
Abstract
Objective:
The aim of this study was to assess HIV screening for prevention of mother-to-child transmission service utilization and associated factors among pregnant women in Hadiya zone, Southern Ethiopia.
Methods:
The study was conducted in a community setting and was cross-sectional with a multistage sampling technique. A total of 613 women were selected randomly from 29 kebeles (the smallest administrative unit next to the district). Data were collected using a standardized interviewer-administered questionnaire. After being coded, reviewed, and entered into Epi-data, the data were exported to SPSS Version 21. Frequencies, percentages, graphs, and means and standard deviations were used to show descriptive data. In bivariate analysis, a p-value of 0.25 was utilized to identify candidate variables for multivariable logistic regression analysis. The statistical significance level was established at 0.05, and the strength of the association was measured using an adjusted odds ratio.
Results:
A total of 613 pregnant women out of 630 who were eligible, were included in our study. Among them, 276 (45%; 95% CI: 41.1–48.8) were tested for HIV. HIV screening was associated with secondary and higher maternal educational level (AOR = 5.01, 95% CI: (3.08–8.16)), number of antenatal care visits four and higher (AOR = 4.25, 95% CI: 2.41–7.51), distance from health facility (AOR = 1.93, 95% CI: 1.24–3.101), and male partner involvement (AOR = 1.88, 95% CI: 1.31–2.69).
Conclusion:
Less than half of the pregnant women included in our study had been tested for HIV; which was quite lower than the national requirement that every pregnant woman be tested during a visit. Only those who had a higher level of education, who regularly took antenatal care, who were not far away from the health facility, and whose partner was involved in antenatal care, were more susceptible to being tested. Thus, actions such as female education and increasing accessibility of the service should be prioritized.
Introduction
Screening is the process of detecting an undiagnosed disease based on the results of tests, examinations, or other treatments that can be performed quickly. 1 Pregnant women, new mothers, their children, and families can receive a wide range of HIV-related prevention, care, treatment, and support services through prevention of mother-to-child transmission (PMTCT). 2
Mother-to-child transmission (MTCT) service programs include preventing HIV infections among women of reproductive age (15–49 years), preventing unwanted pregnancies among HIV-positive women, and providing lifelong antiretroviral therapy (ART) to HIV-positive women to maintain their health and prevent transmission during pregnancy, labour, and breastfeeding. HIV screening for the prevention of HIV transmission from mother to child is the most important intervention point in ensuring that no child is born with HIV (PMTCT).1,3
In 2016, the United Nation Organization for AIDS (UNAIDS) and the President’s Emergency Plan for AIDS Relief (PEPFAR) developed a framework calling for a worldwide spirit to end HIV/AIDS among children, adolescents, and young women. 4 The PMTCT program in Ethiopia was launched in 2001 and implemented the service to reduce HIV epidemics in the general population and specifically in children. According to the WHO Prevention MTCT guideline, it was revised in 2007 and 2012.4,5
Globally, around 1.8 million children <15 years old live with HIV, and 120,000 children died from AIDS-related illnesses in just 1 year. About 95% of these infections are mainly the result of MTCT of HIV during pregnancy, labor, and delivery or during breast feeding. 6
The burden of disease transmission and death varies by region; nearly 75% occurs in Africa alone, with 91% occurring in sub-Saharan Africa and low- and middle-income countries. 7 Ethiopia is one of the countries with a high burden of HIV, with around 66,517 children infected with HIV in 2017, where the main sources of child HIV infections were mostly vertical infections and MTCT. 8 In the absence of therapy, there is a 15%–45% possibility of transferring the virus from mother to child during pregnancy, delivery, and lactation and 50% of all HIV-positive newborns will die before the age of 2 years. 8 However, effective interventions can decrease the risk to below 5%. 9
Ethiopia continues to have a low percentage of pregnant women who undergo HIV tests and pregnant women who test positive for HIV who receive antiretroviral medications (ARVs) for PMTCT. According to the Ethiopian demography and health surveillance (EDHS) report, only 19% of pregnant women received HIV counseling, were tested for HIV, and accepted HIV test results during their antenatal care (ANC) visit. 10 Due to a lack of counseling, only a fraction of them are tested for HIV. Pregnant women are rarely tested for HIV in order to get PMTCT services. Furthermore, HIV transmission from mother to child continues to be a significant problem. Many barriers remain unsolved, especially when it comes to HIV testing and antiretroviral medicine for HIV-positive pregnant women. 11
According to a recently revised strategy for accelerated implementation of the PMTCT program in the “opt-out” strategy, HIV testing should be offered to all women during pregnancy, delivery, and postnatal care (PNC). However, the achievement has been low and lagging behind. 12 Screening of HIV for PMTCT service is one of the important areas that needs to be confirmed for achievement of the sustainable development goals (SDGs) related to health, mainly SDG 3. It is one of the national prevention priority programs of the Federal Ministry of Health (FMOH). The performance of the annual screening of HIV for PMTCT service was 57% in 2017, which is far below the national target of 91% and has decreased by 8% (from 63% to 57%). However, the HIV positivity yield has increased by about 22% compared with 2016. 13 In Southern Nations, Nationalities, and Peoples’ Region (SNNPR), only 17.2% of pregnant women were screened for HIV for PMTCT service during ANC visits, where the performance remains very low as compared with the national standard. 9 In 2010, the EFY Hadiya zone health management information systems (HMIS) report showed that only 42% of pregnant women were screened for HIV for PMTCT during ANC visits. 14 There are a few studies carried out on screening for HIV for PMTCT services in developing countries, particularly in Ethiopia. The studies showed that many barriers were identified relating to screening for HIV for PMCT service.15,16 Some important factors, such as referral linkage for HIV counseling and testing, were not addressed.
As per the investigator’s search, no previous studies were found that specifically focused on HIV screening for PMTCT service utilization in our study area. Therefore, the aim of our study was to determine the prevalence and identify factors associated with HIV screening in pregnant women.
Methods and materials
Study setting and design
A community-based cross-sectional study was undertaken in the Hadiya zone, in southern Ethiopia. It is located 230 km away from Addis Ababa. According to the 2007 European Commission (EC) demographic profile data, the total estimated population of Hadiya is 1.69 million, of which 831,480 (49.2%) are male and 858,520 (50.8%) are female. From the total population, 30,048 (3.5%) are pregnant women. Hadiya zone has 10 districts and 2 town administrations. Regarding health institutions, there is 1 teaching general hospital, 4 primary hospitals, 61 public health centers, and 305 health posts. 14
The study was conducted from 1 March to 1 May 2019.
Participants
All pregnant women who were found in the Hadiya zone were the source population, and those selected women in the selected districts during the data collection period were considered as the study population. Pregnant mothers whose gestational age (GA) was 16 weeks or above in the selected kebeles and who gave consent to participate in the study were included. Pregnant mothers who were severely/critically ill, previously diagnosed mentally ill or unable to communicate verbally during the data collection and who did not volunteer to participate in the study were excluded from the study.
Sample size determination
The sample size was calculated using a single population proportion formula

Where:
n = is the desired sample size;
Zα/2 = was the standard score value for 95% confidence level for two-sided normal distribution which is 1.96;
p = the proportion of HIV testing of PMTCT service utilization among pregnant mothers in Mizan Amen; p = 53.7%; 17
d = 0.05, which is the margin of sampling error.
Thus,

So, n = 382, with a design effect of 1.5, 1.5*382 = 573, then adding 10% non-respondent rate, the final sample size was 630.
Sampling procedure
To select study participants, we have used a multistage sampling technique. At the beginning, 3 districts and 1 town administration were randomly selected from 12 districts and 2 town administrations. In the second stage, we selected 30% of kebeles from selected districts, and after that, the total sample size was proportionally allocated to those selected kebeles. A list of pregnant women was obtained from updated family folders and registration books in the health posts of the selected kebeles and then a sampling frame was prepared. There were 1829 registered mothers in those randomly selected three districts and one town administration. Finally, a systematic random sampling method was used to get mothers by calculating the interval 1829/630 = 2.9 (since it is proportionally allocated, the interval was approximately three in every kebele). The first mother was selected randomly among the first three mothers, and then every third mother was selected systematically from the frame till we got the sample size (Figure 1).
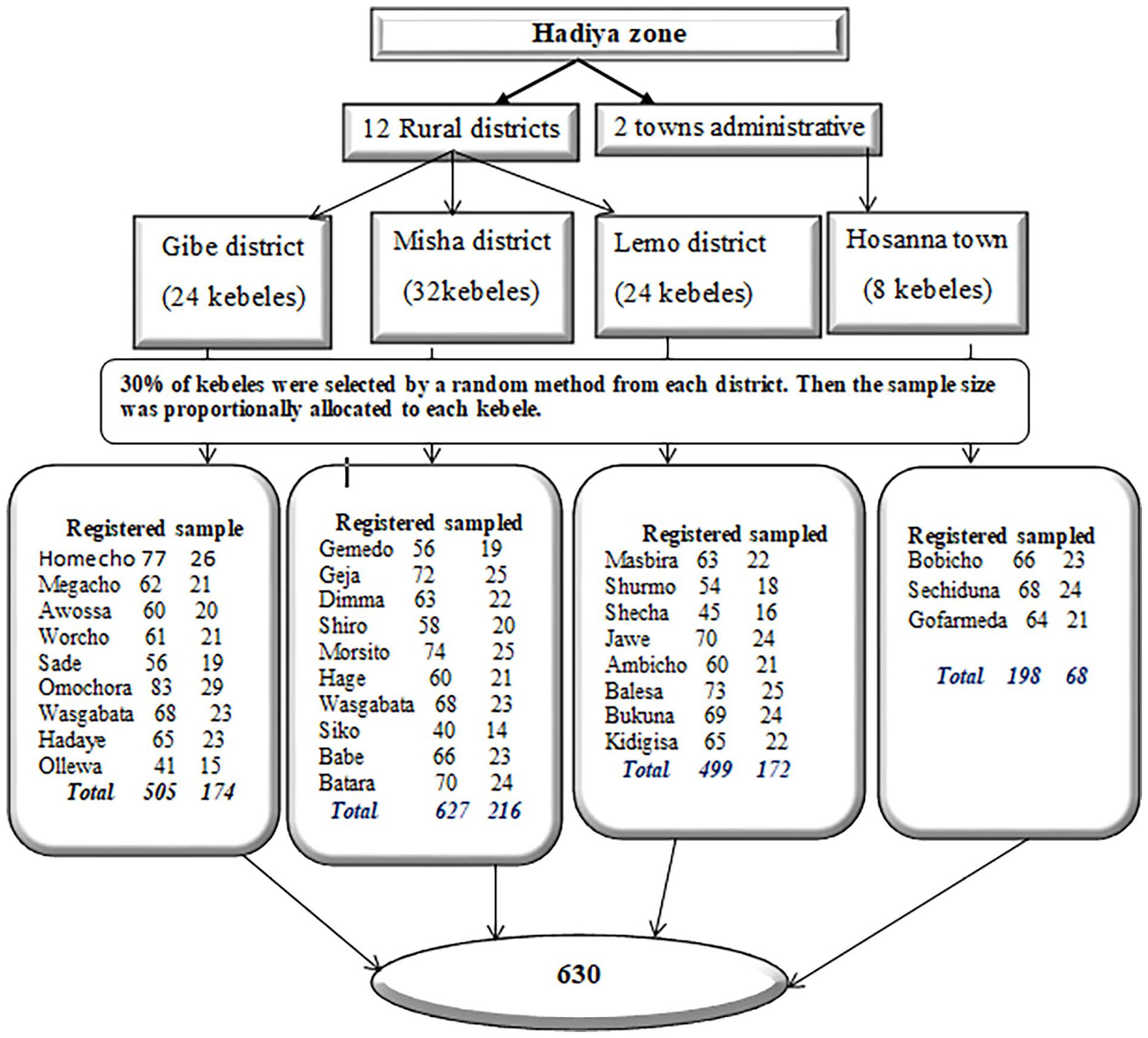
Schematic representation of the sampling procedure for HIV screening and associated factors among pregnant women.
Study variables
Dependent variable
Screening of HIV for PMTCT service utilization.
Independent variables
Sociodemography characteristics, number of ANC visits, place of last, delivery, number of gravidity, GA, fear of stigma and discrimination, partner disclosure, male partner involvement, knowledge, accessibility and distance, privacy and confidentially, source of information, and waiting time.
Operational definition
PMTCT of HIV service
A service that is received by pregnant mothers in health facilities like counseling, testing, and receiving test results for prevention of MTCT of HIV/AIDS. 1
Screening of HIV for PMTCT service utilization
Screening of HIV for PMTCT service utilization was measured by participants’ responses that reported being counseled, tested, and taking the test result for the HIV test.4,17
ANC visits
ANC, which is having a health institution visit for a pregnancy check-up by a skilled health professional during pregnancy, is categorized into four: first ANC visits; second ANC visits; third ANC visits; and fourth and above ANC visits. 18
The distance from the health facility
Mothers who live within a distance of 60 min on foot from the nearest health institution were considered as geographically accessible, and more than 60 min were considered as not accessible. 17
Male partner involvement
The level of partner involvement in the screening of HIV for the PMTCT program was measured using six yes-or-no type questions. A total score of four to six was considered as a high level of male partner involvement, and less than three was considered as low partner involvement. 19
Knowledge about the PMTCT service
It was measured by the participants’ responses to 10 knowledge-related yes or no and multiple-choice type questions related to MTCT. Correct responses were given a value of “1” and incorrect responses were given a value of “0.” Then those who scored 60% and above have good knowledge, while those who scored less than 60% have poor knowledge. 20
Data collection tools
Data were collected by using a structured interviewer-administered questionnaire adapted from the UNAIDS 2015 best practice collection tool. 21 The indicators for the wealth index were adapted from EDHS. 10
Data collection procedures
Before actual data collection, a list of pregnant women (a sampling frame) was obtained from each selected kebeles health post. One-day training was given for 10 data collectors and 4 supervisors regarding the data collection instruments one by one, ethical considerations, and objectives of the study in each district. The data collectors were guided by local volunteers to get the selected mothers’ houses. The data collection procedure was supervised by four BSc public health officers.
Data quality management
Data quality was assured before, during, and after the data collection process.
Before data collection
To ensure consistency, data collection tools were translated from English to Hadiyisa and back to English, and a pretest was conducted in Soro district on 10% of the total sample size (outside of the study area). The clarity, consistency, and completeness of the questionnaire were all reviewed. On the basis of the pretest results, significant changes were made, and the logical flow of ideas was maintained. In addition, data collectors and supervisors received training.
During data collection
The data collection method was closely monitored on a daily basis. Every day, the supervisors and main investigator examined the collected data for completeness and consistency.
After data collection
Before transferring it into computer software, the supervisors and the primary investigator double-checked the accuracy and consistency. Each question was given a nonoverlapping numerical code, and the coded data was entered into Epi-data.
Statistical analysis
The data were checked for completeness and accuracy before being coded and entered into Epi-data. It was cleaned and adjusted as necessary before being exported to SPSS version 21.
Principal component analysis (PCA) was used for socioeconomic factors used in determining a household’s wealth level. To execute data reduction, the PCA assumptions were tested. To conduct factor analysis, Bartlett’s test of sphericity was checked and found to be significant at p = 0.05. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was used to assess the sample adequacy for PCA, and the results were approved if it was >0.5. Varimax rotation is used during factor extraction to reduce item cross-loading across many factors.
To assess the distribution and describe the research population in respect to key factors, descriptive statistics like frequencies, proportions, and graphs were utilized. Cross-tabulation was also used to see how different variables were distributed with respect to the outcome variable. After checking the chi-square assumption and using logistic regression to identify candidate variables for multivariable analysis, bivariate analysis has been performed. Variables having a p-value of less than 0.25 in bivariate analysis were selected as candidates for multiple logistic regressions, which were then entered into a multivariable logistic regression model to find the most relevant determinants. In the final model, a p-value of 0.05 was used to demonstrate the statistical significance, and an adjusted odds ratio with a 95% confidence interval was used to assess the strength of the association. The goodness-of-fit of the model was checked by Hosmer and Lemeshow. It was a nonsignificant 0.544, which means a good fit.
Result
Sociodemographic characteristics of participants
This study had a response rate of 97%, with 613 pregnant mothers participating. Mothers ranged in age from 15 to 49 years, with a mean of 28.28 years and a standard deviation of 5.28. The majority of those who took part in the survey were married (504 or 82.2%) and Protestants (459 or 74.9%). The majority of the women (537, 87.6%) were housewives, and 277 (45.2%) had only an elementary education (Table 1).
Sociodemographic characteristics of pregnant women interviewed (N = 613) in Hadiya zone, south Ethiopia, May 2019.

Catholic, Adventist Seventh day.
Silte, Amhara.
Private employee, students.
Obstetric and related characteristics
When it came to the total number of pregnancies, 455 (74.2%) of them, including the current one, were multi-gravida. Furthermore, the majority (306, 67.3%) of pregnant women with multiple pregnancies had delivered their previous pregnancy at a health facility. Almost half of the pregnancies (48.1%) were in the second trimester, and 176 (28.7%) had four or more ANC visits (Table 2).
Obstetric and related characteristics of pregnant women (N = 613) in Hadiya, south Ethiopia, May 2019.

ANC: antenatal care.
Access to health information and health service characteristics
A total of 193 mothers walked for less than 30 min. Regarding the source of information, 294 (48%) of the participants got information from mass media such as radio and TV, and 319 (52%) of the participants got it from health extension workers. Concerning the average waiting time to see providers, 138 (22.5%) of the respondents reported a short time to get providers, 196 (32% of respondents reported the right time) and 279 (45.5%) reported a long time to get providers.
Individual related factors
Pregnant women’s knowledge of MTCT for HIV/AIDS
Based on these findings, 393 (64.1%) pregnant mothers were knowledgeable, and 220 (35.9%) had poor knowledge.
Referral linkage, male partner involvement, fear of stigma and discrimination related to HIV
From the total number of respondents that have participated in this study, about 401 (65.4%) of the pregnant women had follow-up ANC at the health post. Of 401 participants who had follow-up ANC in health post, 210 (52.4%) were referred to a health center/hospital for PMTCT of HIV/AIDS services. Fear of HIV stigma and discrimination was the reason for 332 (54.2%) of participants’ fears of HIV testing and disclosure of results to a partner or family member, and 47.6% of respondents disclosed to their partner or family member (Table 3).
Referral linkage, knowledge, fear stigma, and discrimination related to HIV of pregnant women about PMTCT of HIV/AIDS service, south Ethiopia, May 2019.
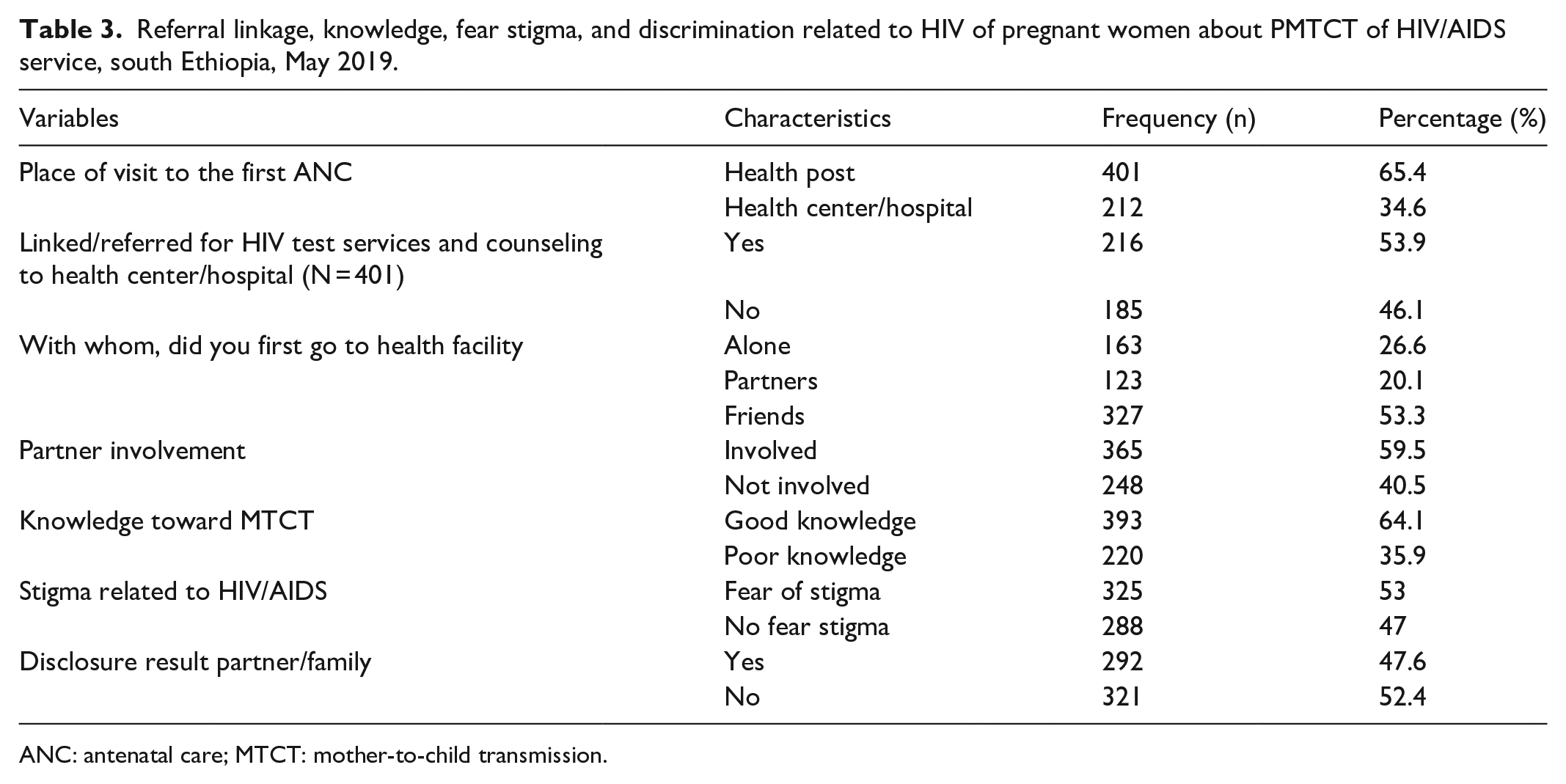
ANC: antenatal care; MTCT: mother-to-child transmission.
Screening of HIV for PMTCT of HIV service utilization among pregnant women
The prevalence of HIV screening for PMTCT service utilization among pregnant women was found to be 276 (45%) with a 95% CI of 41.1–48.8. From the total number of respondents, 479 (78.1%) of women offered counseling for HIV testing, and 276 (45%) were tested. And of those who received their test results, 98.5% were negative. From the total number of pregnant women who had received their results only, 1.5% (n = 4) were found to be positive. And those pregnant women who were found positive, all of them began to use ARV drugs for the purpose of PMTCT. Those who had not tested during their current pregnancy stated that the main reasons were that they did not believe they were at risk for HIV, that they did not want to discuss it with their partner/family, that there was a lack of service, that they were afraid of stigma and discrimination, and that they were afraid of the HIV test (Figure 2).

Reasons for not receiving HIV during pregnancy among Hadiya zone Hadiya southern Ethiopia.
Factors associated with HIV screening for PMTCT service use among pregnant women (bivariate analysis)
In bivariate analysis, residence, maternal educational status, occupation of mothers, husband’s occupation, marital status of mothers, house wealth index status, number of pregnancies, number of ANC visits, GA, distance from health facility, source of information from mass media, from wealth workers, referral linkage, waiting time, privacy kept during ANC, male partner involvement, knowledge toward PMTCT, fear of stigma, place of first ANC visits, and disclosure for partner were all analyzed.
In a bivariate analysis, mothers’ educational status, marital status, GA, number of ANC visits, distance from health facility, male partner involvement, and privacy during ANC visits and testing were chosen as candidate variables associated with HIV screening for PMTCT service at p-value = 0.25 in a bivariate analysis.
Multivariable analysis for factors affecting screening of HIV for PMTCT service utilization among pregnant mothers
The multivariate analysis revealed that pregnant women with a secondary education or higher were 5 times more likely to be screened for HIV for PMTCT services than pregnant women with no formal education (AOR = 5.01, 95% CI; (3.08–8.16)). According to ANC visits in current pregnancy, pregnant women who had four or more visits were 4.25 times more likely to be screened for HIV for PMTCT service (AOR = 4.25, 95% CI: (2.41–7.51)) as compared with those pregnant women who had visited once. Concerning distance, pregnant women with less than a 60-min distance to a health facility on foot were 1.93 times more likely to be screened for HIV for PMTCT service utilization (AOR = 1.93, 95% CI: 1.24–3.01) than their counterparts. Finally, pregnant women who had a male partner involved in ANC were 1.88 times more likely to be screened for HIV for PMTCT service utilization (AOR = 1.88, 95% CI: 1.31–2.69) than those who did not have a male partner involved in PMTCT (Table 4).
A multivariable logistic regression analysis of factors associated with HIV screening for PMTCT service utilization among pregnant women in Hadiya zone, southern Ethiopia, in 2019 (N = 613).

PMTCT: prevention of mother-to-child transmission; ANC: antenatal care; AOR: adjusted odds ratio; COR: crude odds ratio.
Reference category, model fitness (Hosmer and Lemeshow significance test = 0.544), classification power = 66.7 (overall prediction of model was 66.7%).
Discussion
In this study, it was found that only 45% of pregnant women screened for HIV for PMTCT service in their current pregnancy. This finding was lower when compared with the national recommendation set of national PMTCT guidelines, which recommends that every pregnant woman during an ANC visit should be tested for HIV for PMTCT service. 8 Also, this finding was lower than studies conducted in Sebeta (86.9%), 22 Adema (70.1%), 23 Bahir Dar (61.3%), 24 and Mizan Amen (53.7%). 16 The possible reason for the difference between the findings might be due to differences in the methodology; this current study considered pregnant women from community-based and systematic sampling methods, whereas the mentioned studies considered ANC attendant mothers from health facilities and used convenient sampling techniques. Another possible reason might be the shortage of access to health services in study settings compared with the mentioned study settings. In addition, this finding is also lower than studies conducted in Uganda (85.5%). 25 The difference might be due to the socioeconomical differences, whereas this finding is higher when compared with the findings of the studies conducted in South Gonder (9.7%). 26 This discrepancy is due to the time gap between this study and the abovementioned study. As time increases, the awareness of people also increases due to the accessibility and availability of healthcare facilities. Another possible reason due to sociodemographic differences is that this study was conducted in both rural and urban settings, whereas the study conducted in South Gonder was only rural. Furthermore, this result was greater than the 19% found in the EDHS report from 2016. 10 The discrepancy could be due to EDHS including more remote areas than this study area.
Different factors were identified as significantly associated with the screening of HIV for PMTCT service. It was observed from the current study that pregnant women who had education status of secondary and above education (9–12)+ were 5 times more likely to be tested for HIV for PMTCT services as compared with those who had no formal education, and maternal educational level who had primary (1–8) levels were 1.79 times more likely to be tested for HIV for PMTCT services than mothers who had no formal education. This finding is supported by a finding from a study conducted in the Afar region, in which women who could read and write were 11 times more likely to be screened for HIV for PMTCT service than those who could not read and write. 27 Also, this finding is in line with findings from a study conducted in Wollega zone; pregnant women who had formal schooling were 6 times more likely to be screened for HIV for PMTCT service when compared with those who had no formal schooling. Likewise, a study done in Bahir Dara revealed that more than diploma-educated mothers were 1.43 times more screened for HIV for PMTCT service than those less than the diploma. 24 This finding also supports a study conducted in Kenya, where a mother who had an educational level of secondary or above was 1.4 times more likely to be screened for HIV for PMTCT service than those who had no formal education. 28 This could be because as mothers’ education levels rise, so does their health literacy, and mothers know what is right and beneficial for them. This may also result in the mothers’ increased decision-making power and enable them to better knowledge and better understanding of the benefits of HIV testing.
In the current study, pregnant women who visited health facilities for ANC 4 or more times during their current pregnancy were 4.25 times more likely to be HIV tested for PMTCT services when compared with those who visited once. This finding is consistent with a study in Gonder that showed a mother who had visited a health facility for ANC 2 or more times was 2.64 times more likely to be screened for HIV for PMTCT service than a mother who had visited once. 26 This could be because pregnant women who had more contact with health facilities were more aware of how to use services. Another study done in Adema indicated that a pregnant woman who had more than two visits was 2.59 times more likely to be screened for HIV for PMTCT service than a woman who had visited once. 23 Pregnant women who have more ANC visits are more likely to be checked for HIV and receive PMTCT services. Furthermore, a study conducted in Hawassa found that a mother who had four or more visits to a health facility was 1.04 times more likely to be tested for HIV for PMTCT service as compared with those who had only one visit. 29 This is because as the frequency of ANC visits grew, clients were more likely to get complete HIV education and to be concerned about their children’s and own health.
This study illustrates that pregnant women whose nearest health facility was less than 60 min away from their home were 1.93 times more likely to be screened for HIV for PMTCT service compared with mothers who had a distance of more than 60 min. This finding is supported by the finding of a study conducted in the Afar region that indicated that mothers who were nearest to health facilities were 6.5 times more likely to be screened for HIV for PMTCT service than their counterparts. 27 Another similar study done in Ethiopia applying a count regression showed that an increase in walking distance from a health facility would decrease the screening of HIV for PMTCT service 30 This might be due to having better access during ANC to PMTCT services, better education, information, and awareness about the PMTCT service.
Finally, this study showed that respondents who had high male partner involvement during ANC were 1.88 times more likely to be screened for HIV for PMTCT service when compared with those who had less male involvement. This finding is also consistent with the research conducted in Cameroon, where male partner involvement exceeds PMTCT service utilization by 16.8%. 31 The findings of studies conducted in Wollega zone, Ethiopia, where people were 4.5 times more likely to be screened for HIV for PMTCT services than those who were not involved, 32 and a study conducted in Bahir Dar indicated that involvement of a male partner has a significant association with women’s acceptance of voluntary HIV counseling and testing, which was 2.76 times more likely to be screened for HIV for PMTCT service when compared with pregnant women who had a male partner not involved. 24 This might be because if there is male partner engagement, it improves free HIV testing communication and boosts couples’ disclosure communication.
Strength of the study
It was a community-based study that included both urban and rural populations and used the largest possible representative sample size, which was crucial for generalization.
Limitations of the study
There might be recall bias since the study was asking about past experiences like counseling offered or not during HIV testing, male partner involvement, and others. In order to minimize this, data collectors trained very well on interview questions and gave enough time to remember past memories.
It might also be affected by social desirability bias. But, in order to minimize it, the data collectors were recruited from facilities that were not from the study area, and they assured the participants that they would not take any personal information and that the aim of the study was only for service improvement.
Conclusion
The magnitude of HIV testing among pregnant women in the study setting was 45%, which was lower coverage when compared with the national recommendation that every pregnant woman during an ANC visit should get HIV testing. In this study, male partner engagement, educational status (primary or above), number of ANC visits, and distance less than 60 min from the health facility were all found to be substantially linked with HIV testing for PMTCT. The government should ensure accessibility of services in the community by making them closer, female education, and enabling health extension workers by training and encouraging them to promote PMTCT services.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221127876 – Supplemental material for Prevention of mother-to-child transmission screening among pregnant women in southern Ethiopia from the perspective of the current WHO recommendation
Supplemental material, sj-docx-1-smo-10.1177_20503121221127876 for Prevention of mother-to-child transmission screening among pregnant women in southern Ethiopia from the perspective of the current WHO recommendation by Abebe Dune, Mulugeta Hailu Rad and Habtamu Wude in SAGE Open Medicine
Footnotes
Acknowledgements
The authors give special thanks to the data collectors, supervisors, study participants, and the Gibe district health office. They also thank Jimma University.
Authors’ contributions
M.H.R. and H.W. revised the paper from proposal formulation to manuscript production, and A.D. made important contributions to its conceptualization, data collection, analysis, and interpretation. The final version of the manuscript was read and approved by all the authors.
Availability of data and materials
The dataset used during the current study is available from the corresponding author on reasonable request at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance to conduct this study was obtained from the Institutional Review Board of Jimma University with the approval ID JU/023/12.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Prior to the interview, all study participants were informed of the study’s aim and their right to refuse or withdraw from the interview at any moment if they wanted to stop. Written and signed voluntary consent was obtained from all study participants or legally authorized representatives of minor participants prior to the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.