
Abstract
Intracranial epidermoid cysts, also referred to as intracranial primary cholesteatomas, are uncommon, benign tumors characterized by slow, linear growth patterns akin to normal epidermal tissue. They typically become symptomatic around age 43, with a slight female predominance, and are most frequently located in the cerebellopontine angle. This summary presents the case of a 62-year-old woman suffering from paroxysmal excruciating pain of the right hemiface, indicative of trigeminal neuralgia, linked to an intracranial epidermoid cyst in the cerebellopontine angle. Radiological assessment, through magnetic resonance imaging, was instrumental in identifying the cyst. Total surgery resection is the most effective treatment, but it can be challenging due to tumor adherence to important neurovascular structures, therefore responsible for an incomplete removal of the proliferative capsule causing a higher risk of recurrence. The case also raises questions about treatment options, as the patient opted against surgical intervention. Managing intracranial epidermoid cysts requires a careful weighing of potential benefits against associated risks.
Introduction
Intracranial epidermoid cyst, also known as intracranial primary cholesteatoma, is a benign, rare, congenital tumor, with a linear slow growth pattern similar to the normal epidermis, 1 that represents 0.3%–1.8% of all primary intracranial tumors. 2
Though they can develop extradurally in the intradiploic area of the frontal, parietal, temporal, and occipital bones, intracranial epidermoid cysts are found in the intradural compartment in about 90% of cases. 2 Their most frequent locations are the cerebellopontine angle in 40% of cases, the parasellar region in 30%, and the fourth ventricle in 5%–18% of cases. 2 The middle cranial fossa, diploe, and spinal canal are less common locations. 2
Given this, symptoms usually develop at a mean age of 43 years, with a slight female predominance of 56%. 1
Case report
We present the case of a 62-year-old woman with no prior medical history, who suffers from paroxysmal spasm of the right hemiface associated with cruciate pain. It occurs spontaneously and is sometimes triggered by trivial stimuli like talking or chewing, known as trigeminal neuralgia.
Standard magnetic resonance imaging (MRI) sequences with a 1.5 Tesla (T) superconducting system (siemens) were first performed, to exclude an intracranial abnormality, rapid spin echo T1 in the sagittal plane, T2 in the axial plane, three-dimensional (3D) fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted imaging (DWI). To assess the trigeminal nerve pathway and other cranial nerves, 3D high-resolution T2-weighted sequence and gradient recalled echo (CISS) were also obtained, revealing the presence of a well-defined mass in the cerebellopontine right angle hypo signal compared to the cerebrospinal fluid surrounding the ipsilateral Vth cranial nerve and responsible for a mass effect on its cisternal segment (Figure 1(a–c)). This mass presents a high restriction in the DWI (Figure 2(a) and (b)), no contrast uptake in 3D contrast T1-weighted imaging (Figure 3), and a hypersignal 3D FLAIR (Figure 4). All favorable of an epidermoid cyst.
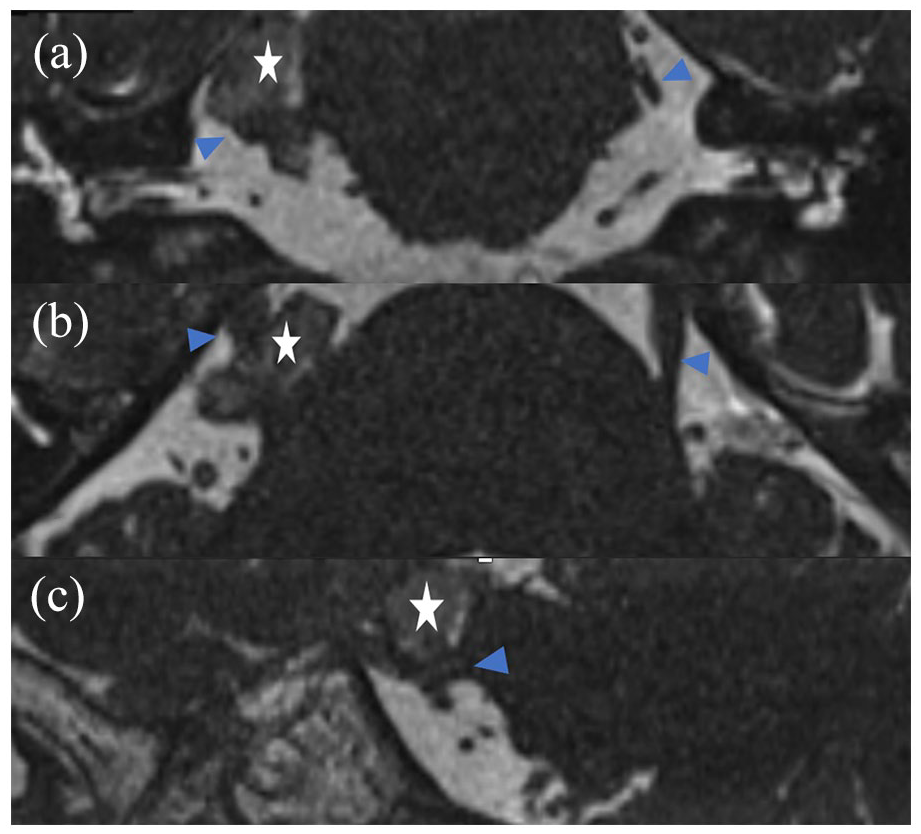
3D high-resolution T2-weighted sequence, gradient recalled echo (CISS) images, coronal (a) axial (b), and sagittal (c) showing a well-defined mass (asterisk) in the cerebellopontine right angle hypo signal compared to the cerebrospinal fluid surrounding the ipsilateral Vth cranial nerve and responsible for a mass effect on its cisternal segment (arrow).
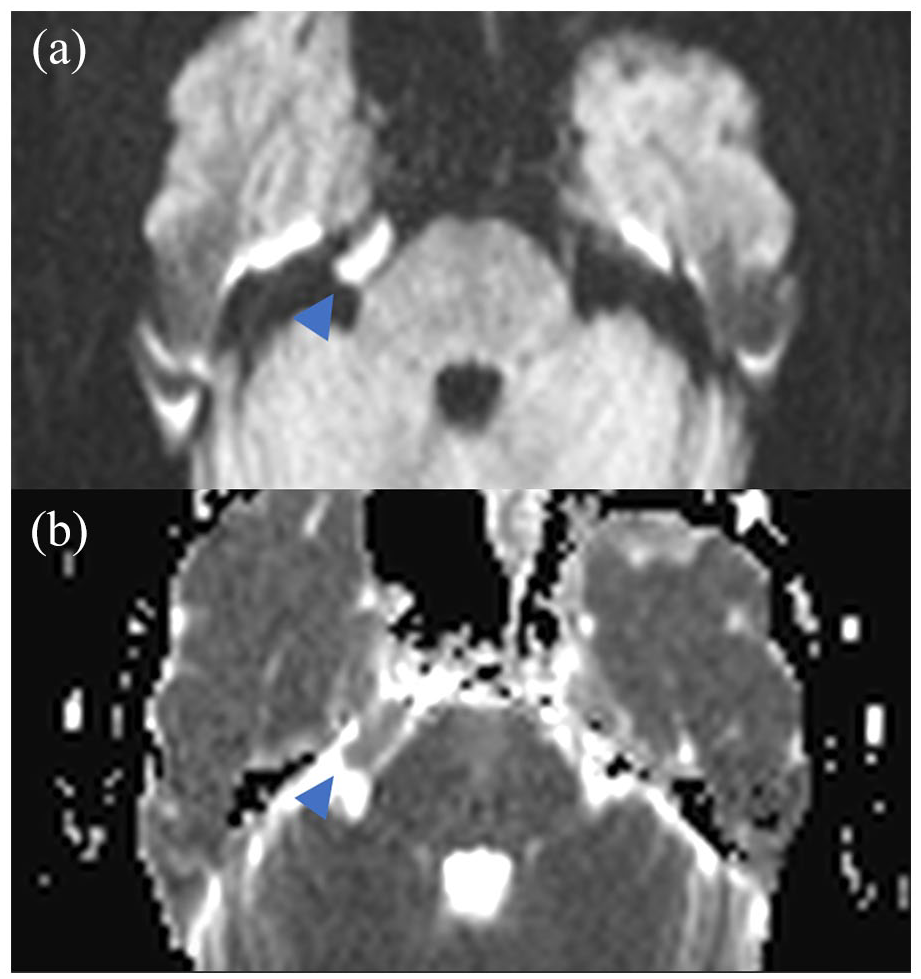
Diffusion-weighted imaging (a) with apparent diffusion coeffecient (ADC) mapping (b) reveals a mass with high restriction (asterisk) in the cerebellopontine right angle.
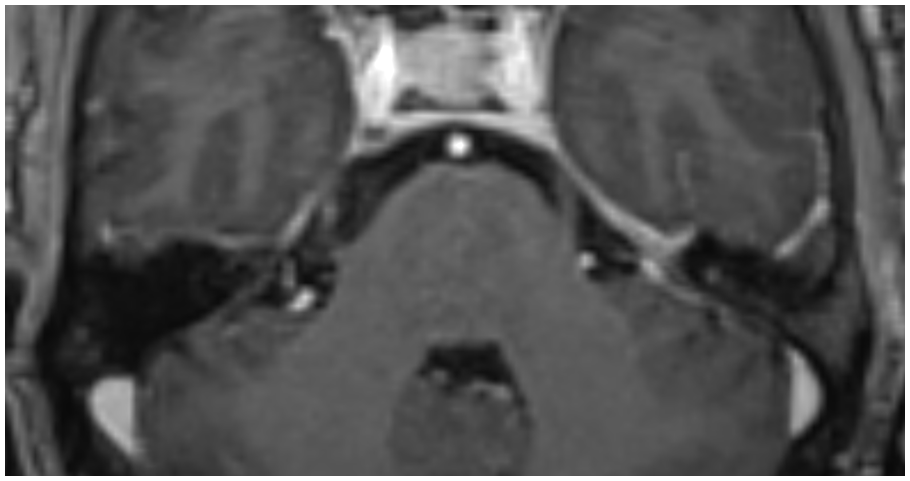
Axial contrast T1-weighted imaging shows the mass in the cerebellopontine right angle hypo signal with no contrast uptake.
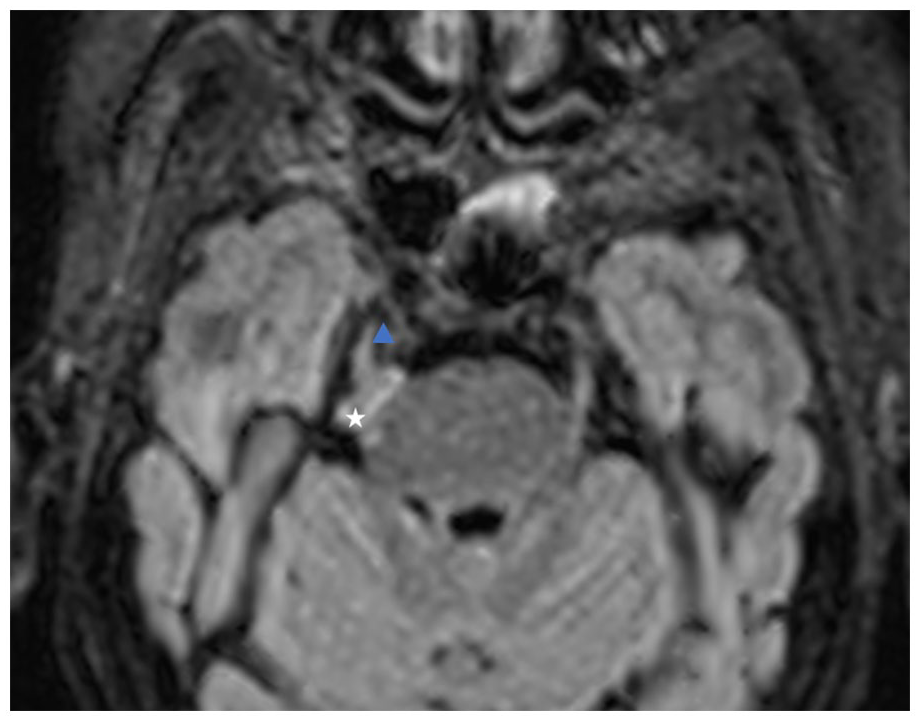
Three-dimensional (3D) fluid-attenuated inversion recovery (FLAIR) axial reconstruction image shows a hyperintense lesion (asterisk) in the cerebellopontine right angle with intimate contact with the ipsilateral Vth cranial nerve.
The patient declined the recommended surgical treatment due to its intimate contact with the Vth cranial nerve and the high risk of nerve palsy and recurrence if incomplete removal, and refused any follow-up.
Discussion
The cerebellopontine angle is the most frequent location of an epidermoid cyst. These tumors, although growing slowly, have a strong tendency to adhere to important neurovascular structures and impinge due to the mass effect, resulting in neurologic impairment. 2
The pathogenesis of the intracranial epidermoid cyst can be explained by the development of epidermal components during neural groove closure between the third and fifth weeks of embryonic life. Migration of otic vesicles or developing neurovascular structures triggers the proliferation and lateral migration of embryonic or transplanted epithelial cells, leading to the characteristic lateral inclination of the epidermoid cyst. 3 The separation of neuroectoderm from its cutaneous counterpart results in the median placement of epidermoid tumors, which is typically characteristic of dermoid tumors. In addition, reports of possible iatrogenic occurrence of the epidermoid cyst after many subdural taps have been made. 3
The subarachnoid space is filled by an epidermoid tumor before the neuronal and vascular systems are moved, extending from the cisternal space into the brain stem, manifesting as an exophytic lesion in the pons or medulla. Over time, the brain stem parenchyma may cover the cyst substance, giving the lesion an endophytic appearance. 3
The buildup of desquamated epithelial cell breakdown products is what causes the tumor to enlarge. Their characteristic pearly or milky-white macroscopic appearance is caused by the accumulation of keratin and cholesterol in the subarachnoid region. 3
The disease follows a typical progression pattern: initially asymptomatic for an extended period, followed by the tumor capsules exerting pressure on a cranial nerve or surrounding brain tissue, leading to rapid functional deficits. 2 Its intimate contact with the Vth cranial nerve, such as in this case, can cause structural changes responsible for an alteration of the nerve function and therefore trigeminal neuralgia.
One of the most striking clinical manifestations associated with epidermoid cysts in the cerebellopontine angle is trigeminal neuralgia. Trigeminal neuralgia is a specific clinical condition marked by an intense pain burst in the sensorimotor distribution of the trigeminal nerve, which is responsible for facial sensation and motor control, and is usually associated with hypersensitivity to non-nociceptive stimuli. 4
The structural changes caused by the presence of an epidermoid cyst in the cerebellopontine angle contribute to trigeminal neuralgia. These changes may include distension, dislocation, or distortion of adjacent structures, particularly the trigeminal nerve itself. As a result, the nerve becomes compressed or otherwise affected, leading to severe pain episodes of characteristic of trigeminal neuralgia.
The epidermoid cyst has a typical radiological finding, and computed tomography (CT) scan can reveal the presence of a hypodense well-defined mass with a possible marginal calcification. MRI sequences are particularly valuable for confirming the nature of the cyst and its relationship with adjacent anatomical structures. Typically, an epidermoid cyst is a well-defined mass usually heterogeneous, hypointense in T1-weighted sequence, hyperintense in T2-weighted sequence, with a higher signal than the cerebral spinal fluid, hyperintense in 3D FLAIR unlike the arachnoid cyst, shows a typically restricted lesion in DWI, and no adjacent bone erosion. 5
The third most frequent tumor in the cerebellopontine angle is the epidermoid cyst. Arachnoid cysts are the most common differential diagnosis, with smooth margins, the same signal as cerebrospinal fluid, no DWI restriction, and erosion of the neighboring bone. The primary sequences that aid in distinguishing between an arachnoid and an epidermoid cyst are the DWI and FLAIR sequences. 5
Dermoid cyst usually contains fat, calcifications, or hair. The CT scan shows a negative attenuating lesion (fat) and the MRI shows a hyperintense lesion on T1-weighted images with a possible fluid fat level. 5
As for miscellaneous cysts, rarer encounters, such as neurocysticercosis, neurenteric cyst, and neuroepithelial cyst, have an identical signal to the cerebrospinal fluid with no DWI restriction and no contrast uptake 5 (Table 1).
Radiological findings of cystic lesions of the cerebellopontine angle.

One notable MRI sequence that provides valuable insight, especially when dealing with cysts located within the cerebellopontine angle, is a 3D high-resolution T2-weighted sequence, gradient recalled echo (CISS). This sequence helps to establish the exact location of the cyst and a comprehensive of its relationship with the cranial nerve, such as the trigeminal nerve in the case discussed.
It is important to acknowledge, however, that the preoperative and postoperative radiological findings may not always perfectly align with per-operative observations. The exact reasons for these discrepancies can vary and may be attributed to factors such as the dynamic nature of tissues and structures within the cranial cavity. This underscores the complexity of radiological evaluation in cases of epidermoid cysts and the significance of clinical assessment and surgical exploration in ensuring accurate diagnosis and treatment. 6
Radical surgical resection stands as the most effective treatment for patients, given the current lack of targeted therapy or specific chemotherapy for this type of tumor. However, surgery poses challenges due to the tumors’ tendency to adhere to critical neurovascular structures, often resulting in incomplete removal of the proliferative capsule. Studies have linked inadequate capsule removal to recurrence rates as high as 93%. Therefore, comprehensive surgical resection is crucial in minimizing recurrence risk. 2
Initial surgery should aim for a global resection to maximize success rates and reduce long-term recurrence risks. Achieving a safe global surgical resection may be improved with experienced surgical teams and the use of adjuncts like intraoperative MRI and neuromonitoring. 7 Temporary cranial nerve palsies emerged as the most common surgical complications, occurring in patients who underwent both complete and subtotal tumor resections, as documented. 7
In cases where surgical resection is not feasible or in recurring tumors, adjuvant radiation therapy may offer some benefits. However, success rates for reoperations are substantially lower, around 16%, compared to 73% in new cases, owing to adhesions and scar tissue. 2 Following surgery, regular postoperative monitoring with serial MRI scans is strongly recommended for all cases of epidermoid tumors, particularly crucial for those undergoing subtotal resection, even in the years following surgery. 7
Conclusion
In conclusion, this case report highlights the intriguing nature of intracranial epidermoid cysts, emphasizing their rarity and distinct clinical manifestations. We describe a case of a right trigeminal neuralgia caused by a direct compression of the Vth cranial nerve by an epidermoid, in its cisternal segment. While imaging techniques such as MRI and CT scans offer valuable insights into the nature of epidermoid cysts and their precise location, it is important to note that these findings may not always perfectly align with per-operative observations, as previously reported.
When treating these tumors, it is important to remember that aggressive radical surgery has a high risk of morbidity and mortality, and an incomplete tumor excision has a higher risk of recurrence.
Footnotes
Acknowledgements
The authors are grateful for the reviewer’s valuable comments that improved the manuscript.
Author contribution
All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.