
Abstract
Objectives:
Care for patients after stroke has been transformed over the last two decades. We explored one patient-centred outcome: the type and range of questions asked after stroke through a publically available helpline. We compared data from 1990 to 2013 to see whether the positive changes in stroke care are reflected in the types and quantity of inquiries from patients and their families.
Methods:
All of the inquiries received by the UK Stroke Association helpline between 1 April 2013 and 31 March 2014 were collated and compared to the data collected and previously reported by Hanger and Mulley between May and September 1990.
Results:
In 1990, the most common inquiry was for more information about stroke (22.5% (429/1908)). In 2013, the most common question remained the same, with 25.4% (2601/10,233) of all callers asking what is a stroke. Specific medical questions increased from 4.2% (80/1908) in 1990 to 10.5% (1074/10,233) in 2013. Queries about support with home care reduced from 9.4% (180/1908) in 1990 to 2.6% (257/10,233) in 2013. Questions about recovery and rehabilitation were frequent in both 1990 (11.1% (212/1908)) and 2013 (13.2% (1353/10,233)).
Conclusion:
The transformation in stroke services has not been reflected in this patient-level outcome in the United Kingdom. Many stroke survivors and their families still struggle with understanding their condition and treatment options.
Introduction
Over the last two decades, stroke care has been completely transformed with the introduction of stroke units,1,2 implementation of early supported discharge teams, 3 and stroke clinical guidelines covering the whole stroke pathway from hyper-acute care to longer-term rehabilitation.4–7 Key features of stroke unit care include clinical leadership from a physician specialist in stroke care and the input of a skilled multi-disciplinary team. 2 We sought to explore whether these changes in stroke care had impinged on one patient and family centred outcome, their concerns and perceived needs as reflected in the type and quantity of inquiries from patients and their families to a public helpline in the United Kingdom.
The Stroke Association is the major charity for stroke in the United Kingdom, formerly the Chest, Heart and Stroke Association; it has been established for over 50 years. In 1990, Hanger and Mulley 8 explored the inquiries made to the Stroke Association helpline.
The purpose of this article is to compare the UK Stroke Association helpline data from 2013 to that reported in 1990 to see whether the transformation in stroke care services over the past two decades is reflected in the expressed concerns and perceived needs of stroke survivors and their families.
Methods
The UK Stroke Association has a long-established advisory service. In 1990, the service operated through geographically distributed Advice Centres and received inquiries by telephone, letter and in person. For the purposes of the Hanger and Mulley 8 article, inquiries were logged onto a paper proforma documenting information on the source of the inquirer, the type of inquirer, the sex and age of the stroke survivor and the subject of the inquiries, which were grouped into 35 categories. In 2013, the national helpline operated from its’ Life after Stroke centre in Bromsgrove, England and inquiries were received by telephone, letter, email and via social media. Data on all of the inquiries received were logged onto a database and included, where available, information on the source of the inquiry, the type of inquirer and the inquirers’ sex. Information on the subject of the inquiry were logged and placed into one of 33 pre-defined categories.
Hanger and Mulley 8 reviewed all data sheets which recorded stroke-related inquiries made to the Stroke Association Advice Centres over an 18-week period of time between May 1990 and September 1990. In 2013, data on all inquiries made between 1 April 2013 and 31 March 2014 were reviewed. The categories of the inquiries made in 2013 were matched to those recorded in 1990 where possible and the frequency of inquiries compared between the two time points. All helpline data are recorded anonymously and only aggregated data were passed to the authors. Ethical approval was not required for this study.
Results
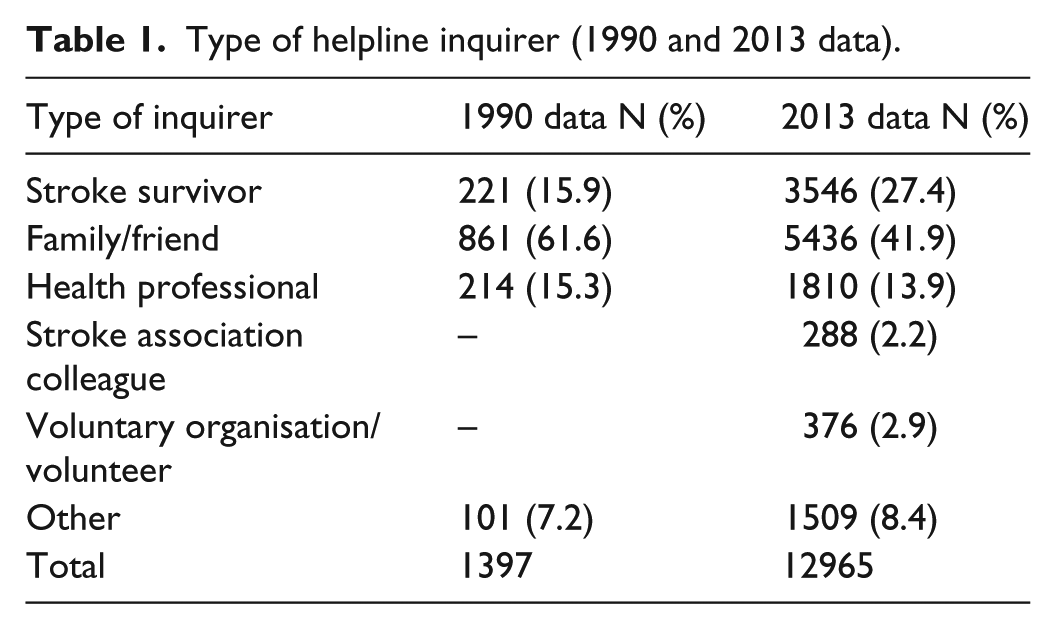
In 2013, a total of 19,674 inquiries were made between the 1 April 2013 and the 31 March 2014. In 1990, 1908 inquiries were made over an 18 week period between May 1990 and September 1990 (estimated 5512 if extrapolated to 1 year). The majority of inquiries in 2013 were made by telephone (65.9% (12,958/19,674)) or email (29.9% (5873/19,674)). In 1990, the majority of queries were made by telephone (data not reported). Data on the inquirer type was available for 65.9% (12,965/19,674) of all inquiries in 2013. Most inquiries were made by the stroke survivors’ family/friends (41.9% (5436/12,965)), by the stroke survivor themselves (27.4% (3546/12,965)), or by health professionals (13.9% (1810/12,965)) (Table 1). In 1990, the vast majority of queries were made by the family and friends of the stroke survivor (61.6% (861/1397)), with fewer calls made by the stroke survivor themselves (15.9% (221/1397)) (Table 1). For the 2013 data, the sex of the inquirer was available for 65.7% (12,922/19,674) of all inquiries. The majority of inquirers were female (68.4% (8837/12,922). In 1990, data were collected on the stroke-survivors sex (not that of the inquirer). Less than half (45.4% (506/1114)) of the stroke survivors were female.
Type of helpline inquirer (1990 and 2013 data).
In 2013, data on the subject of inquiries was available for queries made by telephone. In total, 12,958 telephone calls were made to the Stroke Association helpline; however, due to telephony arrangements, the subject of inquiries was only recorded in 10,233 (79.0%) of calls. Table 2 presents the subject of the inquiries that were made. The largest number of queries asked ‘What is a stroke’ (25.4% (2601/10,233)).
Subject of helpline inquiries (1990 and 2013 data).

OT: occupational therapy; GP: general practitioner.
Including: What is a stroke/tell me about stroke/will I get better.
Including: before and after a stroke.
Including: recurrence risk and role of diet in prevention.
Moved from community care category in 1990, to fit 2013 category.
The most common query in 1990 was also for general information about the stroke (including what is a stroke/tell me about stroke/will I get better) (22.5% (429/1908)). Specific medical questions were the next most common query in 2013 (10.5% (1074/10,233)), these were less common in 1990 (4.2% (80/1908)). In 2013, questions about accessing therapy (speech and language, physiotherapy, occupational therapy/aids/adaptations, and private treatment) made up 8.4% (856/10,233) of all calls and queries about recovery and recovery timescales made up 4.9% (497/10,233) of calls. In 1990, 6.0% (116/1908) of calls related to recovery/rehabilitation including access to therapy, and 5.0% (96/1908) to practical advice and aids.
In 1990, after general stroke information, the next most common question was about support available for home care (including concerns about ability to cope and a lack of support services) (9.4% (180/1908)), in 2013 queries relating to this issue were less common (2.6% (264/10,233)). Similarly, in 1990, 9.2% (175/1908) of calls asked about stroke clubs, but in 2013 only 2.5% (257/10,233) of queries asked about these.
Discussion
Almost 20,000 inquiries were made to the Stroke Association helpline in 2013, with the majority of calls made by the stroke-survivors’ family/friends or the survivors themselves. In addition to the change in stroke services, there has been a huge expansion of information platforms through the Internet and social media over the last two decades, yet nearly 20,000 people contacted the helpline in 1 year. Almost two-thirds of inquiries were made by phone and one-third by email. The predominance of phone calls may reflect the fact that the helpline is mainly advertised as a telephone line, but may also suggest that many stroke survivors and their families desire the personal contact and support that the phone line provides. The Stroke Association also hosts a website forum (TalkStroke), and it would be interesting to see whether the types of inquiry made in the forum are different to those made to the helpline. The Stroke Association helpline clearly plays an important role in providing support to a large number of stroke survivors and their families in the United Kingdom.
Despite the transformations in stroke care over recent years, the most common question received by the Stroke Association helpline remains the same in 2013 as in 1990 with a quarter of all callers asking for information about what is a stroke. Queries relating to specific medical questions increased in number from 1990 to 2013, while fewer calls were made about coping at home and accessing support services in 2013 compared to 1990.
Although stroke care is now primarily delivered by multi-disciplinary teams with expertise in stroke, some stroke survivors and their families remain sufficiently uncertain about the nature of stroke to contact a national helpline. These findings confirm previous literature9,10 that many stroke survivors and their families still do not have sufficient understanding and knowledge about their stroke and recovery. It is difficult to be certain whether this represents a true absence of knowledge or whether asking for information is seen as a ‘gateway’ question to begin dialogue. Stroke survivors and their close family/friends may receive information about their stroke from health professionals while in hospital; however, the stress of the situation may mean that this information is not understood or is forgotten. The Stroke Association helpline may be viewed as a neutral, non-threatening and trustworthy source of information and asking for more information about stroke may provide an opportunity to discuss other problems.
A Cochrane review on information provision after stroke indicates that rather than simply handing out information, a more educational approach to information provision where opportunity is provided to reflect, discuss and ask questions may more successfully address stroke survivors and their families concerns. 10 Knowledge of stroke in the general population as a whole is poor. 11 A population approach to education about stroke would help to ensure a better understanding of stroke prior to being affected by one.
The implementation of early supported discharge and specialised community services may allow for a smoother, well supported, transition home from hospital for some stroke survivors and their families, thus impacting on the support service queries, although not all stroke survivors have access to these services in the United Kingdom. 12 However, queries relating to recovery and access to therapy were frequent in both 1990 and 2013. Many stroke survivors and their families continue to express a need for access to more therapy for longer and for support from Stroke Association services. The feeling of abandonment on discharge from hospital and/or once therapy services withdraw has been reported previously 13 and is acknowledged in policy, but is still not sufficiently addressed. This issue may be resolved by giving stroke survivors the skills and ability to self-manage their own recovery and rehabilitation before the therapists withdraw their services and ensuring that the stroke survivors and their families are aware of, and have access to, other existing long-term support services such as those provided by the Stroke Association and other relevant support/exercise/aphasia groups.
Strengths and limitations of the research
The work presented provides an opportunity to review independently collected data from two distinct time points, reflecting the queries that stroke survivors and their families have about their condition.
Unfortunately, the helpline does not collect information on the time interval between the stroke and the inquiry being made. The needs of stroke survivors and their families may change over time and understanding the types of inquiry made at different times post-stroke would help health professionals target needs appropriately.
The data present the concerns of stroke survivors and their families who have actively identified a problem and sought out help using the Stroke Association helpline. Other issues may be under-represented by these data as some issues may be difficult to verbalise and others (such as sex/incontinence/emotional issues) may be too personal to actively raise and discuss via a helpline. The needs of stroke survivors with aphasia and/or cognitive impairments may be under-represented here as accessing a helpline by phone or email would be difficult for these individuals. This would explain the small number of queries relating to speech difficulties and access to speech and language therapy reported in this study despite up to one-third of stroke survivors being affected by language impairments. 2 In addition, some of the differences reported between 1990 and 2013 may, in part, be due to changes in the way that queries were coded and categorised between the two time points. Nevertheless, this study reflects the concerns of over 10,000 stroke survivors and their families across the UK, and the 2013 data provides a comparison to the concerns raised 20 years previously.
Conclusion
The vast improvements in stroke service provision over the last two decades are not reflected in the expressed concerns and perceived needs of stroke survivors and their families. In 2013, as in 1990, substantial numbers of stroke survivors and their families struggle to understand their condition and treatment options. For stroke services to successfully address the informational needs of stroke survivors and their families, innovative and sustained methods of delivery are required along with careful monitoring of outcomes to ensure that needs have been addressed.
Footnotes
Acknowledgements
The authors are grateful to the Stroke Association Helpline team and in particular to Sian McClure, for providing us with the helpline data and for commenting on a draft of this article. Thanks to the reviewers of the first draft of this article for their helpful comments that have contributed to the discussion of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This publication presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Grant Reference Number RP-PG-0611-20010). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.