
Abstract
Benign and malignant orbital tumours develop from the orbit or invade it from the surrounding tissues. Ocular melanoma is a rare but potentially devastating malignancy arising from the melanocytes of the uveal tract, conjunctiva, or orbit. The poor overall survival depends mainly on its high metastatic rate. Signs and symptoms are variables mainly depending on the size of the tumour. Its treatment consists generally of surgery, radiotherapy or both. We report a case of a patient suffering from unilateral blindness for the last 10 years with a recent swelling of the orbit. The pathological analysis described a uveal melanoma. The patient benefitted from a total orbital exenteration with reconstruction using a temporal flap. Thereafter, the patient received adjuvant radiotherapy and immunotherapy. The patient was in complete remission. No recurrence was highlighted after 2 years of follow-up.
Introduction
Benign and malignant orbital tumours develop from the orbit or invade it from the surrounding tissues. 1 Orbital tumours can have different origins and histological types. 1 These tumours have a broad spectrum of behaviours and prognoses depending on the type of tissue structure. 1
Primary orbital melanoma (POM) and ocular melanoma are two distinct entities. The aetiology of the POM is still unclear. 2 It is thought to arise from melanocytic cells of the leptomeninges or ciliary nerves, or ectopic intraorbital nests of melanocytes. POM can occur ‘de novo’, but it is often reported in association with pigmentary changes within periocular tissues (such as nevus of Ota, blue cellular nevus or oculo-dermal melanosis). 3 Ocular melanoma is a rare but potentially devastating malignancy arising from the melanocytes of the uveal tract, conjunctiva or orbit. 4
Several signs and symptoms have been observed such as visual disturbance, diplopia, pain, and proptosis. They are essentially a consequence of the size of the tumour. The diagnosis is based on tissue analysis. Its treatment consists generally of surgery, radiotherapy (RT) or a combination of both. Due to the scarcity of this pathology, the existing literature has few treatments proposal or outcome-related conclusions. Therefore, we report the case of an orbital mass with a total loss of vision.
Case presentation
A 68-year-old man was referred to the department of oral and maxillofacial surgery of the CHwapi hospital, for an orbital mass. The patient was complaining of swelling in the right orbit for the last 3 weeks. The patient was suffering from blindness of the right eye for 10 years. The patient did not look for medical counselling until this point. The clinical examination highlighted a right orbital mass. Conjunctival tissue with neovascularization covered the mass. The sclera was observed in the external part. No other ocular structures were identifiable. A movement of the components of the right orbit to the left was possible. No other extra-ocular movement was seen. The skin and the eyelids were not clinically invaded. The conjunctiva sac was recognizable. The rest of the head and neck examination was normal. No cervical lymph nodes were palpated.
A computed tomography (CT) scan (Figure 1), a magnetic resonance imaging (MRI) (Figure 2), a positron emission tomography–computed tomography (PET-CT) (Figure 3) and a biopsy, under general anaesthesia, were carried out to complete the workup. The MRI highlighted a solid mass (46.5 × 32 × 31.5 mm) with moderate contrast uptake without a liquid component, with small calcifications. The lesion, mainly intra-conal, included an atrophic and heterogeneous eyeball, pushing back the adjacent structures without moulding them. The CT scan did not observe bony or extra orbital invasion. The PET-CT underscore the malignant activity of the tumour. Furthermore, a small hypermetabolic mass was detected in the abdomen. The biopsy was realized through the conjunctival sac. The pathological examination suspected a primitive or metastatic malignant melanoma.

CT scan, axial.

MRI, axial.

PET-CT, coronal.
After all the results, the head and neck multidisciplinary evaluation in oncology decided that the treatments should be a radical surgery, followed by RT and immunotherapy.
A total orbital exenteration was performed with both eyelids and coronal approaches (Figures 4 and 5), in September 2020. The resection consisted of the entire orbital components through a sub-periosteal dissection (Figure 5). A temporal flap was raised to close and isolate the orbit (Figure 6) with a lateral orbitotomy. The eyelids were closed on themselves. The postoperative course was uneventful. The drains were removed on day 2 and day 3. The patient was discharged on day 4. The final anatomopathological analysis showed an epithelioid malignant melanoma presumably of primary choroidal type occupying the posterior chamber of the eye infiltrating the periorbital adipose tissue and the posterior orbital muscles. It was classified pT4e. Immunophenotyping showed a limited 10% positivity of malignant melanocytic cells for the S100 marker and a 100% positivity for the melanocytic marker SOX10. The oncoprotein P53 was not expressed. The KI67 proliferation index was very heterogeneous (15→25%). The mitotic index evaluated by phosphohistone-3 remained low-grade (9 mitoses per 10 high-power fields). BRAF V600 immunostaining was negative. Pictures of the microscopic view of the tumour are seen in Figure 7.
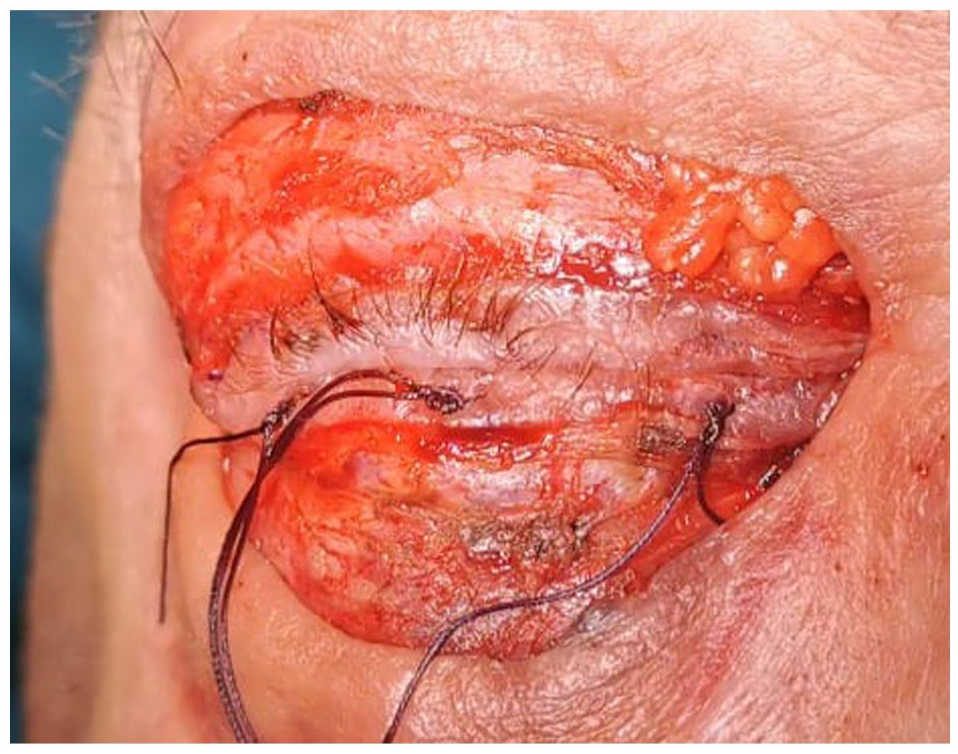
Eyelid incision.

Coronal incision and subperiostal dissection.

Temporal flap.

Tumour’s pictures. (a) Melanic pigment. (b) COX10 histological staining.
Thereafter, the patient received adjuvant RT and immunotherapy in another hospital (Epicura Hospital, Baudour). RT was performed for 6 weeks, from November to December 2020. A 2 Gy dose every 30 sessions was given in the orbit using volumetric arc therapy (VMAT) (3 fields VMAT and daily check position by image-guided radiotherapy (IGRT) (CBCT). Images of the radiotherapy treatment, and the sparing of the organs’ irradiation are seen in Figure 8. A clinical control 1 month after the end of RT showed no toxicity of the treatment. The patient received nine cures of Pembrolizumab, from January 2021 to February 2022. The immunotherapy was stopped because the patient suffered of an obliterating arteriopathy of the lower limbs. The tolerance was very good before this event.

Images of radiotherapy treatment.
A Pet-CT is done annually. He was seen every 3 month the first year and every 6 month the second year. He is still free of disease for now.
Discussion
Primary orbital melanoma is very rare, with approximately 50 cases reported to date. 3 In this case, this diagnosis has not been considered. The tumour seems to come from the posterior part of the eyeball, to invade the surrounding structures. Therefore, the first diagnosis is that of uveal melanoma, which slowly invades the orbit. Ocular melanoma mainly arises from the uveal tract (choroid, iris or ciliary body). 4 Uveal melanoma is more commonly seen in older age groups, with peak incidence at the age of 70 years. 5 Skin colour, hair colour, tan ability, and oculodermal melanocytosis are susceptibility factors, and BAP1 mutation is a predisposing factor. 5 However, sunlight exposure and intermittent exposure to ultraviolet light have not shown any implication for the development of uveal melanoma. 5
The care of this affection depends on the size of the lesion, and therefore the ability to preserve the eyeball and the vision. Radiotherapy is essential in the cure of these tumours. It should be considered as one of the main therapeutic options for local control to try and preserve vision and reduce side effects. 6 Some series have even 98% rates of local tumour control. 4 In recent years, other eyeballs–sparing techniques have become more widespread such as photocoagulation, trans-pupillary thermotherapy, chemotherapy, immunotherapy, and stereotactic radiosurgery. 7
In the current case, radical surgery was performed due to the tumour size and the subsequent vision loss. A total orbital exenteration including the eyelid border was realized. Nevertheless, the bony walls of the orbit were spared. The absence of a bony lesion on the CT scan, the absence of meningeal enhancement and the well-encapsulated appearance on the MRI were not in favour of the upper bony wall resection. The orbital nerve was cut at the apex of the orbit, after clipping the orbital artery.
Many reconstructions have been described, from spontaneous granulation to free flap rehabilitation. 8 The reconstruction aims to isolate the orbit from the nasal cavity, the paranasal sinuses, and if needed the brain. 1 A closed cavity reconstruction, using a temporal muscle flap, was chosen to restore the orbit volume and to have a greater tolerance to adjuvant RT. Indeed, Skinner et al. 9 reported a 5-year local recurrence rate of 22% for patients who received postoperative RT compared with 73% for those who did not. The technique of VMAT (modulated arc therapy) with protons was considered for this patient as a preferred treatment because there was no critical organ at risk in the direct region of the radiation field. The fact that the right eye was removed, together with the right optical nerve and that the tumour bed was situated very superficially without any organ at risk in direct contact was considered as an unrecommended indication for proton therapy.
Prosthesis rehabilitation with an epithesis has been discussed with the patient, during the care and the follow-up. Literature is inconsistent about the metastasis rate at the time of diagnosis. Some authors say that distant metastases are rare at the time of initial ocular presentation, occurring less than 5% of the time. 4 Others say that this cancer is known to metastasize before it is diagnosed. 10 But everyone agrees that about 50% of patients will suffer and die from this condition. In the current case, an abdominal nodule with hyper-metabolic activity was detected. Unfortunately, the biopsy confirmed to be a metastasis of the orbital melanoma. Nevertheless, the orbital surgery was realized before the diagnosis of the lesion, to have local control regardless of the pathology’s extension.
In metastatic uveal melanoma, various treatments have been tested: systemic chemotherapy, immunotherapy, targeted agent against the MAPK pathway, and liver-directed therapies. However, response rates are generally less than 10%, and no therapy has been shown to improve overall survival. 11 These results are inconsistent with the one observed with cutaneous melanoma. A recent prospective study from Fountain et al. 12 showed 80% of patients disease-free at 3 years compared with 50% for historical controls with the use of ipilimumab. Notwithstanding, only 10 patients were included in the study. Furthermore, the results were not statistically significant. A control PET-CT showed a total remission after five cures of Pembrolizumab. The patient finished the immunotherapy after eight cures of Pembrolizumab. No recurrence was observed after a 2-year follow-up.
Conclusion
Uveal melanoma is a rare but deadly disease. The poor overall survival mainly depends on the high metastatic rate of this pathology. Aetiology remains unclear, but it has a different origin from cutaneous melanoma. The treatment options are essentially surgical resection or RT (depending on the tumour size and the ability to preserve the eyeball and its functions). Until now, the different systemic treatments have not shown significant improvement in overall survival. However, many encouraging clinical trials on metastatic uveal melanoma are in progress.
Footnotes
Author contributions
L.M.: data collection, data analysis, manuscript writing
R.A.: data collection, data analysis
B.C.: manuscript revision,
S.A.: manuscript revision, data analysis
S.C.: manuscript revision
G.S.: manuscript writing, manuscript revision, responsible for the integrity of the data analysis
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.