
Abstract
Enterolithiasis or intestinal stones are uncommonly reported. Enterostasis is the cause of stone formation mainly secondary to tuberculous strictures. Although it is unusual, enteroliths can cause intestinal obstruction. We report a case of a mechanical partial intestinal obstruction in a patient with ulcerative colitis previously treated with total colectomy, with the rare diagnosis of multiple primary enterolithiasis.
Keywords
Introduction
Enterolithiasis is a rare cause of small bowel obstruction (SBO). It is classified into primary and secondary types, with primary enteroliths being formed within the bowel and secondary ones originating from outside the bowel. 1 Enterostasis, either due to stricture formation (intestinal tuberculosis, Crohn’s disease (CD), intestinal tumors, incarcerated hernias, intestinal kinking from intra-abdominal adhesions, post-traumatic or surgical enteroanastomoses, radiation enteritis, etc.), blind pouches, afferent loops, or diverticulae, is the root cause of primary enterolith formation.1,2 Secondary-type enteroliths are formed in the organs outside of the gastrointestinal tract and then migrate into the bowel, with the most common type being gallstones. 3 Tuberculous stricture is the most common cause of intestinal stones. 4 In selected populations, the prevalence of enterolithiasis ranges from 0.3% to 10%. 1 The death rate of uncomplicated primary enterolithiasis is very low; however, mortality ascends to 3% in poorly conditioned patients with substantial obstruction and a late diagnosis. 5 Enteroliths can be detected in up to a third of the cases with plain abdominal radiography. 1 Primary enteroliths remain an uncommon medical phenomenon, with isolated case series or reports in the setting of mechanical SBO. Here, we present a case of a partial SBO caused by multiple primary enteroliths.
Case report
A 21-year-old woman was admitted for gradually progressive colicky pain over the hypogastrium for 6 days, associated with vomiting and constipation. She was able to pass flatus, but with cessation of bowel movements. She was diagnosed to have ulcerative colitis (UC) in the past for which total colectomy was performed, followed by a manual side-to-end ileorectal anastomosis. She had previous episodes of partial SBO that resolved with antispasmodics and had an untreated menometrorrhagia for the past year.
She was hemodynamically stable and her abdomen was not distended. Multiple scars from previous abdominal surgery were visible. There was tenderness in all four quadrants, but no signs of peritonism. No anterior wall defects were palpated. Bowel sounds were hyperactive. Parents rejected vaginal and rectal examination.
Plain abdominal X-ray showed multiple radiopaque shadows within the small bowel, no air–fluid levels or dilated loops. We further proceeded with plain computed tomography scan to reach to a final diagnosis of multiple enterolithiasis in the small bowel (Figure 1).
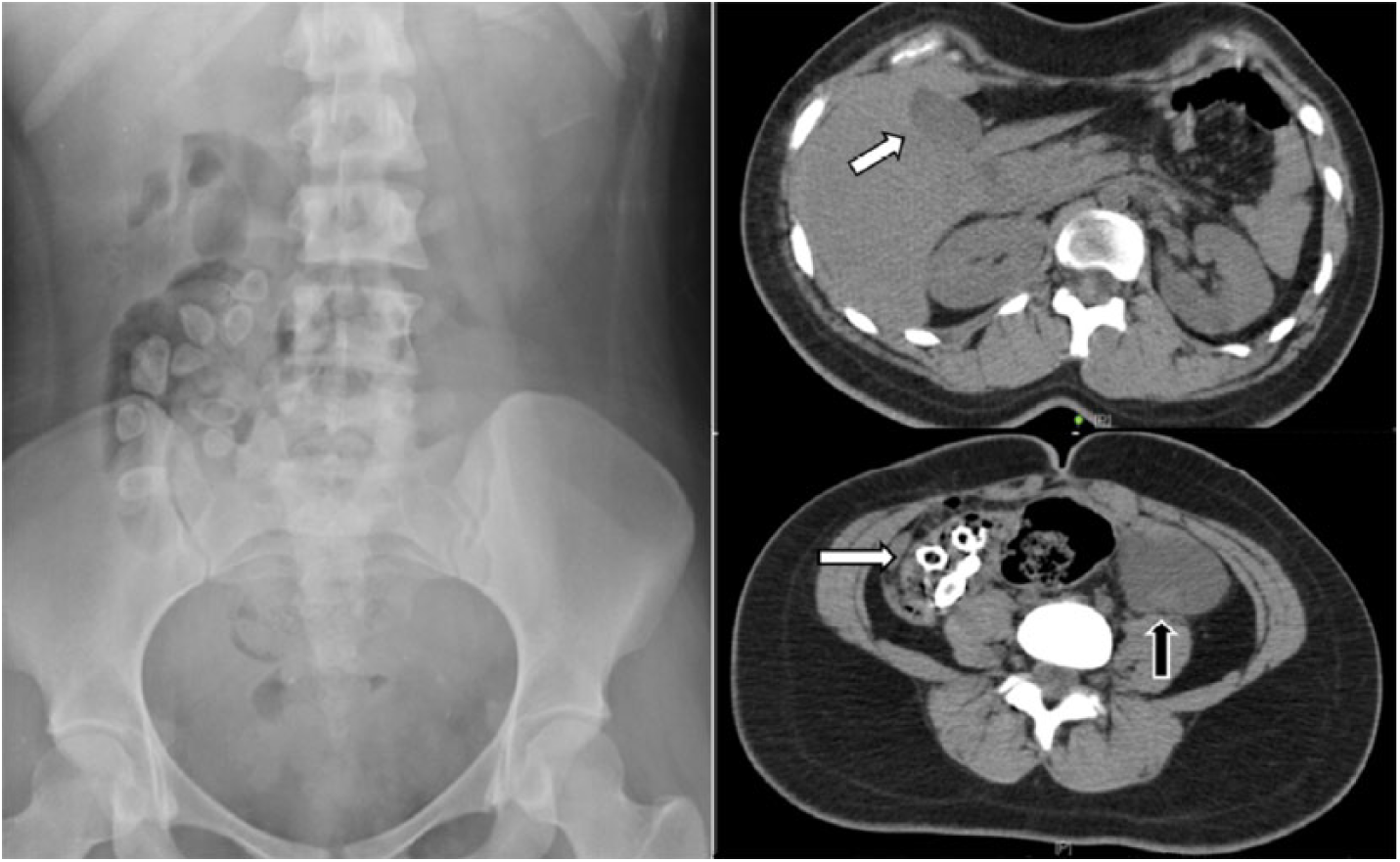
Plain abdominal X-ray film showing multiple radiopaque shadows within the small bowel (left). Axial CT (top right) showing absence of gallstones (white arrow). Axial CT (bottom right) showing intraluminal ovoid structures with peripheral calcification and a hypointense center (white arrow) and (bottom left) adnexal mass (black arrow).
Laparotomy was done after 48 h of poor response to conservative management. Abdominal exploration revealed multiple dense and cohesive adhesions predominantly in the distal small bowel. An anastomotic ileorectal stricture was found, along with multiple stones. The size of the enteroliths averaging 1 cm did not allow manual “milking” of the stones into the rectum (Figure 2). In the pelvic cavity, a cystic mass in the left ovary was found. No communicating fistula was identified between gallbladder and duodenum. Next, left salpingo-oophorectomy was performed, stricture was excised, stones were removed, and intestinal continuity restored with manual end-to-end ileorectal anastomosis at a distance of 12 cm from the anal verge. This was followed by dilation and curettage (D&C).

(a) Ovarian cyst alongside multiple enteroliths with an average diameter of 1 cm after surgical removal. (b) Intact left corpus luteal cyst. (c) Ovarian cyst alongside multiple enteroliths with an average diameter of 1 cm after surgical removal. (d) Dissected enterolith with exposed core showing white-colored aggregates.
In the post-operative period, marked malnutrition was detected with a decrease in serum albumin; for this reason, total parenteral nutrition (TPN) was initiated; 5 days after ex-lap, she presented abundant discharge of succus through the wound. Urgent relaparotomy was performed. Anastomotic leak was found and was managed by dismantling of the anastomosis with closure of the rectal stump and end-ileostomy. Analysis of the biochemical composition of the intestinal stones showed the presence of calcium dihydrate oxalate (85%), calcium monohydrate oxalate (10%), and carbonate apatite (5%). The patient made good recovery and continued well upon discharge.
Discussion
A personalized approach is necessary in the management of enterolithiasis. Timely assessment of underlying pathology is key in establishing effective treatment to avoid stone recurrence. 1 In the context of instestinal obstruction, conservative management may be selectively considered for enteroliths less than 2 cm, in the absence of intraluminal compromise. 6
Successful treatment of intestinal stricturing and stone fragmentation using single- and double-balloon enteroscopy7,8 as well as endoscopic lithotripsy9,10 have been described; however, conclusive evidence is lacking regarding minimally invasive approaches in the removal of enteroliths. Thus far, open surgery remains the mainstay of therapy in the majority of cases. 1
An estimated 30 cases of enterolithiasis in association with CD have been reported. 11 Even though few cases of enterolithiasis-related SBO with stricturing CD have been described, 12 it is accepted that CD is a contributing factor in the development of intestinal stones. 1 In regards to UC, only one case series makes reference to UC as an underlying risk factor. 13 Scant cases of enterolithiasis in association with stricturing UC are reported, 14 with an isolated case presenting as an SBO. 15 Although both forms of inflammatory bowel disease (IBD) are accompanied with intestinal fibrosis and scarring, stricturing UC is rare.5,16 While it is assumed that our patient developed intestinal stones due to anastomotic stricture, it raises the question whether stenosing disease of the bowel due to UC plays a casual or contributing role in the pathogenesis of enterolithiasis.
Conclusion
In the setting of SBO, enterolithiasis is an uncommon medical condition that may fall out of the surgeon’s etiological scope. This clinical and radiological entity should be within the diagnostic and therapeutic purview of the general surgeon, radiologist, and gastroenterologist when assessing patients with SBO. Clinician’s awareness of enterolithiasis as a cause of SBO may yield timely etiologic recognition, treatment, and correction of risk factors for the development and recurrence of stones, thus decreasing morbimortality associated with this pathology.
Footnotes
Acknowledgements
The authors would like to thank Franco Xavier Saucedo Rentería, MD, for his contribution in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.