
Abstract
The prevalence of patent foramen ovale is approximately 20% in the global population. In patients under the age of 55 years, it has been proven as a cause of acute ischemic embolic stroke of otherwise undetermined source. We present a case of a 25-year-old patient who experienced an acute stroke of dominant hemisphere due to internal carotid artery occlusion.The patient underwent mechanical thrombectomy, followed by acute intracranial stenting due to persistent subocclusion of internal carotid artery. Further diagnostic investigations revealed a significant patent foramen ovale. During subsequent follow-up periods, the patient encountered multiple transient ischemic attacks despite receiving antithrombotic therapy. The indicated angiography examination revealed in-stent stenosis and thrombosis, which were resolved after optimal medical treatment. Following patent foramen ovale closure, the patient remained free from further neurological events during the subsequent two-year follow-up periods. This case emphasizes the necessity of comprehensive diagnostic evaluations in young individuals with stroke and underscores the importance of prudent slection of medical therapies.
Introduction
The prevalence of asymptomatic patent foramen ovale (PFO) is approximately 20% in the general human population. 1 However, in young patients who have experienced a stroke, the prevalence of PFO can be as high as 50%. 2 After a comprehensive diagnostic workup of an acute ischemic stroke, the presence of a PFO may strongly indicate a causal relationship with the stroke’s thromboembolic etiology, as a PFO may always be a possible cause of embolic stroke. Therefore, the closure of a PFO has been proved effective in reducing the risk of further embolic events. Additionally, the occurrence of right-to-left shunting (RLS) further increases the risk of stroke and has been found in a larger proportion of stroke patients. 1
The first-line therapy in acute ischemic stroke caused by intracranial large vessel occlusion is stent-retriever thrombectomy, which has an average recanalization rate exceeding 80%. 3 However, acute intracranial stenting, despite achieving successful recanalization, poses an increased risk of complications. These complications include restenosis, in-stent thrombosis, distal embolization, and intravascular stent migration, all of which significantly impact the final functional outcome.4,5 Restenosis, in particular, is the most common complication, occurring in 14.7% of the reviewed procedures. 4 Additionally, symptomatic intracerebral hemorrhage is a feared complication associated with standard antiaggregation therapy during intracranial stent placement, with a rate of 7.7%.3,6
We present a case of a young female patient who suffered a PFO-mediated ischemic stroke. She was treated acutely with thrombectomy and acute stenting of a cerebral artery and subsequently with PFO closure after having suffered another ischemic event, thought to be due to in-stent restenosis with associated thrombosis.
Case presentation
A 25-year-old woman, who had a history of smoking, was urgently admitted to our Neurological Intensive Care Unit due to the sudden onset of right-sided hemiparesis and severe dysphasia. The only notable finding during the physical examination was increased blood-pressure values (140/105 mmHg). Emergency imaging, including CT, MRI, and multislice computed tomography angiography, ruled out intracranial hemorrhage and confirmed an ischemic stroke in the left anterior choroidal artery region (affecting the left hippocampus and the posterior limb of the left capsula interna). Urgent invasive angiography confirmed the occlusion of the left internal carotid artery (LICA) and thrombectomy was performed. Despite successful thrombus aspiration, residual stenosis was observed in the intracranial segment of the LICA, leading to non-patency in the early postprocedural angiogram. As a result, acute intracranial stenting (Neuroform Atlas Nitinol stent, 3 × 15 mm) of the LICA was performed. Subsequent imaging confirmed the previously diagnosed ischemic lesion (Figure 1). Further diagnostic workup, including a 24-h Holter-ECG (DR400 NorthEast Monitoring inc.) and venous Doppler ultrasound exam, revealed no aberrant heart rhythms or signs of thrombosis, respectively. However, transesophageal echocardiography revealed a large PFO with significant RLS and intracranial embolism. Antithrombotic therapy was initiated, and the patient received dual antiaggregation therapy in the early postprocedural period, which was later replaced by dabigatran and ticagrelor. Early physical therapy was initiated and maintained throughout the patient’s hospital stay. The patient exhibited significant regression of the neurological deficit, with residual right-side hemiparesis, and was subsequently discharged to a rehabilitation center. The patient’s late National Institute of Health Stroke Scale (NIHSS) was recorded as 5, while the early modified Rankin scale (mRS) was 2.

MRI of the brain showing acute ischemic stroke in the left anterior choroidal artery region (a), as occluson of left carotid internal artery was confirmed, thrombectomy was performend, however, even after two attempts only partial recanalization was achieved with residual subocclusive stenosis (arrow) and insufficient anterograde flow (b). The last picture (c) showing the end—result after thrombectomy and urgent intracranial stenting of left carotid internal artery.
Three months later, the patient presented once again to the emergency department due to prolonged speech difficulties, dyslexia, dysgraphia, progressive right-hand weakness, and a persistent diffuse headache that had been ongoing for 2 days. Neurological examination revealed subtle motor dysphasia, drooping corner of the lip, right-side spastic hemiparesis (right arm manual muscle testing [MMT] 3/5, right leg MMT 4/5), spastic gait, and right-side hemihypesthesia, resulting in a calculated NIHSS of 7. Additionally, an elevated blood pressure of 160/106 mmHg was noted. Emergency MSCT revealed the presence of two new hypodense zones with loss of differentiation in the territory supplied by the left cerebral medial artery (ACM).
An urgent angiogram was performed, demonstrating restenosis in the distal segments of the stent (extending up to the M1 segment of the left ACM) as well as the formation of a thrombus at the distal edge of the stent (Figure 2). Considering these findings, an aggressive medical approach was deemed optimal. Dabigatran was discontinued, and the patient received intravenous antiaggregation treatment with eptifibatide for 24 h, followed by a switch to dual antiplatelet therapy (DAPT). A comprehensive hematologic evaluation ruled out hereditary thrombophilia and acquired prothrombotic conditions. The patient was discharged from the facility after 7 days, with a regression of the neurological deficit to its prior state.
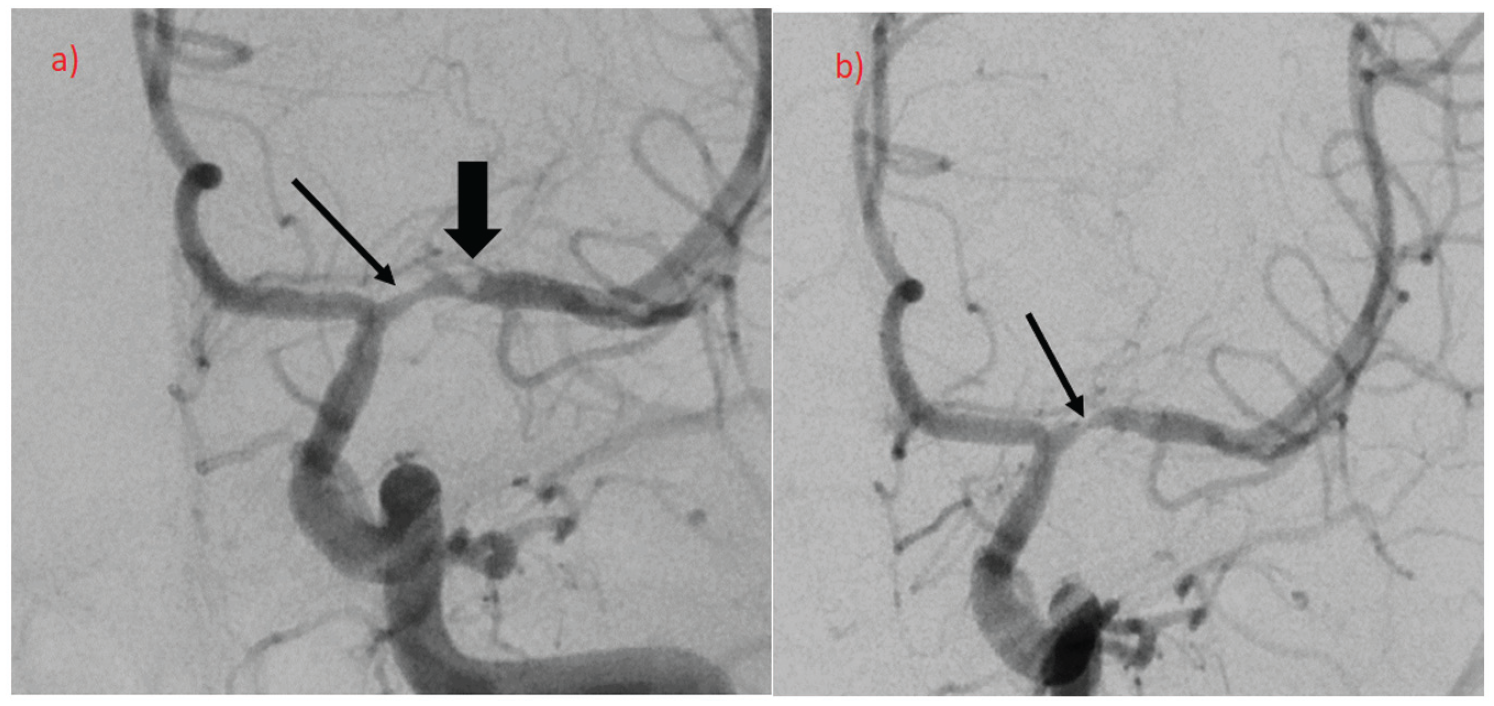
Urgent angiogram showed in-stent restenosis in its distal parts (reaching the M1 segment of left middle cerebral artery—thin arrow) as well as thrombus formation of the distal edge of the stent, with attenuation of distal blood flow (thick arrow, picture a). Control angiography (picture b) showing only residual stenosis (thin arrow) after thrombus resolution.
Six months after the initial stroke, a planned attempt at PFO closure was made. However, the first procedure was unsuccessful, and the patient was advised to continue with her prescribed medication. Subsequent 12-month follow-up assessments did not reveal any further clinical deterioration. One year after the initial attempt, a second intervention was performed at the same Cardiology clinic. The preprocedural cardiological assessment did not identify any pathological findings. The procedure was conducted via the right femoral vein, utilizing an MP catheter to pass through the PFO, and an Amplatz wire was guided into the left upper pulmonary vein. Subsequently, an Amplatzer 25 mm Talisman PFO occluder (Abbott) was carefully positioned over the defect with the assistance of a guidewire and confirmed to be in an optimal position through echocardiographic imaging. The intervention proceeded without any complications. The patient was advised to continue her prescribed medication, particularly aspirin, indefinitely and scheduled for additional echocardiography follow-ups. Subsequent follow-up examinations remained uneventful during the 2-year period of regular checkups.
Discussion
Although the relationship between PFO and cryptogenic strokes has been established in several studies, it remains somewhat unclear.1,7 Cryptogenic strokes account for 15%–40% of all strokes, while PFO is found in 40%–56% of young cryptogenic stroke patients.2,7 In a large meta-analysis of case-control studies, the odds ratio for stroke in patients below 55 years of age with the PFO was reported to be 3.1. 8
In the case of our patient, extensive investigations have excluded other possible causes of stroke. Transcranial Doppler examination demonstrated RLS after a “Valsalva maneuver,” strongly suggesting a cardioembolic stroke.9,10 Therefore, anticoagulant therapy for secondary prevention was deemed appropriate. 11 The patient provided informed consent for off-label use of dabigatran and concomitant consideration of PFO closure. As the patient underwent urgent intracranial stenting during thrombectomy for revealed intracranial subocclusive stenosis, antiplatelet therapy had to be introduced simultaneously, with ticagrelor being chosen. 12 It has less known possible resistance than clopidogrel (5%–44% clopidogrel nonresponders across various studies). 13
The etiology of the verified intracranial stenosis remained uncertain. Although atherosclerotic intracranial artery stenosis could be considered, the absence of involvement of other intracranial blood vessels made atherosclerosis less likely. 14 Artery dissection, another common cause of ischemic stroke in young adults, was ruled out based on the absence of characteristic morphological features. The possibility of a congenital localized stenosis of LICA was raised, but not confirmed. Such isolated intracranial large vessel stenosis without an identifiable cause is extremely rare and requires specific interventional and therapeutic approaches.
Symptomatic intracranial artery stenosis is the most common cause of stroke worldwide, and can be treated through medical, surgical, or endovascular strategies. 15 The VISSIT and the SAMMPRIS trials have both compared the efficacy and the success rate of angioplasty with stenting and aggressive medical therapy. They have shown that endovascular intervention does not provide additional benefits.4,7,16 However, endovascular treatment can be considered for patients unresponsive to medical therapy, yielding a 95.7% success rate and low reocclusion rates (14.7%). 4 In our patient, intracranial acute stenting was indicated due to localized intracranial stenosis of the LICA, and antiplatelet therapy was initiated for 3 months, as sole thrombectomy could not achieve sufficient blood flow in the stenotic vessel. Complications arose after 14 weeks from the procedure, with stent restenosis, thrombosis, and distal embolization occurring 2 weeks after discontinuing ticagrelor. Apparently, anticoagulation therapy was not sufficient to prevent thrombotic events in the attenuated blood flow through the stent. By introducing DAPT and ceasing anticoagulation therapy, the thrombus resolved while maintaining stent patency.
Considering the etiology of stroke in our patient, the intracranial stenosis may have played a more significant role than PFO itself, highlighting the importance of considering both factors in the choice and exclusion of antithrombotic therapy. Following PFO closure, and the continuation of antiplatelet therapy, the patient remained clinically stable without further complications during the two-year follow-up period.
Conclusion
Acute ischemic stroke (AIS) is a relatively uncommon occurrence in young patients and its etiology necessitates meticulous investigation to establish accurate secondary prevention strategies. PFO may serve as a potential etiological factor for cardioembolic strokes in this particular patient population; however, this possibility should only be entertained after ruling out all other potential causes. In our presented case, the patient underwent confirmation of a significant PFO and embolic events via transcranial doppler (TCD) detection, which appeared to be the sole attributable factor for the stroke episode. Despite the presence of the PFO, the concurrent occurrence of intracranial focal stenosis in large blood vessels necessitated an urgent intracranial stenting, along with a temporary regimen of combined antiplatelet and anticoagulation therapy. Following the closure of the PFO, long-term antiplatelet therapy, specifically acetylsalicylic acid, was continued. This case serves to exemplify the imperative for a comprehensive and meticulous diagnostic approach as well as a judicious selection of treatment modalities, in young patients presenting with a dual pathology.
Footnotes
Acknowledgements
We would like to thank our colleagues from the intervention neuroradiology department for providing us with graphical materials, the featured patient for her consent for inclusion of transpired events into our case report, and Miščin E., PhD in Linguistics, University of Zagreb, Faculty of Medicine, for language assistance.
Author contributions
D. Š. wrote the article with the support of Z. P.; J. L. analyzed the data, contributed to the interpretation of the medical data and to discussion; D. O. supplied and interpreted neuroimaging data; I. P. collected and contributed to the interpretation of the medical data; N. B. collected and contributed to the interpretation of the medical data; Z. P. supervised the writing of the article, interpretated the medical data, and discussed the results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This case report was approved for publishing by the University Clinical Hospital Zagreb Ethical Board.
Informed consent
Written informed consent was obtained from the patient(s) for the publication of their anonymized information in this article.