
Abstract
Splenic volvulus of wandering spleen is a rare clinical condition. It causes significant morbidity and mortality, especially if undetected. Here, we report a case of 32-year-old female who presented with worsening abdominal pain for 1-week duration. Contrast-enhanced computed tomography scan of the abdomen showed splenic volvulus with infarction and involvement of the pancreatic tail. She underwent exploratory laparotomy and splenectomy with preservation of the pancreatic tail. Patient progressed favourably. Our case report describes a rare clinical entity of a splenic volvulus with a twisted pancreatic tail. This is a life-threatening condition that requires prompt diagnosis and treatment.
Introduction
The spleen is anatomically located in left upper quadrant of the abdomen attached to spleno-renal, gastro splenic and spleno-phrenic ligaments. 1 A wandering spleen is an uncommon condition where the spleen migrates from left upper quadrant to other parts of peritoneal cavity due to congenital or acquired weakness or hypermobility of splenic suspensory ligaments. 2 This condition occurs in less than 0.2% of the population and its more common in females (10:1). 3 Its incidence has two peaks: first in children at the age of 3 months–10 years and second in adults in the age range of 20–40 years. 4 The clinical presentations of wandering spleen vary from asymptomatic to a surgical emergency and may mimic other abdominal pathologies. 5
A splenic volvulus is a rare complication of wondering spleen; in which the spleen twists on its hilum causing torsion on the splenic vasculature. 6 This ultimately results in congestion, infarction or, in a severe case, splenic rupture. Splenic volvulus can present as intermittent, acute or chronic abdominal pain, as the spleen may undergo time to time torsion and detorsion. 7 Laboratory tests are non-specific, however pancytopenia may be present as a manifestation of hypersplenism. 8 Contrast-enhanced computed tomography (CT) scan is useful to evaluate spleen position and vascular integrity. Wandering spleen can be managed with splenopexy, while splenic volvulus with infarction needs splenectomy. 9
Case
We present a case of splenic volvulus of a wandering pelvic spleen in a 32-year-old mother of one child. She was diagnosed with anaemia in her first pregnancy at the age of 26 years. She was detected to have moderately enlarged pelvic spleen at that time. Ultra sound scan abdomen showed a moderately enlarged spleen at this time (17 cm × 8 cm × 6 cm). She has undergone lower segment caesarean section to deliver her baby. She defaulted from the haematology follow-up at the age of 27 years. She presented with intermittent left side colicky pain for 1-week duration associated with anorexia and fever.
Physical examination revealed a fever of 38.3 C, a heart rate of 88 beats per minute, a blood pressure of 100/70 mmHg, and an oxygen saturation of 100% on room air. She appeared in moderate distress from pain, and an abdominal examination revealed a mobile pelvic mass. Laboratory investigation was notable for whole blood count (WBC) 13.44 × 103/μL, haemoglobin 6.5 g/dL, platelets 940 × 103/μL, erythrocyte sedimentation rate (ESR) −37 mm/first hour aspartate transaminase test (AST) 51 U/L, alanine transaminase test (ALT) 83 U/L, amylase 83.3, C- reactive protein (CRP) 143, amylase −83, and total bilirubin 16.4 μmol/L. Electrolyte and renal functions were normal. Her pregnancy test was negative. She was transfused with red cell concentrate to optimize her haemoglobin level. She was started on aspirin due to thrombocytosis. A CT of the abdomen and pelvis was performed, which demonstrated findings consistent with wandering spleen with splenic infarction and rotated mesentery, involving the tail of pancreas, splenic vein and superior mesenteric vein, and its branches suggestive of a whirl sign (Figure 1). She was taken to the operating room for exploratory laparotomy and found to have moderately enlarged pelvic spleen with twisted hilum including tail of the pancreas in the infra colic compartment. Spleen appeared dusky in colour (Figure 2). Detorsion and splenectomy were performed, and the viable tail of pancreas was placed in the supra colic compartment. Size of the spleen was 20 cm × 15 cm × 9 cm and the weight was 3.24 kg. Laparoscopic approach was considered but we proceeded with the open method as the spleen was occupying the centre of the abdomen.
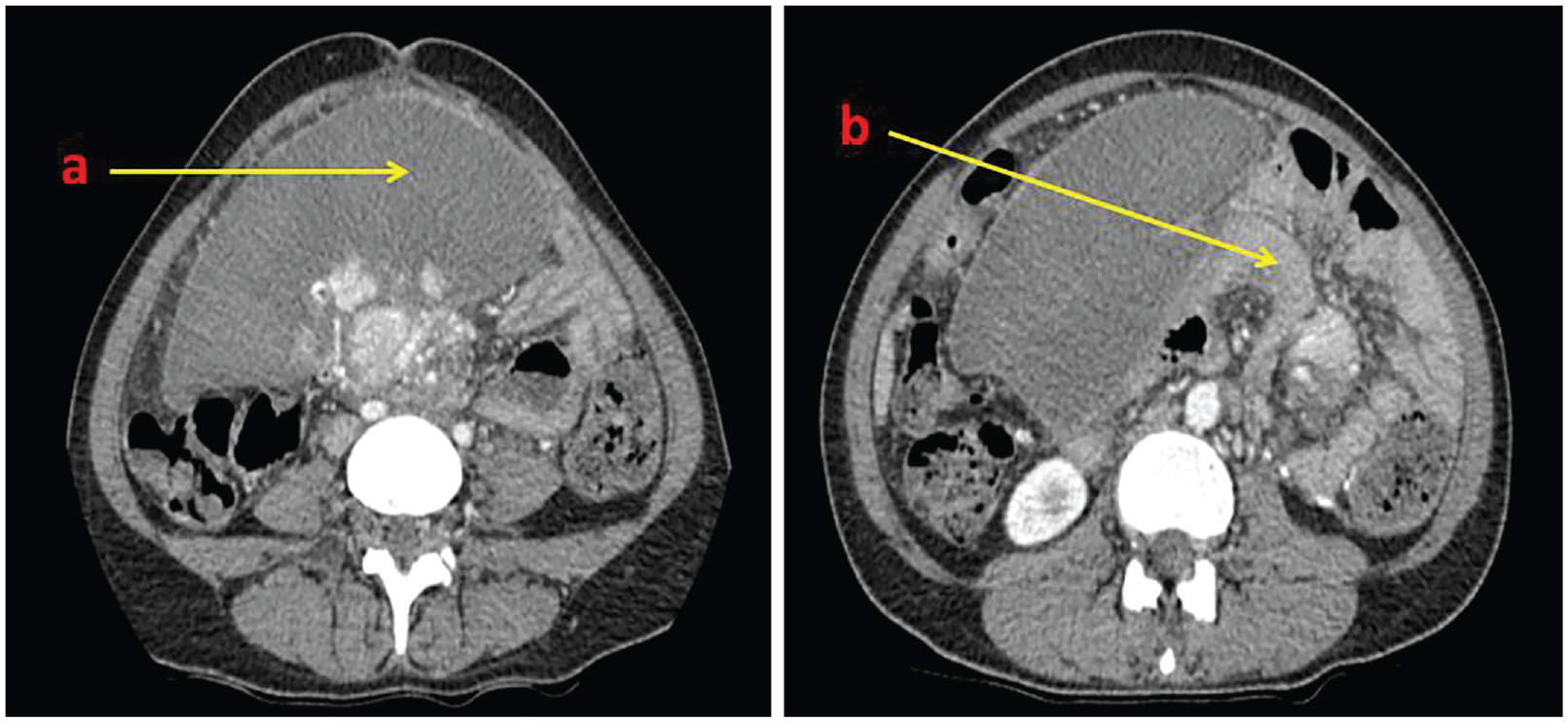
Computed tomography images. (a) Axial image showing moderately enlarged spleen with absent enhancement. (b)Whirl appearance of splenic pedicle, including the pancreatic tail (demonstration of a thickened and coiled vascular pedicle) – pathognomonic finding of torsion.

Intraoperative findings. (a) Infarcted, moderately enlarged pelvic spleen. (b) Splenic volvulus showing torsion of splenic pedicle. (c) Untwisted splenic pedicle along with pancreatic tail. (d) Splenectomy specimen (20 cm × 15 cm × 9 cm).
Her postoperative course was uneventful. Aspirin was omitted when the platelet count reached normal range. Post splenic vaccine prophylaxis was arranged. She was discharged from hospital on postoperative day 5.
Discussion
Wandering spleen is a rare clinical entity that accounts for less than 0.5% of all indications for a splenectomy. 10 This is also known as splenoptosis, ectopic, free-floating, or aberrant spleen. This condition is characterized by a congenital deficiency or acquired laxity of the suspensory ligaments of the spleen. 1 It occurs most commonly in women of the reproductive age group. 4
Our case matches gender and the age of presentation of splenic volvulus (female predominance and age range of 20–40 years). 3 Wandering spleen is related to acquired condition such as splenomegaly, which this patient had for more than 5 years. Acquired form of wandering spleen can happen in conditions that weaken the ligaments such as pregnancy. 5 Wandering spleen may manifest as an abdominal or pelvic mass, chronic intermittent abdominal pain with spontaneous torsion and untwisting. 11 It can present as an acute abdomen in which abdominal pain is the main feature and is associated with nausea, vomiting and fever, indicating volvulus of the wandering spleen favoured. 7 This may mimic intestinal obstruction.
Full blood count reveals thrombocytosis which is attributed to possible splenic infarction compared to thrombocytopenia in splenomegaly described in the literature. 8
Contrast enhanced computed tomography of the abdomen and pelvis is the imaging modality of choice, confirming the diagnosis of splenic volvulus of wandering spleen by showing an empty left upper quadrant with an abdominal or abdominal-pelvic mass reminiscent of the hypodense appearance of the spleen and not taking contrast after intravenous injection. The twisted splenic pedicle demonstrates a whirlpool configuration. 12
When the diagnosis is made, surgical exploration is indicated. In the absence of splenic necrosis, the treatment of choice is splenoplexy, followed by detorsion to fix the spleen in its normal anatomical position. In cases of splenic necrosis, splenectomy is indicated by an open or laparoscopic approach. 13 In our patient, a splenectomy was performed, due to the infarction of the spleen. In our case, the pancreatic tail was twisted, but it was also viable. One case report described associated pancreatitis when pancreatic tail was involved. 14 In our case amylase level was normal and pancreatic tail was viable despite twisting.
Vaccinations should be considered to prevent fulminant infections due to encapsulated germs (post-splenectomy sepsis). 15
The patient is uneventful for 3 months following surgery and is being followed up at our clinic.
Conclusion
Splenic volvulus is an uncommon condition in patients presenting with an acute abdomen. A high degree of suspicion is necessary for the diagnosis of the condition when a known patient with splenomegaly presents with abdominal pain. Previous medical history, examination and early imaging play vital roles in the diagnosis. It has to be diagnosed promptly and surgical intervention is mandatory in most to prevent life-threatening complications and to preserve the spleen if possible.
Footnotes
Acknowledgements
None declared.
Author contribution
All authors were involved in the management of the patient. K.L., S.U.N, G.N., M.R.C and S.K. contributed in acquiring data, literature review, designing the figures and drafting the article. K.W. and M.N. contributed to design and concept of the article, revising it critically for important intellectual content and approval of the final version to be published. All authors have read and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.