
Abstract
Objective:
This systematic review was aimed to address the prevalence and causes of intestinal obstruction in Ethiopia.
Methods:
Systematic searches were conducted on PubMed, EMBASE, CINAHL, Scopus, African Journals Online, HINARI, and other supplementary sources, including Google Scholar. We conducted methodological quality assessments for the articles by employing a critical appraisal checklist of Joanna Briggs Institute.
Results:
The reported prevalence of intestinal obstruction in Ethiopia ranges from 18.6% to 50.7% among patients with acute abdomen. However, the prevalence varies from 4.3% to 34.6% among total surgical admissions. The leading causes of small intestinal obstruction were small bowel volvulus, intussusception, and adhesion. Sigmoid volvulus was the most commonly reported cause of large intestine obstruction, followed by colonic cancer.
Conclusion:
The highest reported prevalence of intestinal obstruction in Ethiopia was 50.7% among patients with acute abdomen and 34.6% among surgical admissions. Small intestine volvulus and sigmoid volvulus were the common causes of small and large bowel obstructions, respectively. Therefore, clinicians have to consider the common causes during the diagnosis and management of intestinal obstruction.
Introduction
Intestinal obstruction is a partial or total blockage of the passage of fluids and digested food through the intestines. 1 It is one of the most common acute abdominal disorders which require emergency surgical admission and is commonly related to high mortality of 3%–30% across the globe.2,3 Based on the anatomical location, the intestinal obstruction could be classified as small bowel obstruction (SBO), large bowel obstruction (LBO), and compound obstruction. 1 Also, it can be either mechanical or functional depending on the underlying pathophysiology of obstruction. In 80% of cases, intestinal obstruction occurs in the small bowel. 4
The cause of intestinal obstruction has varied geographically. 5 In developed countries, adhesion is the main cause of intestinal obstruction since hernias and volvulus are the common reasons for intestinal obstruction across Africa.6,7 Although the shreds of evidence illustrate a pattern change in Africa, little is known about the underlying causes.8–10 Despite the above estimations of the global prevalence of intestinal obstruction, it was not well-documented in Ethiopia. However, national evidence on the magnitude of intestinal obstruction is required to make informed health policy decisions. Therefore, we reviewed published and gray literature aiming to document the prevalence and causes of intestinal obstruction in Ethiopia.
Methods
Study protocol
This systematic review was reported based on the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P). 11 The study protocol was registered under PROSPERO (CRD42020202148). 12
Data sources and searches
The online databases and indexing services, including PubMed, EMBASE, CINAHL, Scopus, and African Journals Online (AJOL), were visited as major sources of data and other supplementary sources, including Google Scholar. Advanced search strategies were applied to major databases to retrieve relevant articles closely related to intestinal obstruction. Again, articles published in the subscription-based journals under Wiley’s Online Library were accessed through HINARI. The search was conducted with selected keywords and indexing terms without a time limit.
All published and unpublished articles available online till the day of data collection were considered. Gray literatures from organizations and online university repositories were accessed through Google. Search terms, such as “intestinal obstruction,” “bowel obstruction,” “sigmoid volvulus,” and “Ethiopia” were employed. Boolean operators (AND, OR), truncation, and MeSH terms (Duodenal Obstruction, Fecal Impaction, Ileus, Intestinal Pseudo obstruction, Intestinal Volvulus, Intussusception) were used appropriately for systematic identification of records for the research question.
Eligibility criteria
We included all cross-sectional, case reports, and case series studies conducted in Ethiopia and in the English language without restriction to the date of publication. Furthermore, there was no restriction on the group or age of the participants. However, we excluded articles with incomplete information and study protocols for conferences.
Study selection
We set predefined inclusion and exclusion criteria for initial screening by titles or abstracts and evaluation of full texts for their eligibility assessment. Next, we assessed the original articles reporting obstruction, both small, and large intestine, as the secondary outcome or reported as the etiology of acute abdomen.
Data extraction
A customized data abstraction format prepared on a Microsoft Excel sheet was used to extract relevant data. Two authors (G.F. and A.T.) independently reviewed and extracted data about the first author, year of publication, study design (cross-sectional, case report, and case series), study participants (children, adults, and mixed-age groups), types (small intestine or large intestine), causes of intestinal obstruction, sample size, and event of interest (number of intestinal obstructions). Any discrepancy during extraction was solved through discussions with a third author (B.B.).
Quality assessment
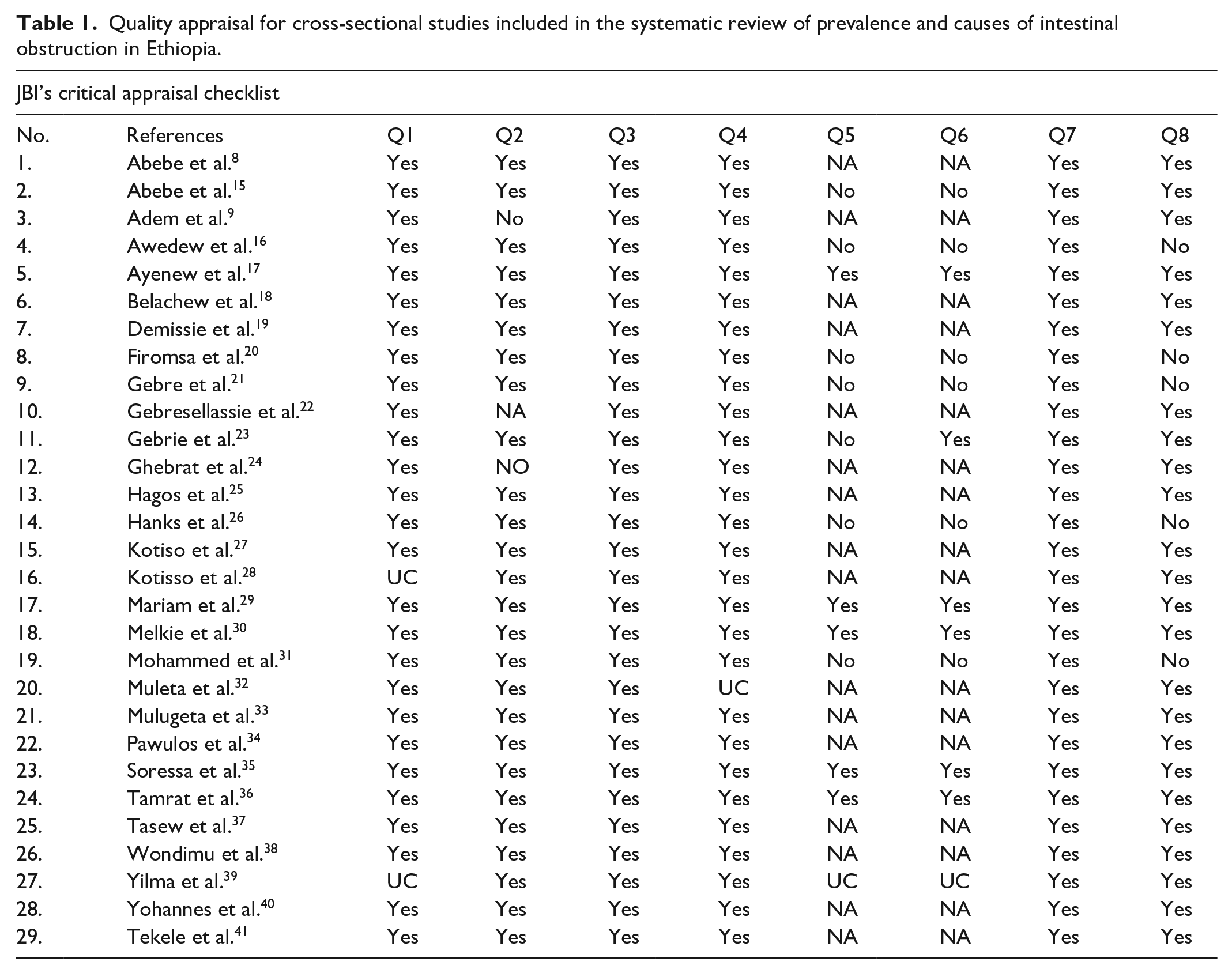
Two independent reviewers, G.F. and A.T., conducted the quality assessment of the articles by employing the Joanna Briggs Institute’s (JBI’s) critical appraisal checklist for all types of studies.13,14 The results of the two authors’ appraisals were used for the final decision of inclusion. Finally, we ranked the articles by their methodological quality based on the total number of appraisers’ scores marked as “yes” to questions of the JBI’s critical appraisal checklist. Any disagreements during appraisal were solved through discussion with the other authors. Accordingly, we included all studies with their overall positive responses in the range of 50%–75% (moderate-quality studies) or higher than 75% (high-quality studies) for the systematic review (Tables 1–3).
Quality appraisal for cross-sectional studies included in the systematic review of prevalence and causes of intestinal obstruction in Ethiopia.
Case series studies included in the systematic review of causes of intestinal obstruction in Ethiopia.

Case report studies included in the systematic review of causes of intestinal obstruction in Ethiopia.
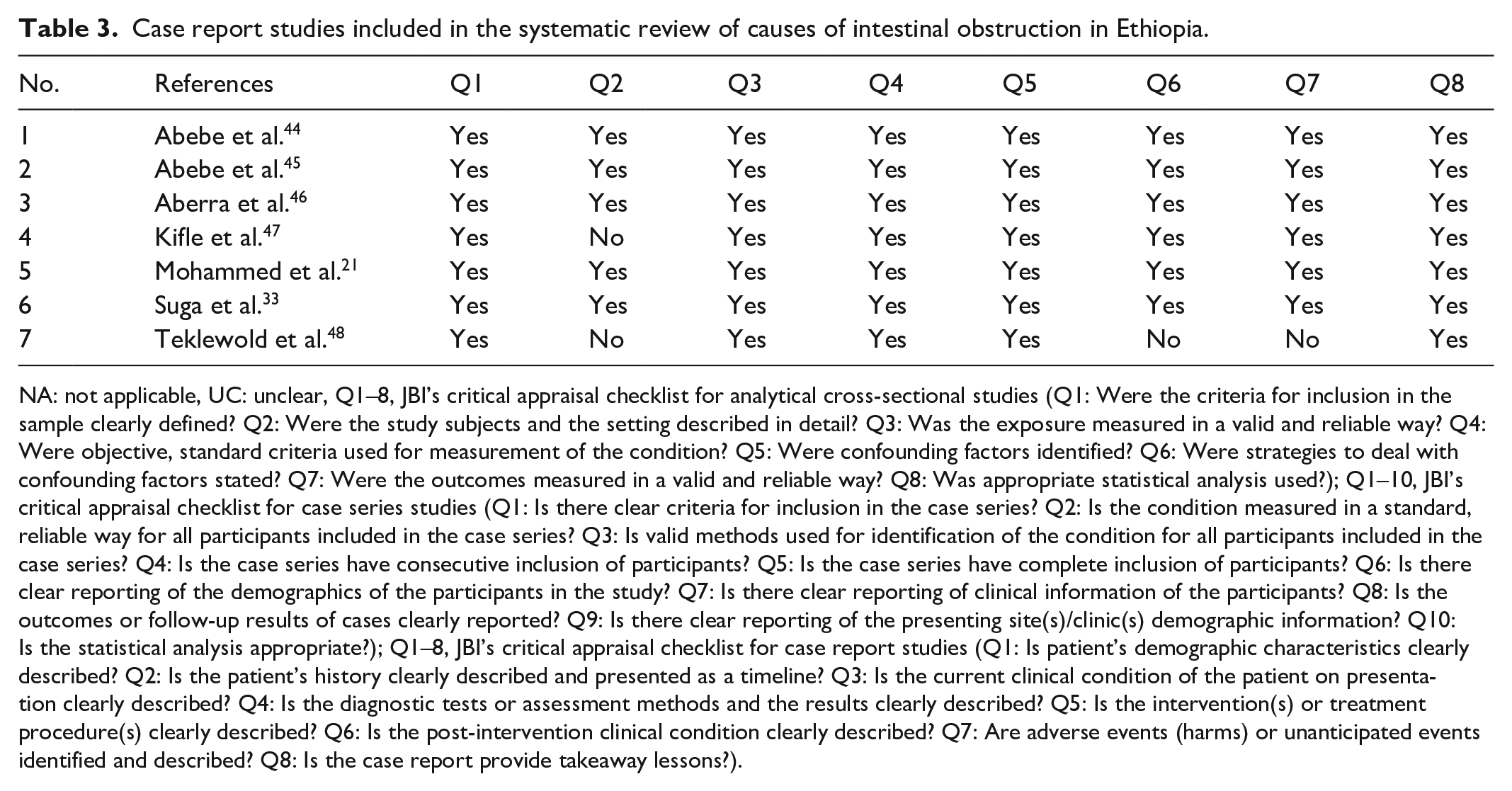
NA: not applicable, UC: unclear, Q1–8, JBI’s critical appraisal checklist for analytical cross-sectional studies (Q1: Were the criteria for inclusion in the sample clearly defined? Q2: Were the study subjects and the setting described in detail? Q3: Was the exposure measured in a valid and reliable way? Q4: Were objective, standard criteria used for measurement of the condition? Q5: Were confounding factors identified? Q6: Were strategies to deal with confounding factors stated? Q7: Were the outcomes measured in a valid and reliable way? Q8: Was appropriate statistical analysis used?); Q1–10, JBI’s critical appraisal checklist for case series studies (Q1: Is there clear criteria for inclusion in the case series? Q2: Is the condition measured in a standard, reliable way for all participants included in the case series? Q3: Is valid methods used for identification of the condition for all participants included in the case series? Q4: Is the case series have consecutive inclusion of participants? Q5: Is the case series have complete inclusion of participants? Q6: Is there clear reporting of the demographics of the participants in the study? Q7: Is there clear reporting of clinical information of the participants? Q8: Is the outcomes or follow-up results of cases clearly reported? Q9: Is there clear reporting of the presenting site(s)/clinic(s) demographic information? Q10: Is the statistical analysis appropriate?); Q1–8, JBI’s critical appraisal checklist for case report studies (Q1: Is patient’s demographic characteristics clearly described? Q2: Is the patient’s history clearly described and presented as a timeline? Q3: Is the current clinical condition of the patient on presentation clearly described? Q4: Is the diagnostic tests or assessment methods and the results clearly described? Q5: Is the intervention(s) or treatment procedure(s) clearly described? Q6: Is the post-intervention clinical condition clearly described? Q7: Are adverse events (harms) or unanticipated events identified and described? Q8: Is the case report provide takeaway lessons?).
Statistical analysis
The extracted data were exported to STATA software version 16.0 for analysis. We reviewed the reported prevalence of intestinal obstruction among patients with acute abdomen and total surgical admission, and the common causes of intestinal obstruction in Ethiopia. Tables and figures were used to present the results.
Results
Description of studies
We identified 471 articles from different sources. Of these articles, 265 were excluded due to duplication, 115 irrelevant outcomes, and 10 studies were conducted outside of Ethiopia. Next, 81 full-text articles were assessed for eligibility. Finally, 38 articles (29 cross-sectional studies, 7 case report studies, and 2 case series studies) were included in our systematic review analysis. The reasons for the exclusion of 43 full-text articles were irrelevant or insufficient information (34) and poor methodological qualities (9) (Figure 1). The majority of studies included patients with a minimum age of 1 day to a maximum of 95 years. Cross-sectional studies were conducted between 2001 and 2020, whereas the case reports and case series studies were conducted between 2015 and 2019.
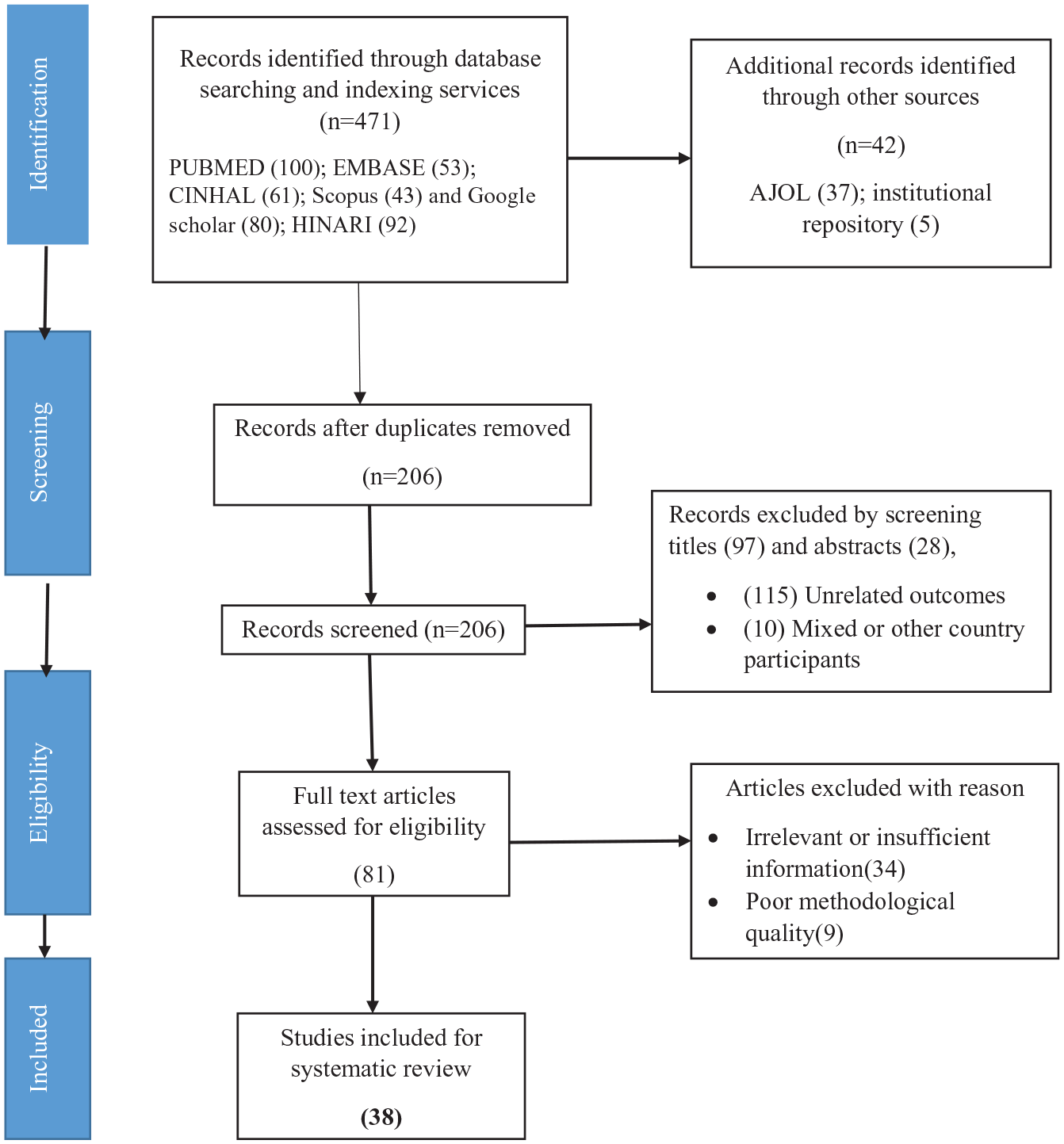
Flow diagram for selection of studies included for the systematic review of prevalence and causes of intestinal obstruction in Ethiopia.
A total of 17 studies from different parts of Ethiopia were included for the review of intestinal obstruction’s prevalence. In addition, for the causes of intestinal obstruction, we included a total of 38 cross-sectional studies, including those studies considered for the prevalence review.
Prevalence of intestinal obstruction
The reported prevalence of intestinal obstruction in Ethiopia ranges from 18.6% to 50.7% among patients with the acute abdomen.21,34 However, the prevalence varies from 4.3% to 34.6% among total surgical admissions.22,36 The highest prevalence of intestinal obstruction, 50.7%, was reported from the Debre Berhan Referral Hospital, Amhara Region, 40 and the lowest prevalence, 18.6%, was reported from Suhul General Hospital, Tigray Region 21 among patients with acute abdomen. According to the administrative regions and cities, in Addis Ababa, the reported prevalence of intestinal obstruction among total surgical admission ranges from 4.3% 22 to 17.1%. 32 Moreover, only one study reported the prevalence of intestinal obstruction, 26%, among patients with acute abdomen in Addis Ababa. 27 The remaining studies have reported the prevalence of intestinal obstruction among patients with acute abdomen. Accordingly, in the Oromia Region, it ranges from 21.8% to 40%,17,35,37 28% to 49.3% in the Southern Nation, Nationalities, and People Region,23,34 18.6% to 37.3% in the Tigray Region.10,21,25 In the Amhara Region, only one study reported the prevalence of intestinal obstruction of 50.7% among patients with the acute abdomen, 40 37.8% in the Dire Dawa city administration, 30 and 34.6% reported by a study conducted at Addis Ababa city and Amhara Region 36 (Table 4).
Descriptive summary of cross-sectional studies included in the systematic review of the prevalence of intestinal obstruction in Ethiopia.

SNNP: Southern Nations, Nationalities, and Peoples.
Causes of intestinal obstruction
A total of 38 studies were included in the systematic review of the causes of intestinal obstruction. More than one cause was reported for each study. It was classified according to the site of obstruction as small and large intestine obstruction. However, there was no case reported on compound obstruction.
Small intestine obstruction
According to the current review, the most common cause of small intestine obstruction was small bowel volvulus which was reported by 14 studies.16,17,19,23,24,27,29,39,40,48,49 Overall, 755 cases of small bowel volvulus were reported, with the highest magnitude of 148 cases from Debre Tabor General Hospital. 16 The second-highest number of intestinal obstructions due to SBO was reported 133 cases from Gondar, Northern Ethiopia. 24
Intussusception was reported by 18 studies as the second most common cause of SBO.10,17–21,23,25,27,29,34,37,39,40,46,49,50 Moreover, Belachew et al. 18 and Yilma et al. 49 reported that three specific types of intussusception; Ileo-colic, Ileo-ileal, and Colo-colic, among children aged 1 month–8 years with a peak occurrence of 3–6 months. While, a case report study from Gondar University also revealed the post-operative intussusceptions. 46
The third most common cause of small intestine obstruction was adhesion which was reported by 13 studies with a total of 327 cases.10,17,19,21,23,27,29,34,37,39,40,50 Among these studies, two of them reported tuberculous adhesions from Adama Hospital 35 and Yirgalem General Hospital. 19
The hernia was reported by 16 studies.10,17,19,20,21,23,25–27,29,34,37,39,40,50 Among those studies, two of them reported incarcerated types of hernia.20,29 Moreover, Ileo-sigmoid knotting was reported by 10 studies.10,15,17,19,23,25,27,34,44 Among those studies, one study was the case report of a 50-year-old female patient who was intraoperatively diagnosed with Ileo-ileal knotting. 44 Similarly, two case reports were presented with appendiculo-ileal knotting from Hawassa hospital 47 and St. Paul hospital. 51 The appendiculo-ileal knotting has been reported with different names in the literature; appendicular tourniquet, appendicular knot, and appendiceal tie syndrome.52–54
In the current review, two studies reported three cases of gossypiboma among women who had cesarean sections. One study reported a case of a 25-year old female patient who had a cesarean section 5 months before being diagnosed with gossypiboma. 45 The other two cases were reported by Alemu et al.; 42 a 32-year-old woman who passed a retained surgical sponge through her rectum 5 months after cesarean section and a 30-year-old woman who presented with an acute abdomen that was later identified as a retained surgical sponge, a year after she had a cesarean delivery.
One case of gallstone was reported from Ethio-Tibeb Hospital. According to the report, an 80-year-old female was presented to the emergency surgical department with the complaints of vomiting and abdominal cramps. On examination, the SBO caused by gallstones was detected and removed by a simple ileostomy. 55 Moreover, three cases of Meckel’s diverticulum were observed.35,56
A cross-sectional study illustrated five cases of small intestine obstruction due to ascariasis lumbricoides among 297 patients. Among them, four cases were managed operatively, while one case was managed conservatively. 39
We found one case of giant mesenteric lipoma which was reported in a 25-year-old male who presented with an acute exacerbation of abdominal pain, nausea, and vomiting. Moreover, a small bowel volvulus with extensive yellow mass was detected during laparotomy. 57
Large intestine obstruction
Sigmoid volvulus is the commonest cause of colon obstruction in Africa. 6 In Ethiopia, 17 studies reported the sigmoid volvulus as the cause of large intestine obstruction.10,17,19,21,23,25–27,29,33–35,37,40,50
Colonic cancer-related causes of large intestine obstruction were reported by 12 studies.10,17,21,23–25,27,35,37,40 Moreover, colorectal cancer was reported by two studies from Wolaita Sodo teaching and referral hospital, SNNP region 34 and from Nekemte referral hospital, Oromia region. 17
A total of 11 cecal volvulus cases have been reported. Three cases were reported from Mekelle hospital, Tigray region, and four cases each were reported from Tikur Anbessa specialized hospital, Addis Ababa city, 28 and Yirgalem referral hospital, SNNP region. 19
We found four cases of anal stenosis which were reported from Tikur Anbessa Specialized hospital among the pediatric population. 20 In addition, Mohammed et al. 31 reported that anorectal malformation, atresia, and meconium ileus were reported as the cause of intestinal obstruction among neonates.
The etiologic cause underlying constipation also causes fecal impaction, which is the rare cause of colon obstruction. The congenital disorders of the colon and rectum, including Hirschsprung’s disease, may cause fecal impaction. 58 Soressa et al. 35 reported two cases of fecal impaction from Adama Medical College Hospital among adult patients. Similarly, two studies reported a total of 21 cases of Hirschsprung’s disease from Tikur Anbessa specialized hospital among pediatric population.20,31
Discussion
The epidemiology of intestinal obstruction in Ethiopia varies based on the settings. We review the epidemiology and causes of intestinal obstruction in Ethiopia. According to the current review, the reported prevalence of intestinal obstruction in Ethiopia varies from 18.6% to 50.7% among patients with acute abdomen. Moreover, the prevalence ranges from 4.3% to 34.6% among the total surgical admissions. Literature documented that intestinal obstruction is the leading cause for emergency presentation in low- and middle-income countries, including Ethiopia.4,5 Furthermore, there are wide variations in the prevalence of intestinal obstruction across the world depending on ethnicity, age group, dietary habits, and geographic locations. 59
Small bowel volvulus is a rare cause of surgical emergency in high-income countries, while it is common in Africa. 16 The current review signifies that the first leading cause of small intestinal obstruction in Ethiopia is volvulus. So, clinicians should bear in mind the commonest cause of intestinal obstructions during the diagnosis and treatment of patients with intestinal obstructions.
The second common cause of intestinal obstruction was intussusception followed by adhesion. Inconsonance with the current finding, the study results from Rwanda reported intussusception as the second leading cause of SBO followed by adhesion. 60 The same pattern is found in many African countries, particularly in rural settings.6,61 However, adhesion is the leading cause of SBO in high-income countries, parts of Asia, and the Middle East.62,63
Hernia and knotting were also reported as the fourth and fifth causes of SBO according to the current review. Concur with the current finding, studies conducted in other African countries have reported a higher magnitude of SBO secondary to hernia and knotting.64,65
We found that the rare causes of SBO include ascariasis, gossypiboma, and gallstone ileus. Such causes of small intestine have also been reported previously in the literature.55,66 In particular, gossypiboma is an ethico-medical issue that needs due attention from clinicians and other stakeholders. The cases were reported among post-cesarean section women, which signify the need to take precautions during cesarean surgical procedures since the highest prevalence of cesarean delivery beyond the WHO recommendation has been reported in Ethiopia and other African countries.7,67,68
Sigmoid volvulus is the initial and most common cause of colon obstructions in Ethiopia, according to the current review. In agreement with the current finding, it is the most common cause of LBO in numerous regions of the world, with 1%–7% in the United States 69 and around 80% in the Andes. 70 Also, it is the leading cause of colon obstruction in most African countries.71,72
Numerous risk factors attributed to sigmoid volvulus include a narrow mesocolon at its parietal attachment producing an excellent pivot point for a redundant sigmoid colon, predisposing the individual to volvulus. 52 In addition, studies have illustrated that advanced age, medications altering intestinal motility, chronic constipation, consumption of high fiber diets, 73 history of abdominal surgery, neurological or psychiatric illness, pregnancy, high altitude, and megacolon contribute to sigmoid volvulus.4,33,38
Globally, colon cancer is the third most commonly diagnosed cancer in males and the second among females. 74 Also, it is the fourth most frequently diagnosed cancer. Furthermore, the second leading cause of death in the United States. 75 It was once the primary disease solely observed in high-income countries. Conversely, recently, the paradigm has shifted to middle- and low-income countries. 76 In Ethiopia, it is the most common type of cancer diagnosed among males and the fourth among females. 77 In the current review, it is the second most common cause of LBO in Ethiopia. 76 Therefore, health education and early screening for high-risk groups of the population are paramount to reducing the debilitating effects of colonic cancer.
The current review pointed out the prevalence of intestinal obstructions and underlying causes in Ethiopia. It gives national insight and would be used by policymakers to due attention and plan for intervention toward the intestinal obstructions. The result of the current review also helps to guide the clinicians for diagnosis and treatment plans.
We have followed the standardized method of reporting the systematic review, critically evaluated the quality of articles included for systematic analysis, and exhaustively incorporated all relevant articles, which were the strengths of our work. However, the current review was not without limitations. We could not obtain the pooled prevalence due to the high heterogeneity (> 90%) detected during the meta-analysis.
Conclusion
The current review revealed nearly 6% of patients presented with acute abdomen or for abdominal surgery have an intestinal obstruction. The leading cause of SBO in Ethiopia was volvulus, followed by adhesion and hernia. Moreover, the sigmoid volvulus and colonic cancer were found to be the commonly reported causes of colon obstruction. Having knowledge of the prevalence and common causes of intestinal obstruction will assist clinicians with early diagnosis and treatment.
Footnotes
Acknowledgements
We would like to thank Fekede Asefa (PhD) for his support in extraction of the articles from an online databases.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Availability of data and materials
The dataset used for analysis could be shared with reasonable request from corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.