
Abstract
Objective:
Early recognition of stroke symptoms and risk factors is important for timely intervention to improve outcomes. This study aimed to investigate differences in stroke frequency, risk factors, and presentation in pregnant and non-pregnant women of reproductive years.
Methods:
This multicenter ambispective cohort study, conducted from 4th August 2021 to 4th March 2023, examined strokes in women of reproductive years at the neurology outpatient/emergency department of five busiest/referred neuro-medical facilities in Karachi, Pakistan, where patients from across the nation are assessed. In all, 1210 patients were enrolled via consecutive or convenient sampling retrospectively from January 2017 to August 2021 and prospectively from August 2021 to March 2023. Pregnancy-related and non-pregnancy-related stroke occurrence and characteristics were compared using the chi-square/Fischer’s exact test.
Results:
56% were non-pregnancy-related strokes and 44% were pregnancy-related strokes with non-pregnancy-related strokes approximately equal throughout the reproductive years (15–24 years = 34%, 25–34 years = 25%, 35–45 years = 41%) and pregnancy-related stroke between 15 and 35 years (82%). In the non-pregnancy-related stroke, arterial stroke dominated (96.4%); while in pregnancy-related stroke, arterial stroke accounted for 61.4% and venous stroke for 38.6% of cases. Middle cerebral artery was a typical stroke site (66%). Infarction was the most significant CT/MRI finding (PRS = 89%, NPRS = 66%), with pregnancy-related stroke hemorrhagic stroke occurring in only 11% of cases and non-pregnancy-related stroke comprising one-third (34%). The most prevalent etiologies were eclampsia in pregnancy-related stroke (32%), hypertension in non-pregnancy-related stroke (40%), and cardiac problems among both groups (25%:33%). Weakness and headache were the common clinical manifestations among both groups. In the pregnancy-related and non-pregnancy-related stroke groups, the initial presentation of stroke resulted in severe disability for 91% and 75%, respectively. With timely treatment, the outcome improved significantly. The mortality rate was 7% for the pregnancy-related stroke group and 4% for the non-pregnancy-related stroke group.
Conclusions:
Our findings show that stroke is prevalent among reproductive-year women, posing a significant mortality risk if not adequately recognized and treated. Awareness, research, and screening of stroke risk factors and their often-overlooked early presentation (i.e., headache and weakness) in reproductive years are essential to reducing stroke occurrence among reproductive-year women.
Keywords
Introduction
A stroke, also known as a cerebrovascular accident, is a sudden impairment of neurological function caused by reduced or diminished blood supply to the brain due to arterial constriction or obstruction.1,2 Studies show that males are more likely to experience a stroke, 3 but recent evidence indicates a minimal difference between the sexes. 4 In middle- to high-income countries, stroke is the second leading cause of mortality among women, and years of life lost due to disability.5,6 Lack of proper women’s healthcare and regular clinical follow-ups are contributing factors. Numerous studies demonstrate that young women have a higher stroke incidence than young men, especially during their reproductive era,5,6 when they require greater medical attention. According to a Toronto General Hospital study, medical professionals typically do not consider reproductive-aged women as probable stroke cases, which may lead to underdiagnosis resulting in higher mortality rates in young pregnant women. 7 Prior stroke research has primarily focused on males or pregnant women, ignoring the vast majority of reproductive-year women (15–45 years). Rarely any study has indirectly compared pregnancy-related stroke (PRS) to non-pregnancy-related stroke (NPRS). 8 One study discovered that PRS is ninefold higher in peripartum and threefold higher in the first 6 weeks of postpartum, 5 indicating that pregnancy elevates the risk of stroke due to pathophysiological changes such as increased coagulation, endothelial damage, blood stasis, increased blood volume, enhanced cardiac output and preload, reduced afterload, and increased heart contractility. 9 However, none of the studies highlighted the risk of stroke in non-pregnant women, who comprise the majority of the world’s population. This lack of knowledge about stroke patterns among groups of reproductive-year women is also a contributing factor to increased mortality rates. Consequently, the authors hypothesize that early recognition of stroke symptoms and risk factors is important for timely intervention to improve outcomes in women of reproductive years.
Henceforth, our principal objective was the assessment of the frequency of PRS and NPRS, with additional focus encompassed a comparative analysis of distinctions between NPRS and PRS among women in their reproductive years, involving considerations such as age, medical history, etiological factors, mode of presentation, stroke type, and involvement of arterial and venous territories. Our secondary aim was to appraise the outcomes and disability in both PRS and NPRS cohorts.
Methods
Study design, setting, and period
This multicenter ambispective cohort study was conducted at five institutions in Karachi, Pakistan: Creek General Hospital (CGH), Neuro-spinal and Cancer Care Institute (NCCI), United Hospital (UH), Fazaia Ruth Pfau Medical College Hospital (FRPMC) affiliated hospital, and RIMS Trauma Hospital. These five institutions were selected because they are the busiest neuro-medical facilities in Karachi, where patients from all social classes across Pakistan are evaluated, particularly for stroke and its type. The study took place from 4th August 2021 to 4th March 2023, following approval from the Ethical Review Committee.
Sample size and sampling techniques
A sample size of 73 was calculated, considering Pakistan’s female population of 109.32 million and a prevalence of stroke of 5%. 10 This study enrolled reproductive-age females with stroke at the Neurology Outpatient Department (OPD)/emergency department of the above-mentioned institutes in Karachi, Pakistan, from 1st January 2017 to 3rd August 2021 retrospectively and 4th August 2021 to 4th March 2023, by consecutively enrolling all female patients who presented with stroke at OPD/emergency department of the above-mentioned convenient sampled hospitals, during the specified conduction time period. The final sample consisted of 1210 patients, after excluding 34 individuals who had missing data, did not meet the inclusion criteria, or were lost during the follow-up.
Inclusion and exclusion criteria
Pregnant and non-pregnant females aged 15–45 years with clinical and radiological diagnoses of arterial and venous strokes at CGH, NCCI, UH, FRPMC, and RIMS in Karachi, Pakistan, were included in this study. Females under 15 or over 45 years old, or those with a clinical and radiological diagnoses other than stroke and not presenting at CGH, NCCI, UH, FRPMCH, or RIMS in Karachi, Pakistan, were excluded from the study.
Statistical analysis
The authors collected data from hospitals’ databases, patients’ file, reports after gaining consent from relevant hospital authorities and patients regarding strokes’ frequency, characteristics, and outcomes among pregnant and non-pregnant females. The tests and imaging modalities used in these institutes for identifying stroke and its associated characteristics are consistent with those employed in other centers across Pakistan (Table 1). The authors identified the stroke from the patient’s file and reported it retrospectively and additional assessment and follow-up in OPD/emergency during follow-up, including the history, clinical examination, and neurological deficit for retrospective data and prospective patients were followed where applicable for the above-mentioned variables. For analysis, the data were entered into SPSS 23 by IBM Corporation (Figure 1). Frequencies and percentages are reported for categorical variables. The chi-square/Fischer’s exact test is utilized to compare NPRS with PRS. A p-value of <0.05 is considered statistically significant.
Methods of identification.

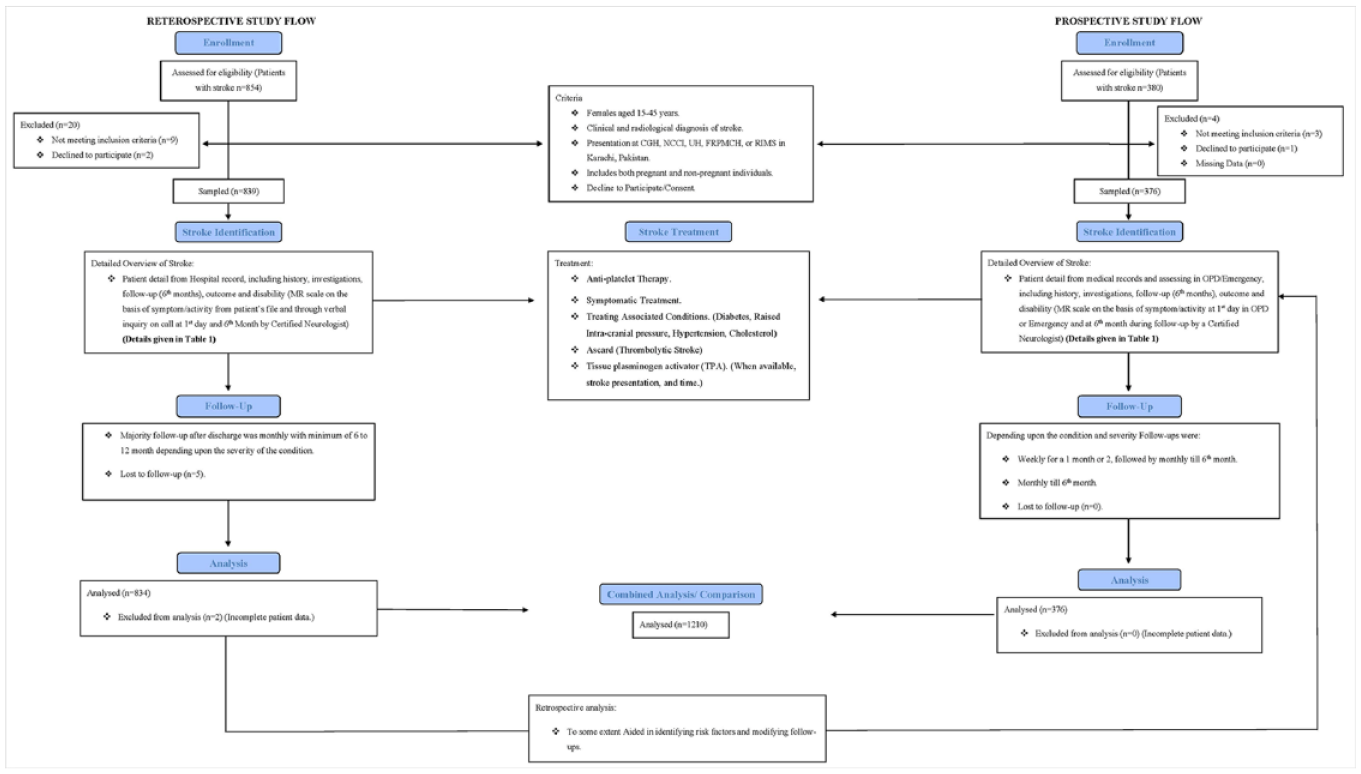
Study design and flow: visual representation in a comprehensive flowchart.
Operational definitions
Peripartum period: The peripartum period includes the time immediately before, during, and after childbirth, up to 24 h.
Postpartum period: The postpartum period, known as the puerperium, refers to the time starting 24 h after birth and lasting up to 6 weeks.
PRS: Pregnancy-related stroke refers to the occurrence of a stroke in a woman during pregnancy, childbirth, or in the immediate postpartum period till 6 weeks.
NPRS: Non-pregnancy-related stroke encompasses strokes that occur in individuals who are not pregnant.
Arterial stroke: Stroke caused by a disruption of blood flow in the arteries supplying the brain, characterized by either an ischemic event (blockage or clot) or a hemorrhagic event (bleeding from a ruptured vessel).
Venous stroke: Stroke occurring in the venous system, when there is a problem with blood flow in the brain’s veins, either due to a clot (thrombosis) or bleeding (hemorrhage), leading to impaired blood drainage from the brain.
Consecutive sampling technique: Consecutive sampling is a non-random sampling technique characterized by the sequential selection of participants based on their availability or order of presentation, devoid of specific randomization procedures.
Convenient sampling technique: Convenience sampling is a non-random method employed in this study for hospital selection, entailing the identification of facilities based on accessibility, practicality, or proximity to the researcher, without the utilization of a random or systematic approach.
Reporting of the study
Strobe guidelines are implemented for study’s reporting (Supplemental Material 1).
Results
Frequency of stroke among females of reproductive years
Of 1234 identified cases of stroke in females of reproductive years, 1210 were recruited, of which 44.1% (n = 534) were PRS, and 55.9% (n = 676) were NPRS, without a significant difference of stroke frequency between the two groups (p-value < 0.05). The PRS was more prevalent in the postpartum period and the peripartum (last trimester of pregnancy) (Figure 2).

Frequency of stroke in different phases of pregnancy (N = 534).
Overall, stroke was prevalent among those aged 15–45 years, with the NPRS being prevalent almost equally among all ages, whereas the PRS was prevalent among those aged 25–34 years. Patients with a past medical history of eclampsia and PIH/PPH were significant stroke risk factors in pregnancy, whereas hypertension was seen in non-pregnant patients. Patients’ past and family stroke histories were not found to be risk factors for stroke in either group, but stroke had a high recurrence among NPRS as compared to PRS in terms of past and family stroke histories (Table 2).
Frequency of age-related, past medical, family, and personal history of strokes in females of reproductive years (N = 1210).

PRS: pregnancy-related stroke; NPRS: non-pregnancy-related stroke; HTN: hypertension; DM: diabetes mellitus; PIH: pregnancy-induced hypertension; PPH: postpartum hemorrhage.
Represents significant p value.
Characteristics and clinical presentation of stroke among females of reproductive years
Most of the strokes were arterial, while venous strokes were only found in a few cases, with the NPRS leaning toward arterial in almost all cases and the PRS being almost two-third arterial and one-third venous, with infarction being predominant in PRS while in NPRS IC bleed and infarction was 1:2. MCA remains the most affected territory, with 66.1% overall, 52.4% in PRS, and 76.9% in NPRS. >1 arterial territory involvement was higher in the NPRS, whereas venous thrombosis was higher in the PRS. On CT/MRI scans, infarction was the most common finding in both groups, while hemorrhage was less common in the PRS but was one-third in the NPRS. Overall, cardiac problems were identified as the leading cause of stroke among females of reproductive age (29.4%), but only 17% of patients were aware of their cardiac issues before experiencing a stroke. Cardiac problems and HTN were the most common etiologies in the NPRS, whereas, in the PRS, the most common etiology was eclampsia, followed by cardiac problems (Table 3).
Characteristics, disability, morbidity, and mortality of stroke in females of reproductive years (N = 1210).

PRS: pregnancy-related stroke; NPRS: non-pregnancy-related stroke; ACA: anterior cerebral artery; LST: lateral sinus thrombosis; MCA: middle cerebral artery; PCA: posterior cerebral artery; PICA: posterior cerebellar artery syndrome; SSST: superior sagittal sinus thrombosis; IC: intracerebral hemorrhage; HTN: hypertension; DM: diabetes mellitus; AVM: arteriovenous malformation; ITP: immune thrombocytopenia.
Represents significant p value.
Valvular heart disease, especially mitral valve disease, was the most common heart problem in 184 (15.2%) patients with heart disease who were either being treated or untreated. NPRS had more IHD and valvular problems, while PRS had more MVR, followed by IHD (Figure 3).
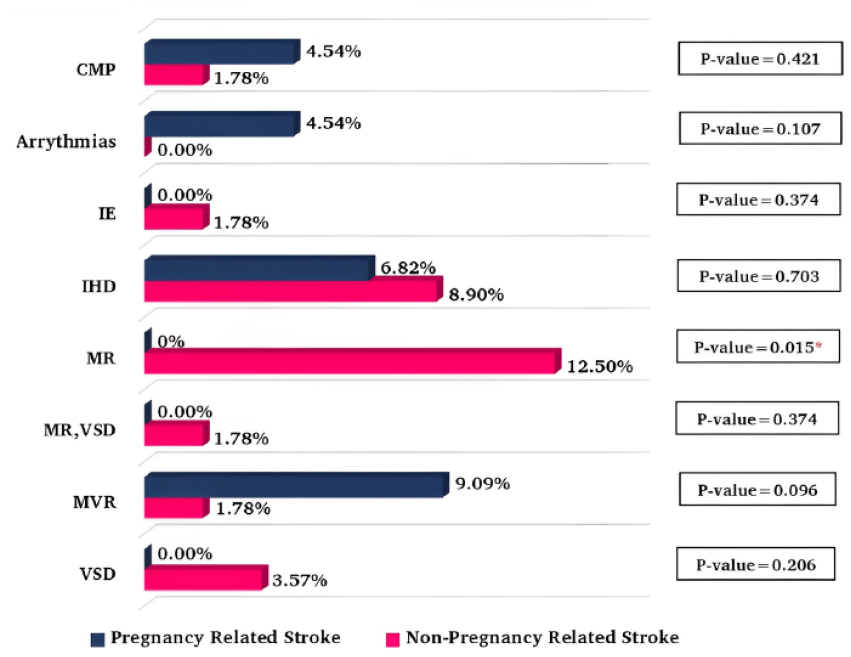
Cardiac problems in pregnancy and non-pregnancy stroke cases (N = 1210).
Motor weakness was the most prevalent symptom in 86% of patients, while headache was the second most prevalent symptom in 46%. In both groups, motor weakness was the most common clinical manifestation of a stroke, followed by headaches. At the same time, unconsciousness and seizures were significantly higher in PRS (Figure 4).
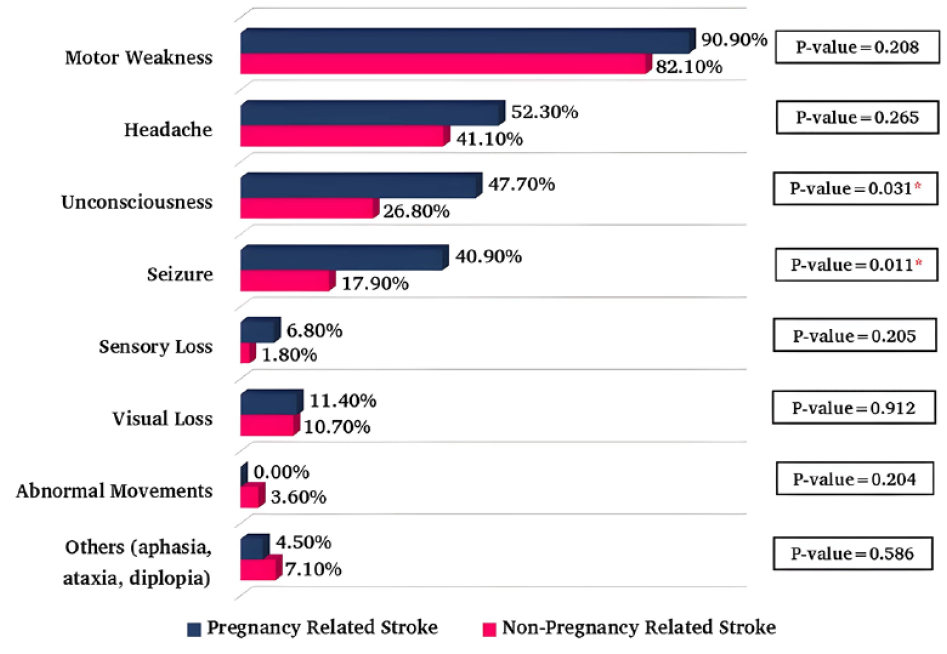
Clinical presentation of stroke in pregnancy and non-pregnancy (N = 1210).
Morbidity and mortality of stroke among females of reproductive years
MRS showed that most patients were severely disabled (score = 5) at their initial presentation in both the PRS and NPRS. But the long-term results for MRS patients showed a significant improvement, with 58% having no disability and 20% having a slight disability. Patients after a 6-month follow-up found that 93% had a favorable prognosis in terms of being alive and little to no significant disability with treatment, 5% died, and 2% left against medical advice. Comparing the two, the pregnancy-related group had a slightly higher death rate outcome than the NPRS (Table 4).
Disability, morbidity, and mortality of stroke in females of reproductive years (N = 1210).
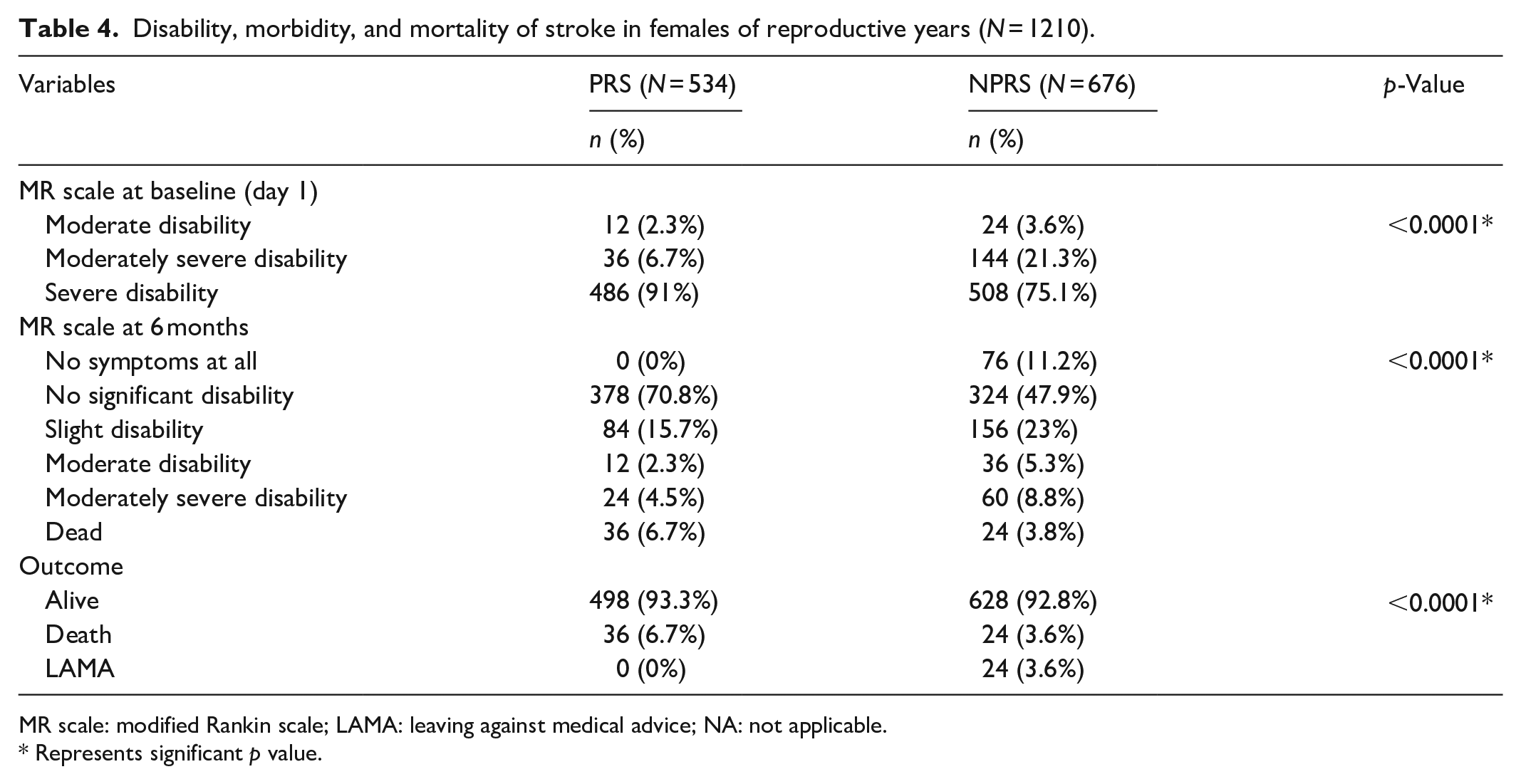
MR scale: modified Rankin scale; LAMA: leaving against medical advice; NA: not applicable.
Represents significant p value.
Discussion
This study compared stroke frequency, characteristics, and outcomes in pregnant and non-pregnant females in the tertiary care institutions of Karachi, Pakistan. Our investigation revealed a heightened prevalence of stroke among females within the reproductive age range (15–45 years), with a notable emphasis on the susceptibility of pregnant females aged 25–34 years compared to their non-pregnant counterparts, which was nearly equal in all age groups. In comparison, a meta-analysis of 11 studies by Swartz et al., 1 a review by Khalid et al., 11 and an original study by Prabhu 12 indicate that 0.03%–0.066% of pregnant females per 100,000 are susceptible to stroke worldwide at 22–34 years, about 2–3 times higher than in non-pregnant females. Our findings underscore the heightened risk in low-income countries like Pakistan, where limited healthcare and added stressors increase susceptibility during pregnancy, endangering both mother and child. In addition, our analysis found the frequency of NPRS (56%) is somewhat higher than the PRS compared to the prior studies which states stroke is more in pregnant females,1,11,12 highlighting the lack of attention devoted to the NPRS, which has not been the subject of prior studies, ultimately leading to the belief that pregnant women are at risk than non-pregnant women. This observation is particularly significant in low- or low- to middle-income settings like Pakistan, where women in their reproductive years play a crucial role in family dynamics. The patient’s previous medical history and stroke risk factors played some part in the stroke recurrence. However, a family history of stroke has no role in strokes that happen during pregnancy, but it contribute to strokes that happen outside of pregnancy,13–15 which was not uncovered by prior studies.13–18
Furthermore, our study shows that pregnant women are more likely to have a stroke during postpartum and in the last few months of their pregnancies. This agrees with a cohort study in England by Ban et al., 5 which found that the incidence of stroke is ninefold higher in peripartum and threefold higher in early postpartum. The Jeng et al. 18 study found that 67% of pregnant women had strokes in the third trimester and puerperium, which is associated increased demand, stress, and vulnerability in these periods.
In addition, females of reproductive years predominantly experienced arterial strokes, with two-third of arterial and one-third of venous strokes during pregnancy-related period, whereas non-pregnant women presented with almost exclusively arterial strokes. MCA was the most prevalent territory of stroke in both groups (52.4% and 76.9%), with non-pregnant females having greater propensity of multiple arterial involvements. Similar to our findings, Swarts et al. 1 and Grear et al. 19 reported a higher incidence of arterial strokes in pregnant women, and Yoshida et al. 20 discovered that 73% of PRS were arterial, with the MCA being the predominant site for stroke, attributable to its role as the largest artery of brain. The reason for the occurrence of arterial stroke in pregnancy arises from the hypercoagulable and hemodynamic state inherent to gestation, supported by our findings citing multiple etiologies,12,18 but since venous stroke constitutes a third of the portion of stroke underscores the need for neurologists to consider the possibility of venous stroke occurrences during pregnancy. Furthermore, the involvement of multiple arteries in NPRS can be related to large arteries due to the possibility of atherosclerosis 21 identified as a cardiac disease and HTN 22 among both groups as a risk factor. This observation holds significance as it delineates the distinction in stroke-affected regions between pregnant and non-pregnant women of Pakistan.
According to our study, weakness (86%) and headaches (46%) are the most common clinical manifestations of stroke in females of both reproductive years. By contrast, a meta-analysis by Ali et al. 23 revealed that headache 1.24 (95% CI: 1.11–1.39) and consciousness/mental status 1.38 (95% CI: 1.19–1.61) were more prevalent in women presented with stroke, whereas Jerath et al. 24 discovered that general weakness was the most common stroke symptom in 81.8% of women, aligning with our findings. According to our observation of Pakistani clinics, female patients with headaches and general weakness are misdiagnosed as having a psychiatric illness, migraines, flue, sleep disorders are not taken seriously, resulting in their subsequent arrival in the emergency room with severe deficit seizures and unconsciousness. Prioritizing a thorough assessment of these symptoms could enable early detection of strokes and spare families the anguish of suffering serious repercussions or disability.
In addition, our analysis demonstrates that infarction occurs in 88.8% of PRS patients, whereas in NPRS patients, infarction accounts for two-thirds and hemorrhages account for one-third, which contradicts the commonly observed higher prevalence of hemorrhages over infarctions in PRS reported in studies by Jeng et al. 18 and Yoshida et al. 20 discovered (33% and 25% infarction; 39% and 74% hemorrhages) in PRS. This stems from the higher prevalence of hypertension and cardiac issues in a low- to middle-income economy, as supported by our findings that eclampsia and cardiac diseases notably contribute to strokes in pregnancy, whereas strokes in non-pregnant individuals are more associated with cardiac diseases and hypertension. Several studies support these etiologies for PRS, such as Jeng et al. 18 report that 37% of women had eclampsia and 44% had cardiac diseases, Prabhu 12 presented that 73% of eclampsia patients had PRS, and Leffert et al. 17 demonstrated a 5.2 times higher susceptibility to stroke in pregnant females compared to non-pregnant counterparts. The above findings illustrate that cardiac problems and hypertension are the two main factors that should always be looked at in females of reproductive years to predict the chances of stroke and should be treated, due to the demands of their responsibilities and perhaps lack of awareness, the population in this geographical region is not adhering to lifestyle and dietary modifications aimed at mitigating the risk factors associated with stroke.
Furthermore, the majority of patients in both groups of reproductive years initially had severe disabilities; however, if treated effectively, the outcome was around 92%–93% with minimal casualties, which is consistent with the studies by Sanders et al. 13 and Liu S et al., 16 which show that if diagnosed and attention is paid to the rising cases of stroke in females of reproductive years, the chances of stroke can be reduced. Moreover, our study also revealed that although venous stroke initially resulted in more significant disability than arterial stroke, the prognosis for venous stroke was significantly better. This is owing to the fact that venous stroke symptoms respond more quickly to prompt anticoagulation medication, whereas arterial stroke symptoms linger for a longer duration, requiring a long-term therapy and significantly more care.
This study is an initiative to make changes in the prognosis for young female stroke patients. By establishing an early diagnosis and administering prompt therapy, the clinician can prevent stroke. Educating physicians and clinicians working in remote places where not all diagnostic modalities are available can lead to early inquiry and a quick diagnosis, hence improving the prognosis. General practitioners’ education sessions would play a crucial part in the improvement of prognosis. Furthermore, a simple investigation such as a CT scan of the brain, combined with knowledge of what can happen or what is the cause of stroke that occurs in a specific female of reproductive years, can help them decide which type of treatment would be best, which will lead to better quality of life.
Our study has limitations because the authors only had access to the databases and patients of five Karachi institutes, so some cases, might be missed when considering other institutes, but the results are generalizable as the five main busiest institutes were selected. Another limitation of this study is that the new stroke classification was not utilized due to limited data availability due to a lack of facilities and standardized diagnostic criteria in Pakistan relative to middle- to high-income countries. Also, the critical confounders (smoking, ethnicity, socioeconomic status, body mass index, prothrombin/activated prothrombin time, international normalized ratio) were unavailable for analysis from the database. Another limitation is that we did not use the National Institutes of Health Stroke (NIHSS) scale, which assesses acute stroke severity. Since our patients present at different times, usually after a delay or treatment from primary care hospitals, it was better suited to use the MR scale to identify stroke disability at different time frame. Another limitation is the use of convenient sampling technique, which was overcome by selecting five busiest and generalizable institutes. Lastly, the study did not account for home deliveries or people who cannot afford to go to the hospital for treatment. Our study’s strength lies in the fact, that it is conducted in busiest multi-institutes over an extended period in a low- to middle-income country, and being ambispective which gives it advantage over other studies which gives it an advantage compared to the many other studies discussed, that were retrospective and in developed economies. Our study shows a difference between two reproductive-year female groups that was not previously been accounted for, resulting in the novel findings and put more focus on both groups equally highlighting the lack of attention given to the largest populace of females who are non-pregnant. The sample size adequately portrays the results.
Conclusion
Our findings indicate a notable prevalence of stroke among females of reproductive age, with a slightly higher occurrence in non-pregnant individuals compared to pregnant ones. Stroke occurrence is significantly elevated in the 25–34 age group, a critical phase encompassing marriage, pregnancy, and childbirth in low- to middle-income countries. Presentation of strokes varies marginally between pregnant and non-pregnant females, emphasizing the importance of meticulous evaluation for optimal treatment. This underscores the necessity for ongoing medical follow-ups throughout the reproductive years to assess stroke risk and administer careful treatment, thereby reducing occurrence. Promoting year-round screening for stroke risk factors, including often-overlooked symptoms such as headache and weakness, is crucial for prevention, mitigating morbidity, and minimizing mortality. The study highlights the imperative for additional research, enhanced awareness, and a comprehensive approach to stroke in females of reproductive age, extending beyond pregnancy or exclusive focus on males.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121241242610 – Supplemental material for Evaluation of stroke in pregnant and non-pregnant women of reproductive years: A multicenter ambispective cohort study in a low- to middle-income country
Supplemental material, sj-pdf-1-smo-10.1177_20503121241242610 for Evaluation of stroke in pregnant and non-pregnant women of reproductive years: A multicenter ambispective cohort study in a low- to middle-income country by Muhammad Hamza Dawood, Kauser Mahmood, Mavra Roshan, Lailamah Rehman Sherani and Haseefa Perveen in SAGE Open Medicine
Footnotes
Acknowledgements
The authors like to show their gratitude to the above-mentioned institutes for their co-operation in conduction of the study. The author would also like to thank Dr. Syeda Zain from United Medical and Dental College for her initial help in data collection process but was not financially compensated.
Author’s note and authorships
Muhammad Hamza Dawood and Kauser Mehmood are first co-authors, Mavra Roshan is the second author, Lailahmah Rehman Sherani and Haseefa Perveen are co-third authors and have contributed equally to this study.
Authors contributions
MHD and KM are the guarantor of the study. MHD was involved in conceptualization, data curation, methodology, formal analysis, software, validation, writing—original draft, writing—review and editing. KM was involved in conceptualization, data collection and curation, investigation, methodology, supervision, writing—original draft, acquisition of ethical approval. MR, LRS, and HP were involved in data collection and curation, interpretation, visualization, writing—review and editing. All authors have approved the final version of manuscript for publication.
Data availability statement
The datasets generated or analyzed for this study are not publicly available due to the confidentiality promised to the participating members, but de-identifiable data are available upon reasonable request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional review board of United Medical and Dental College, Karachi, Pakistan (Ref. No: UMDC/Ethics/2021/04/08/286).
Informed consent
Written informed and verbal consent was taken from all the patients for their participation during the collection process. Verbal consent was obtained for the retrospective data collection in instances where patients were unable to physically present at the hospital and in prospective cases where participants exhibited limited literacy skills. For patients who were below 18 years, written consent was provided by their parents or legal guardians.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.