
Abstract
Hyalinizing clear cell carcinoma is an uncommon neoplasm arising in minor salivary glands. We present a rare case of hyalinizing clear cell carcinoma in the base of the tongue. We report a case of a 38-year-old female presented with a progressive history of hemoptysis and dysphagia over the course of 4 years. Examination revealed a mass originating from the base of the tongue with a biopsy confirmed as hyalinizing clear cell carcinoma . An Ovid MEDLINE and PubMed literature review was conducted due to the rarity of this type of tumor. The patient underwent surgical excision with immediate reconstruction with radial forearm free flap followed with adjuvant radiotherapy and was disease free at her most recent follow-up (12 months). Our review included a total of 13 new cases, including our case. The majority of the cases presented with dysphagia. Surgical excision is the mainstay of treatment, and overall these patients have a good prognosis. Our case highlights a rare presentation of hyalinizing clear cell carcinoma of the base of the tongue, successfully treated with surgical excision, free tissue reconstruction and adjuvant radiotherapy.
Introduction
Hyalinizing clear cell carcinoma (HCCC) is a malignant salivary gland tumour with distinct pathological features typically located in minor salivary glands, specifically the hard and soft palate,1–3 and accounts for 1% of all salivary gland cancers as described in 1994 by Milchgrub et al. HCCC is characterized by the appearance of clear cytoplasm in tumor cells under microscope due to the abundant presence of glycogen. 3 This microscopic features of HCCC overlaps with other salivary gland tumors, which add a challenge of diagnosis. The presentation of HCCC is often a slow-growing, painless mass and it is associated with a good overall prognosis with a very low chance of local recurrence. Moreover, while regional lymph node metastasis is very rare and reported in only few cases, the metastatic potential remains higher compared to other salivary gland carcinomas. 4 There are only a total of 35 cases reported in English literature of HCCC arising from the base of the tongue since 1994.
Herein, we describe a rare case of a HCCC found at the base of the tongue with evidence of regional lymph node metastasis along with a literature review of similar cases to highlight some of the challenges in diagnosis and management.
Case presentation
A 38-year-old female presented to The Ottawa Hospital’s outpatient clinic with a 2-week history of a sore throat superimposed on a 4-year history of haemoptysis. During this time, she was also experiencing progressive dysphagia and odynophagia. She had a history of weight loss, night sweats and generalised fatigue. She denied any dyspnoea or voice changes and was an otherwise healthy lifelong non-smoker with minimal alcohol consumption.
Initial evaluation revealed no distress. Examination of the oral cavity and oropharynx revealed a mass involving the left palatine tonsil. Fibreoptic examination confirmed the presence of an exophytic, non-ulcerative mass originating from the base of the tongue with superior extension to the tonsillar region. Examination of the neck demonstrated palpable level I cervical lymphadenopathy. Computed tomography (CT) scan of the neck showed enlargement of the left tonsil (29 mm × 52 mm × 32 mm) with narrowing of airway and enlargement of left level IB lymph node (Figure 1). The clinical picture at that point was mostly in keeping with lymphoma. As such, the patient provided written informed consent for awake intubation with a biopsy and debulking of the mass lesion.

Axial (a&c) and sagittal (b&d) CT scan cuts showing the mass occupying the oropharynx and obturating the majority of airway lumen.
On the day of the procedure, the patient was intubated without incident using an awake fibreoptic technique. Laryngoscopy was performed using a Dedo Laryngoscope and multiple biopsies of the mass were taken. These were sent fresh for lymphoma protocol. Next, debulking of approximately two-third of the mass was executed revealing a large mass with a thick stalk originating from the left base of the tongue. There were no complications.
Microscopic examination of the excised tissue demonstrated an infiltrative tumour limited to the submucosa. The tumour was composed of large cells with ample clear to eosinophilic cytoplasm. The tumour cells were embedded in a densely hyalinized stroma. Rare mitotic figures were identified but the overall mitotic rate was very low (less than 1 mitotic figure per 10 high-powered fields). Immunohistochemistry performed showed that the tumour cells were positive for cytokeratin 5, cytokeratin 7, p40, p63 and epithelial membrane antigen but were negative for glial fibrillary acidic protein, S-100 protein, SOX-10, smooth muscle antigen and muscle-specific antigen. The proliferative index as measured by the proliferation marker Ki-67 was less than 1%. RNA-based next-generation sequencing was performed and an EWSR1-ATF1 fusion was detected. Overall, these results were in keeping with HCCC.
MRI was then conducted demonstrating a mass with likely origin in the left base of the tongue with extension superiorly to the mid/inferior tonsillar pillar, anterior into the glossotonsillar sulcus and inferiorly into the vallecula. Additionally, it demonstrated an enlarged lymph node in left level IB measuring 11 mm. The case was discussed at our institutional multidisciplinary tumour board. The diagnosis of a T3N1M0 HCCC of the left oropharynx was agreed upon, as was an agreement for surgery as the primary modality of treatment.
The surgery consisted of a tracheostomy, transcervical transmandibular approach for wide excision of the lesion, along with neck dissection and radial forearm free flap for reconstruction. During the procedure, the lingual nerve was sacrificed to gain access to the tumour but was repaired at the end of the procedure. The intraoperative findings confirmed an exophytic mass originating from the left lateral pharyngeal wall/base of the tongue. Intraoperatively, the defect measured 5.5 cm × 6 cm in the left base of the tongue, extending laterally into the glossotonsillar area. The patient had an uneventful operative course and post-operative recovery. She went home 12 days later, without a tracheostomy or feeding tube, tolerating a pureed diet.
Gross examination of the tissue resected demonstrated a 3.9-cm mass protruding from the surface of the oropharynx (Figure 2(a)). Upon sectioning the tissue, the mass appeared as a tan/white, well-circumscribed lesion that occupied most of the specimen (Figure 2(b)). Microscopic examination revealed an infiltrative tumour composed of large cells with ample clear to eosinophilic cytoplasm (Figure 2(c)). The tumour cells were arranged in nests, sheets and small cysts and were embedded in a variably hyalinized myxoid stroma (Figure 2(d)). Perineural invasion and lymphovascular invasion were seen, and metastatic HCCC was identified in 2 of the 32 lymph nodes examined. No additional immunohistochemistry was performed on the resection specimen. The final pathologic stage was pT2, pN3b. As a result of tumour and lymph node high-risk features, post-operative adjuvant radiotherapy was recommended. The most recent follow-up was 12 months’ time without evidence of recurrence.

Hyalinizing clear cell carcinoma of the palatine tonsil. Grossly, the tumour appeared as an exophytic mass that protruded from the surface of the tonsil (a). In cross sections the mass was tan/white in colour, well demarcated and centred within the submucosa. The deep margin was free of tumour (b). The tumour was composed primarily of monomorphic population of large clear cells arranged in nests (c). The stroma surrounding the tumour cells varied from hyalinized to myxoid, a typical finding for hyalinizing clear cell carcinoma (d).
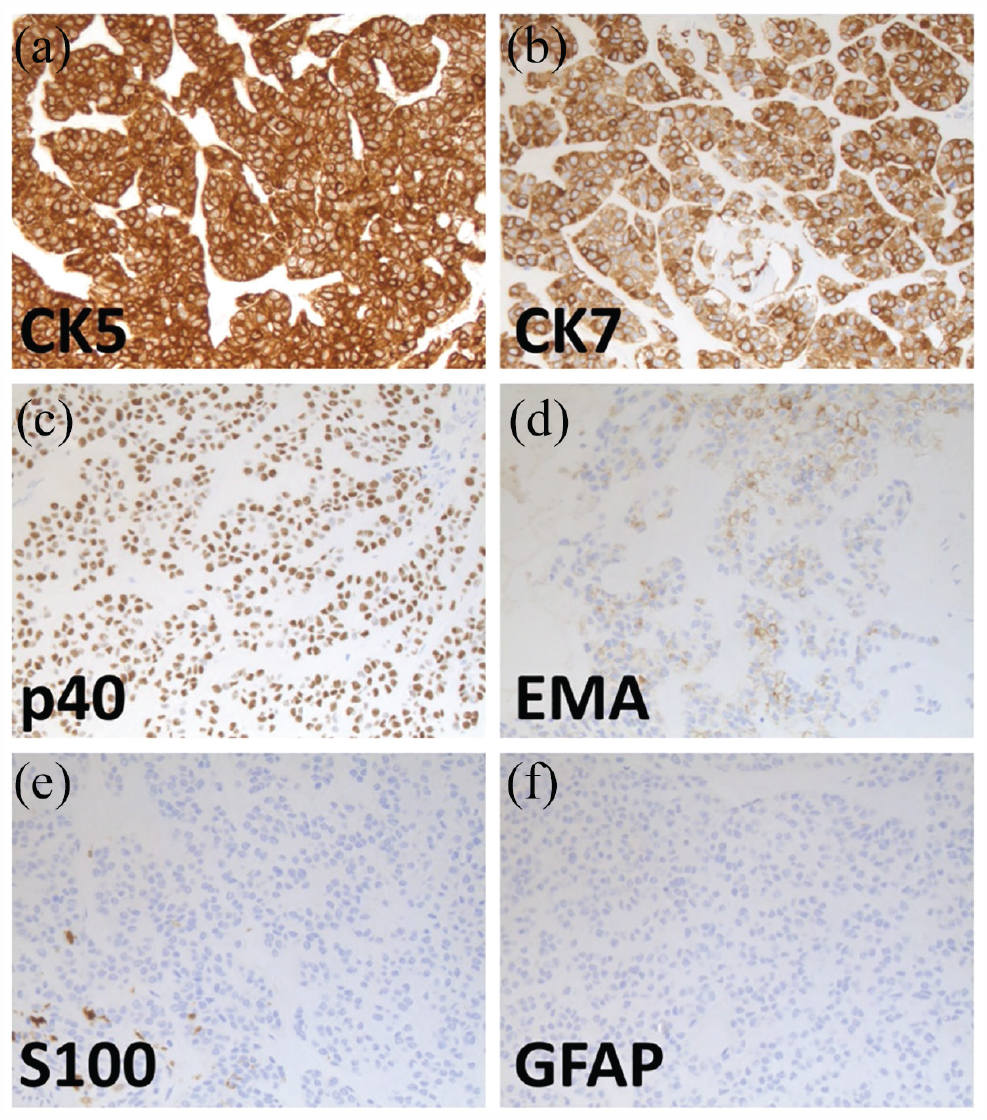
Immunohistochemical results. The tumour cells were diffusely positive for cytokeratin 5 (a), cytokeratin 7 (b) and p40 (c), and focally positive for epithelial membrane antigen (d). The tumour cells were negative for S-100 protein (e); non-neoplastic dendritic cells are positive in this image and glial acidic fibrillary protein (f). Magnification = 20 × (a–f).
Discussion
The most common tumour found in the base of the tongue is squamous cell carcinoma. Approximately 0.5% of tongue base tumours are salivary gland in origin, the most common of which are mucoepidermoid carcinoma, adenocarcinoma not otherwise specified and adenoid cystic carcinoma. HCCC represents 1% of all salivary gland tumours and is only rarely found in the oropharynx.3,5
Here we present a case of HCCC of the base of the tongue in addition to a literature review, using PubMed and Ovid MEDLINE of HCCC originating from base of the tongue. Our review serves as an update to one completed by Watanabe and colleagues in 2015. At that time, they reported a total of 23 cases. As such, the literature review presented spans from 2015 to 2022. We included all case series, case reports and conference abstracts. A total of 13 new cases were reported since 2015, including the case from our institution (Table 1).3,6–12 In total, there are 36 cases reported in literature since 1994. These numbers highlight the rarity of this tumour and resulting challenges in treatment selection.
Summary of the published cases and series of HCCC at the base of the tongue since 2015.

ND: neck dissection; TORS: transoral robotic surgery; RT: radiotherapy; CT RT: chemotherapy radiotherapy; RFFF: radial forearm free flap; LN: lymph node; N/A: not applicable.
Of the 13 new cases found during our literature review, a female preponderance was identified (11/13, 85%), which corresponds to certain literature1,13 but contrasts with review done by Watanabe et al., who found an equal prevalence between males and females (1:1). The mean age in our series is 55 years (range 33-75) which is comparable to what is reported by others in literature.1,6,13 The mean size of the excised tumour is documented to be 2.3 cm (range 1.1-3.9), making our case the largest diameter tumour documented in this series. Progressive dysphagia is the most common symptom on clinical presentation.
Surgical excision is the most common modality of treatment, but with different approaches, including conventional transoral, transoral robotic surgery, mandibulotomy and transcervical. Unfortunately, the majority of the cases do not describe in detail the surgical approach and the associated rationale, and as such, it is hard to draw conclusions on the success or failure of each approach.3,6,7,9–12,14 The mandibulotomy approach was chosen in our case to provide sufficient surgical exposure, to allow for optimal margin control, to achieve adequate haemostasis and to facilitate free tissue reconstruction.
In terms of the neo-adjuvant/adjuvant treatment, one case received chemoradiotherapy preoperatively, 10 two cases received radiotherapy alone and one case received chemoradiotherapy post-operatively.7,9,14 Unfortunately, in the majority of cases primary treatment of the neck was not motioned, however, delayed neck metastasis was confirmed in two cases (15.4%) at 3 years and 9 years, requiring neck dissection and post-operative radiotherapy.10,11 HCCC is reported to have regional metastases in 15.3% of cases and distant metastatic disease in 4.7% of cases.6,15 In our case, a neck dissection was performed (Levels I–III), confirming two metastatic lymph nodes. This tendency for regional metastatic disease highlights the importance of treatment of the neck upfront.
Conclusion
In conclusion, HCCC is a rare salivary gland tumour that is uncommonly found in the base of the tongue. Wide local surgical excision with neck dissection is the preferred treatment approach. Post-operatively, adjuvant radiotherapy can be considered based on the final pathology of the surgical excision to minimize local or regional recurrent disease.
Statement of collaboration of team members
The team members for this project are as follows:
Dr. Fahad Al Zadjali
Dr. Hussain Alsaffar
Dr. Michael Odell
Dr. Jason Wasserman
Angelina Tohmé
Dr. Stephanie Johnson-Obaseki
Footnotes
Acknowledgements
N/A
Author contributions
S.J.O. and F.A.Z. are both Head and Neck oncology surgeons at The Ottawa Hospital. Fahad was the main author for the literature review. They were both responsible for the overall writing of the article. M.O. and H. A. were the main Head and Neck oncology surgeons responsible for the care of the patient in question. These authors contributed the relevant information and details pertaining to the diagnosis, treatment and overall care of the patient. J.W., head and neck pathologist, contributed his expertise by composing the information regarding the pathology of specimens collected and provided the images and descriptions of samples. A.T. is the primary research coordinator for the department of Otolaryngology – Head and Neck Surgery at The Ottawa Hospital. She has extensive clinical research experience. She was involved in the manuscript preparation, formatting, and review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.