
Abstract
Cyst or thrombus formation in the left ventricular outflow tract of a normal heart is very rare. We present a case of a male who presented with a major stroke and was found to have a freely mobile cystic mass in the left ventricular outflow tract, with an otherwise completely normal heart. He had some risks factors for hypercoagulability (reduced protein C activity and raised fibrinogen), but only received aspirin therapy due to his stroke severity (haemorrhagic transformation). Once his brain imaging suggested it was safe to proceed, repeat imaging showed the mass had gone, so cardiac surgery was avoided. What was it and where did it go?
Introduction
A thrombus is the final product of blood coagulation and is composed of aggregated platelets, red blood cells and a mesh of fibrin. According to Virchow’s triad thrombi occur when three antecedents are met: vascular stasis, hypercoaguability and vascular damage. A cyst is defined as a thin-walled hollow cavity containing fluid. Cardiac cystic masses are rare and are usually seen in association with underlying cardiac/valvular pathology.1,2 Cyst or thrombus formation in the left ventricular outflow tract (LVOT) of a normal heart is a very rare occurrence and does not seem to have been reported previously. Cystic thrombi are rarely smooth and completely spherical. 2
Case
A 40-year-old male presented to the Emergency Department following a collapse and was found to have left sided weakness. He denied chest pain, palpitations, dyspnoea or dizziness. He also reported decreased vision is his right eye. Computed tomography (CT) of his head showed a large right fronto-parieto-temporal cortical and subcortical hypodensity involving the right middle cerebral artery territory, producing a mass effect and midline shift of 4.2 mm (Figure 1). CT angiography and head perfusion showed total occlusion of the distal right common carotid artery (Figures 2 and 3). He reported that he had no fever.

CT head – showing a large right fronto-parieto-temporal cortical and subcortical hypodensity, producing a mass effect and midline shift of 4.2 mm and midline shift.
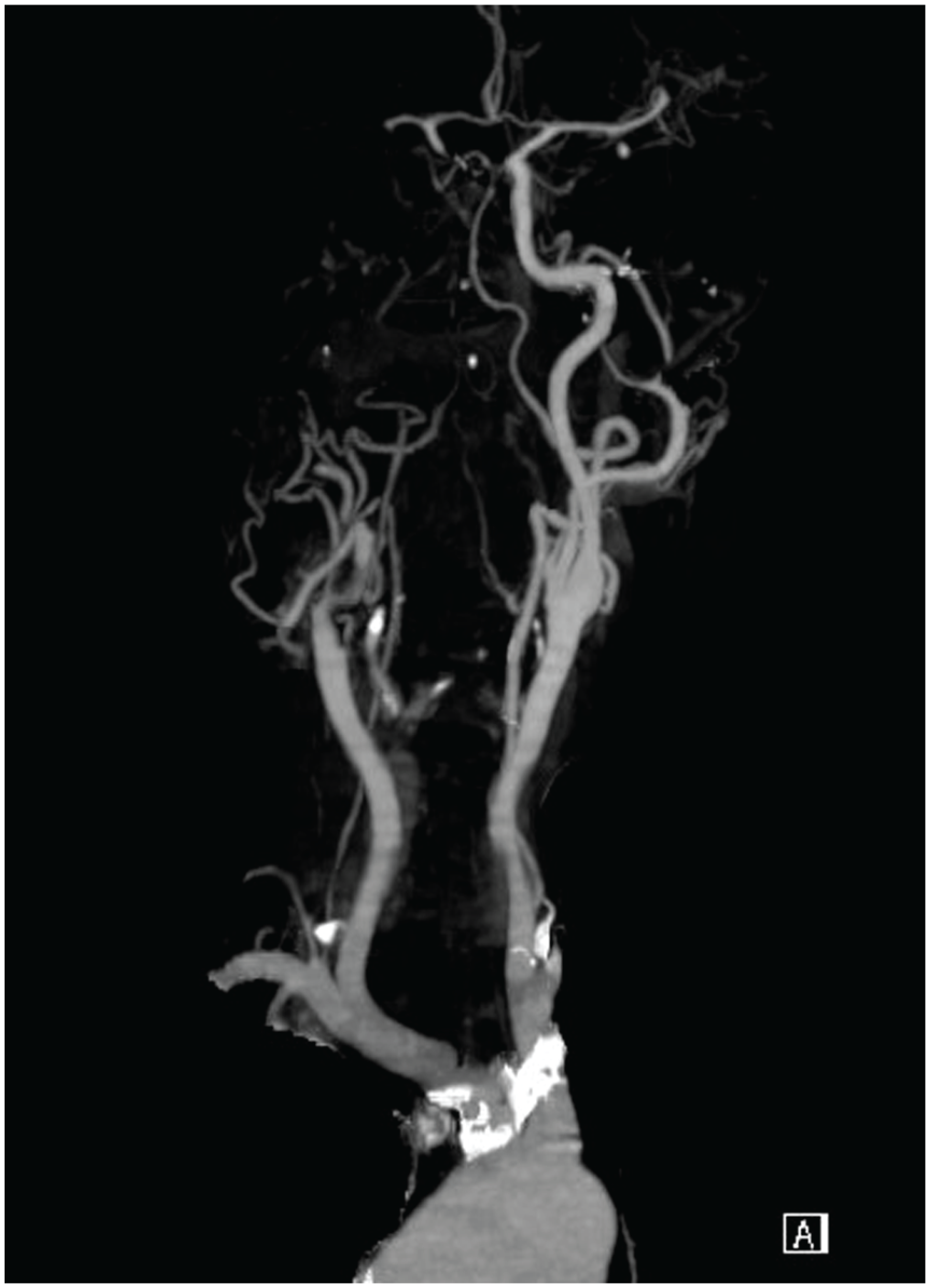
CT angiogram (head) – showing occlusion of the distal right common carotid artery and its distal branches.
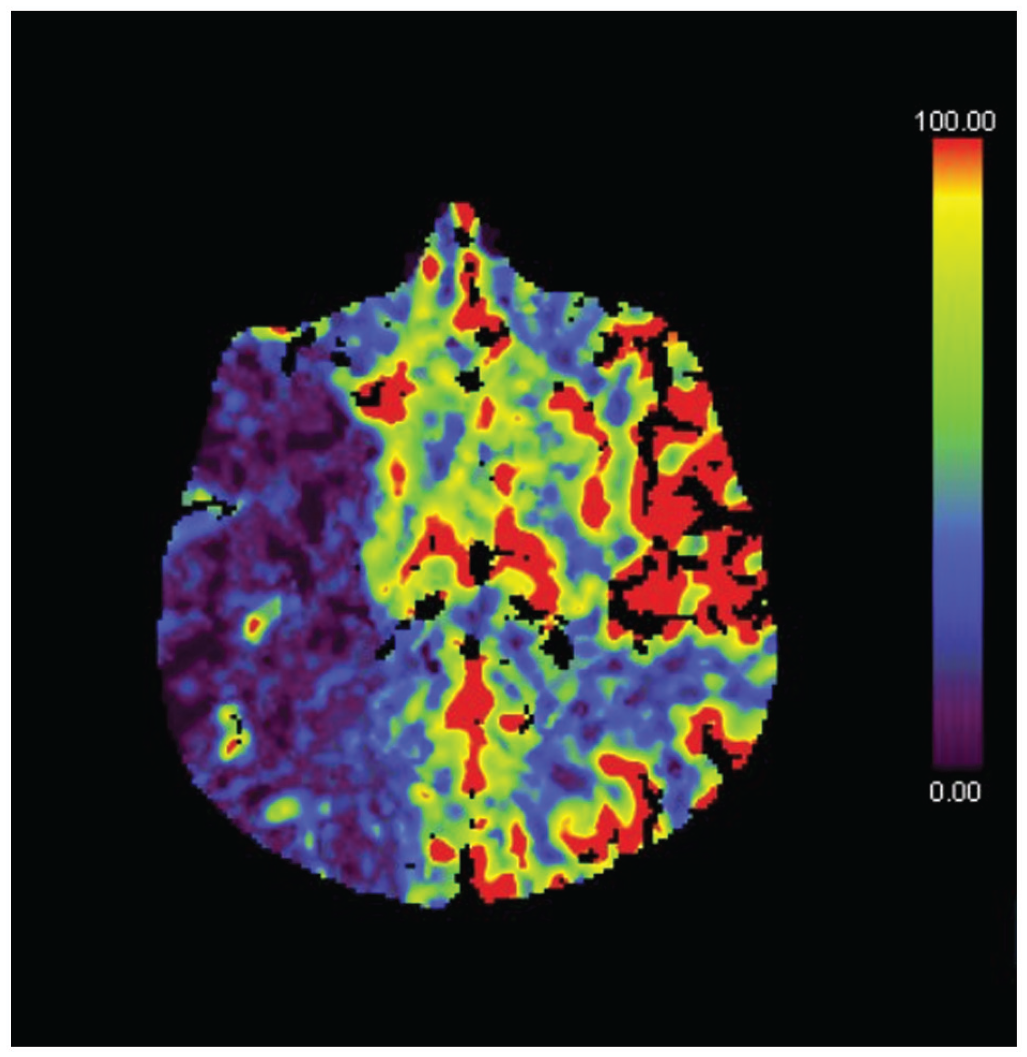
Head perfusion – right fronto-parieto-temporal stroke with a core of infarct and surrounding penumbra due to occlusion of the distal common carotid artery and its distal branches.
On admission his National Institute of Health Stroke Scale (NIHSS) 3 was 18 (a score of 16–20 is considered moderate to severe stroke), so he was not a candidate for thrombolysis. He was assessed by neurosurgery with a decision that no surgical intervention was required as his Glasgow Coma Scale was 15. 4 The patient declined magnetic resonance imaging (MRI), at that time. The patient underwent serial CT scans and the neurologists were initially very concerned about his haemorrhagic transformation. We waited until they gave clearance.
Blood investigations showed raised haemoglobin of 17.1 g/dL (haemotocrit 51.5) with a slightly reduced protein C activity (59.8%) and normal protein S activity (94.5%) as well as normal antithrombin activity. His protein C resistance was 0.87, and he also had a raised fibrinogen level at 5.25 g/L (normal range 1.7–4.2 g/L). An autoantibody screen was negative. Due to the likelihood of an embolic event, he underwent cardiological assessment. Transthoracic echocardiography showed a highly mobile cystic mass seen in the LVOT (Figures 2 and 3). There was no aortic regurgitation present. Transoesophageal echocardiogram confirmed the cystic mass to be 12 × 8 mm and attached to the undersurface of the non-coronary cusp in the LVOT with normal aortic valve appearance and function (Figures 4 and 5). Hydatid cyst was excluded by serological investigations.
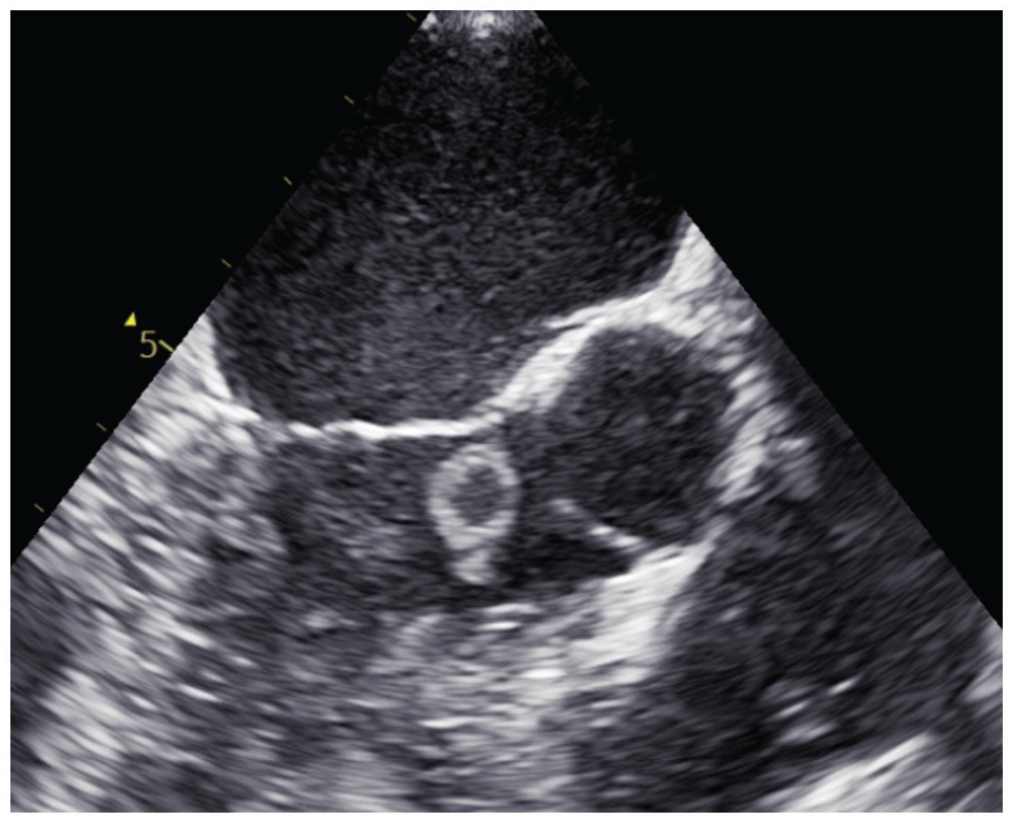
Transthoracic echo – a highly mobile cystic mass measuring 12 × 8 mm is seen, attached by a very short pedicle to the left ventricular outflow tract.

Transthoracic echo – a highly mobile cystic mass attached at the base of the non-coronary cusp of the aortic valve.
In view of his recent large cerebral infarction, the neurologists decided to wait until his CT scans were favourable, which took 6 weeks. During this time, the patient finally agreed to undergo MRI that confirmed the infarction related to the right middle cerebral artery occlusion with multiple foci of resolving micro-haemorrhages. He underwent CT coronary angiogram, which was normal. Prior to his planned cardiac surgery, cardiac MRI was performed, which suggested no evidence of a LVOT mass. Transthoracic echocardiogram confirmed no residual lesion (Figure 6). Abdominal CT scan showed scarring in the right kidney, secondary to an old insult, although the patient denied ever having abdominal pain. The patient was managed conservatively and continues his rehabilitation, with no recurrence of the mass.

Transthoracic echo – no mass was visible.
Discussion
Cardiac cystic masses are uncommon and are usually seen in association with underlying cardiac/valvular pathology4,5 such as post-myocardial infarction. Cyst or thrombus formation in the LVOT of a normal heart is a very rare occurrence, and we can find no such cases in the literature.
The differential diagnosis of cystic cardiac masses includes infectious, vascular malformations, cystic thrombi or oncogenic causes.4,6 Normally, thrombus forms secondary to an underlying abnormality or hypercoagulability, as stasis is not really seen in a normal heart (Virchow’s triad of blood stasis, hypercoagulability and endothelial injury). 5 Early diagnosis and treatment are important as embolic complications may result if thrombi are left untreated, but unfortunately embolic complications may be the presenting feature (as in our case). Although anticoagulation is the treatment of choice (3–6 months), some patients may have contraindications to this modality of treatment, and cardiac surgery may be necessary to remove the lesion.
Conclusion
If a patient with a cardiac mass is to undergo delayed cardiac surgery, further imaging prior to the surgery should be performed, as there is a chance the lesion may have disappeared/resolved.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. This manuscript has not been published or under consideration elsewhere.