clear infection site. At the beginning, there might have been microabscesses or biofilm which could not be found by CT resolution. An autopsy failed to reveal formation of an obvious biofilm, but erosion of the distal vascular prosthesis suture sites and invasion of inflammatory cells were noted. Therefore, the presence of MRSA on the artificial material may have played a role in this prolonged infection. In addition, formation of microabscesses in the kidneys was noted, indicating a secondary infection.
Conclusion
We experienced a case with persistent MRSA infection after vascular prosthesis. Although the removal and/or exchange of the vascular prosthesis would have been the best way to control infection, we were unable to remove it for medical reasons and had to continue antimicrobial therapy. The persistent MRSA infection may have led to a decrease in susceptibility to VCM.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.