
Abstract
Supernumerary teeth and taurodontism are both common dental anomalies when found as isolated entities. However, simultaneous presence in the same individual without a syndrome is rarely reported in the literature. This case report describes a 20-year-old non-syndromic male with multiple supernumerary teeth in association with multiple molar and premolar taurodonts and no family history of genetic predisposing factors. Taurodontism was measured and confirmed through cone-beam computed tomography for accuracy of the classification. Early diagnosis with the aid of radiographic imaging and persistent follow-up are crucial to treatment.
Introduction
Supernumerary teeth (ST) or hyperdontia refers to the presence of teeth additional to normal dentition. The prevalence of the condition varies in relation to different racial groups, ranging from 0.1% to 3.2% in permanent dentition, 1 with the highest prevalence in Asian and African populations. 2 Although the factors responsible for the morphogenesis of ST remain unknown, the most widely accepted theory is hyperactivity of dental lamina, influenced by environmental and genetic factors. 3
A multiplicity of supernumeraries is predominantly associated with developmental disorders or syndromes such as cleidocranial dysplasia or Gardner syndrome, and its presence as an isolated entity is rare. The most common location for multiple ST is in the mandibular premolar region.1,4
Taurodontism, as introduced by Keith, 5 is the tendency for the body of the tooth to enlarge at the expense of the roots. 5 This has been reported in a wide range, from 0.1% to 48%, depending on racial factors and the diagnostic criteria used. 6 Molars are the most affected teeth, but taurodontic premolars have also been reported in the literature. 7 In these cases, diagnosis is usually difficult with conventional radiographic imaging, as this only depicts the tooth in the mesiodistal dimension. 6
In general, a tooth is considered to be taurodontic if the distance from the cemento-enamel junction (CEJ) to the highest point of the pulp chamber floor is greater than 2.5 mm. According to Shifman and Chanannel’s Taurodontism index (TI), when the distance between the highest point of the pulp chamber floor and the lowest point of the pulp chamber roof, divided by the distance of the second to the root apex, multiplied by 100, is equal to or greater than 20, the tooth is considered to be taurodontic. 8 Depending on the above measurements and the extent of the condition, taurodontism is classified as hypo-, meso-, and hyper-taurodontism, as Shaw described. 9 The techniques used to diagnose and classify taurodontic teeth are based on either external morphological criteria or periapical and posterior bitewing radiographs.
Taurodontism pathogenesis remains unclear, but it could be due to a delay in the calcification of the pulp chamber, 10 as well as an odontoblastic deficiency and an alteration in Hertwig’s epithelial root sheath. 10 It could be associated with developmental anomalies and syndromes such as cranioectodermal dysplasia, 11 Down Syndrome, 12 and Klinefelter Syndrome, 13 but is mostly an isolated anatomic variant. 6
The literature is scarce when it comes to the relation between hyperdontia and taurodontic teeth without the involvement of syndromes, such as otodental dysplasia. 14
This report presents a case of a healthy, syndrome-free patient with multiple supernumerary and hyper-taurodontic molar and premolar teeth.
Case report
A 20-year-old male patient from the Nigerian Igbo tribe presented to the Dental Clinic of the European University Cyprus to seek aesthetic treatment for a fractured incisal edge on tooth No. 11 due to past trauma and mild discomfort in the lower right posterior region.
Familial and medical history were free of pathological findings and extraoral examination was within normal limits.
Intraoral examination revealed hyperpigmented labial mucosa and traumatically irritated buccal mucosa, correlated with the partially impacted teeth No. 38 and 48, rotated tooth No. 44 and a bulge lingual to teeth No. 44 and 45 (Figure 1). Differential diagnosis was torus mandibularis, odontoma, peripheral fibroma, or undiagnosed unerupted supernumerary tooth.

Intraoral photograph, right mandibular occlusal view of rotated tooth No. 44 and bulge lingual to teeth No. 44 and 45 that was later radiographically diagnosed to be due to partially impacted para-premolar.
Cold sensitivity test was performed on teeth No. 11, 44, and 45, and all teeth were found to be vital.
Orthopantomography (Figure 2) and periapical radiographs (Figure 3) revealed an impacted supernumerary para-premolar in the area of teeth No. 34–35 and a partially impacted supernumerary para-premolar in the area of teeth No. 44–45 and two impacted supernumerary distomolar teeth in the areas distal to teeth Nο. 18 and 38. In the same radiographs, taurodontism was evident in most maxillary and mandibular molar teeth.

Orthopantomography of the patient shows two supernumerary mandibular para-premolars and two distomolars in the upper right and lower left regions. In addition, bilateral maxillary and mandibular taurodontism is present, in teeth No. 18, 17, 27, 28, 38, 37, 47, and 48.

Periapical radiographs of molars for all quadrants ((a)–(d)), acquiring measurements for the calculation of the TI:
The patient was informed about the findings, and a cone-beam computed tomography was taken (Figure 4) to reach a more accurate diagnosis.
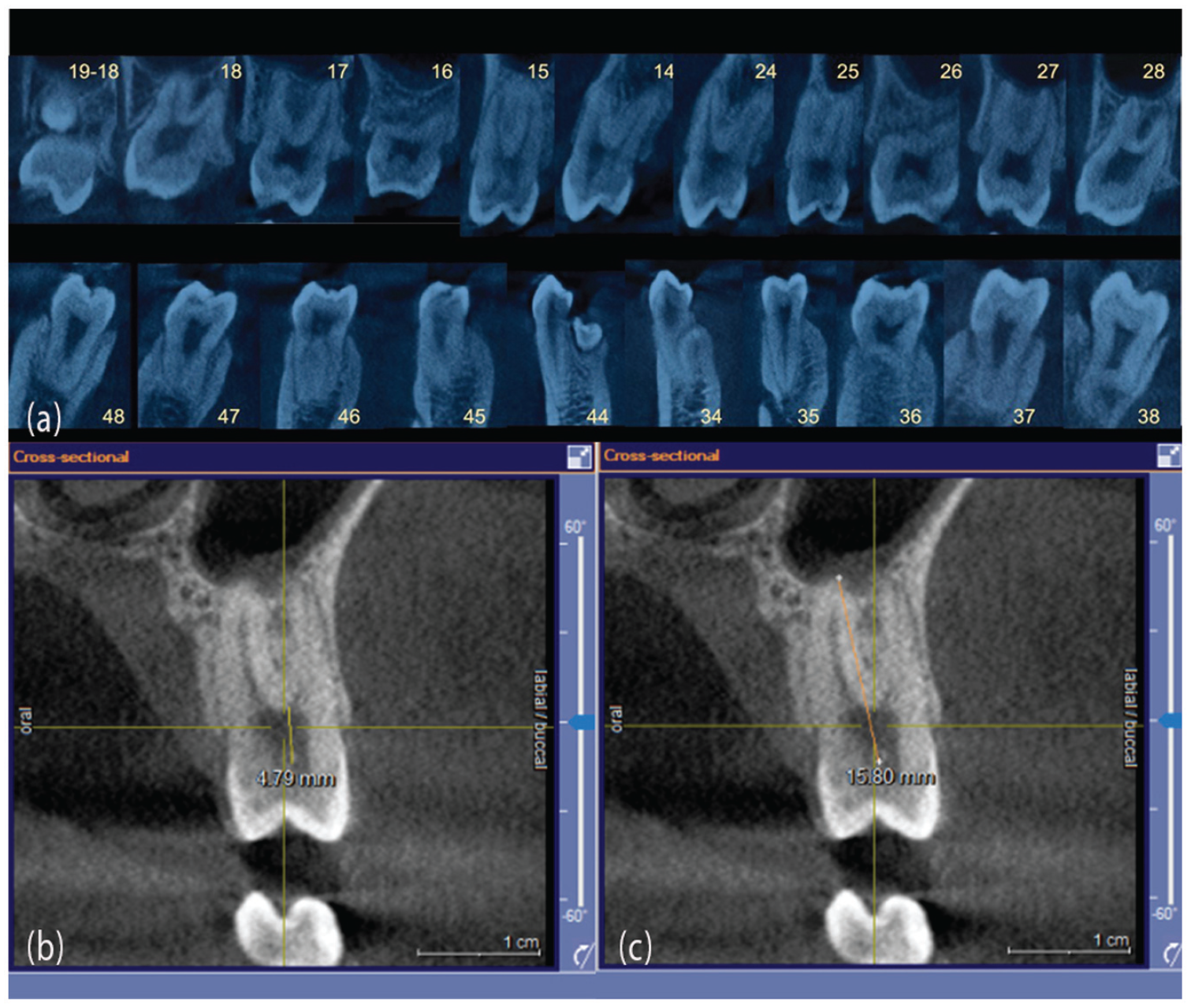
CBCT images. (a) cross-sectional view of all posterior teeth. Upper right distomolar (19), lower left para-premolar near tooth No. 34, and lower right para-premolar, erupting lingually of tooth No. 44. (b) cross-sectional view of tooth No. 15, shows V1 measurement. (c) cross-sectional view of tooth No. 15, shows V2 measurement.
The formed treatment plan included extraction of all third molars and supernumerary upper right and lower left distomolars, extraction of the lower right para-premolar, and monitoring of the lower left para-premolar. In addition, a class IV composite resin restoration was planned to restore the fractured tooth No. 11.
TI was applied on all posterior multi-rooted teeth, and further subdivision was performed, according to Shaw’s classification (Table 1).
Results from periapical, orthopantomography, and CBCT radiographic measurements.

CBCT: cone beam computed tomography; TI: Taurodontism index.
Depending on the TI, taurodontism (>20) is subclassified as hypo-taurodontism (20–30) in green, meso-taurodontism (30–40) in blue, and hyper-taurodontism (40–75) in red. Numbers lower than 20 are without color. (–) indicates teeth that cannot be measured using the corresponding radiographic images.
Discussion
This report of a non-syndromic young male patient with a rare presence of multiple taurodontic and ST calls attention to the uncommonness of the relationship.
The prevalence of ST appears to be low in most populations, and most of these teeth are reported in patients from Asian or African origins such as Nigeria. 2 They are more frequently found in the anterior maxilla as mesiodens, 1 but in cases with multiple ST, para-premolars are the most common; 75% of the supernumerary premolars are impacted, and while the majority appear to be asymptomatic, mandibular supernumerary premolars commonly have a marked tendency to form cysts or other pathological changes.4,15 In the present case, two impacted mandibular para-premolars were found, one in the right premolar region and one in the left premolar region, as well as an upper right and a lower left distomolar.
Recent studies show increased taurodontic prevalence around the globe, with the second and third molars being more prone than other teeth. 6 In a study of 19.146 molar and premolar teeth of the north Indian population, only 4 teeth were found to be taurodontic premolars. 16 In this report, four maxillary premolars were found to be taurodonts, with tooth No. 15 being a meso-taurodont and teeth No. 14, 24, and 25 hypo-taurodonts.
The diagnosis of taurodontism is usually a random finding, made through routine two-dimensional (2D) radiographic imaging such as periapical or orthopantomography, but these techniques may not be adequate to accurately classify the condition due to possible distortion, leading in turn to inaccurate measurements. 17 In our study, cone beam computed tomography (CBCT) imaging was considered to be appropriate for proper diagnosis and preparation for surgical extractions, to evaluate the proximity of the teeth to anatomical structures such as the inferior alveolar nerve, to evaluate the remaining lingual bone next to the lower right para-premolar and its proximity in the bucco-lingual dimensions to teeth No. 44 and 45. As the CBCT was available, it was used to research differences in taurodontism classification with different imaging techniques. This may serve as a pilot study for further research.
Discrepancy in measurements is found between the three most used imaging modalities, periapical, orthopantomography, and CBCT. For instance, teeth No. 16 and 46 were not depicted as taurodonts on 2D imaging but were through measurements on CBCT. Similarly, teeth No. 15 and 25 were shown to be two rooted, allowing the application of TI in the cross-sectional view. Two rooted second maxillary premolars is a common finding, 7.6%–20.4%, depending on the population.18–21 However, in this report it is evident that many times two rooted second maxillary premolars may not be detected with 2D imaging techniques while the two rooted morphology is clearly shown on CBCT imaging. Orthopantomography is highly distorted, with structures lying outside the focal trough appearing as shadows and artifacts. Furthermore, they have high magnification errors of up to 10%–21%, 22 while CBCT scans are significantly more accurate, having an error of only around 1%–2%. 22 Periapical radiographs performed using paralleling techniques, which pose issues with angulation errors, making measurements taken appear either larger or smaller than reality. 22 This was also evident in our results, as measurements made through periapicals were lower than those taken from orthopantomography and CBCT (Table 1).
Simultaneous presence between hypodontia and taurodontism appears in several studies,23,24 while the one between hyperdontia and taurodontic molars and premolars is limited to case reports.7,25 Studies where multiple populations were investigated, reported that hyperdontia and taurodontism existing simultaneously was statistically insignificant.23,24
In a Turkish population study, the existence of a relationship between hyperdontia and taurodontism was investigated, and taurodontism was the most common dental anomaly to be found in hyperdontia patients. Hyperdontia was found in 21 out of 2340 patients, and taurodontism coexisted in 10 (48%) of these 21 cases. 26
In another study that investigated the association between taurodontism with numerical dental anomalies, 45 patients out of 164 presented with ST and only 12 patients had a simultaneous presence of taurodontism and ST. The association was described as weak by the authors. 24 In a controlled study by Baccetti, ST appeared to be a separate etiological entity with respect to other anomalies that were examined, including taurodontism. 27
The presence of multiple supernumeraries can create several clinical challenges, such as crowding, delayed eruption, rotation, diastema, resorption of adjacent teeth, and oral cyst pathologies. 1 Conflicting opinions exist about the management of ST, particularly the timing of removal, if necessary, at all. 2 Some authors agree that removal of ST that are not associated with pathological conditions or are not creating a problem to the adjacent permanent dentition is unnecessary treatment.28–30 In this case, the decision to extract all third molars and supernumerary upper right and lower left distomolars was based on the irritation caused by the patient’s persistent biting on the operculum covering teeth No. 38 and 48 due to crowding in the lower jaw. In addition, the CBCT scans revealed contact between tooth No. 18 and the upper right distomolar, justifying their extraction. The lower right para-premolar was also advised to be extracted due to its unfavorable eruption pattern and crowding. Khalaf et al. 4 suggest that if a supernumerary premolar is erupting or is crowded after eruption, removal should be undertaken to relieve the crowding and/or avoid occlusal discrepancies. Finally, CBCT imaging did not reveal any pathology or problem associated with the still forming lower left para-premolar, so it was justified to be left and monitored with yearly radiographic examination until completion of root development, unless it erupts or becomes symptomatic in which case it also should be extracted.
Taurodontism, on the contrary, is implicated endodontically, as altered canal configuration can occur, and a higher potential for added canal systems pose challenges for treatment. 6 Prosthodontic and orthodontic work is negatively affected as well in taurodonts due to the lack of stability of these teeth, making them poor candidates for anchorage purposes. 6 Therefore, prevention and follow-up yield the best prognosis when it comes to taurodontism, in the sense of minimizing the potential problems associated with any treatment needed on these teeth. For example, as a taurodont with periodontal disease would be lost faster in comparison with a non-taurodont due to the lower stability offered by its roots, it would be more important to apply proper oral hygiene measures and regular scaling and root planning. Also, the application of proper caries risk management and prevention, in order to avoid the risks of an endodontic treatment failure.
Conclusion
Thorough clinical examination, complemented by indicated radiographic imaging, should always be performed during the initial examination of a patient. In cases where more details are needed for accurate diagnosis and treatment planning, the use of CBCT may be indicated. Early diagnosis, along with appropriate treatment planning and monitoring are of particular importance so that the different implications following these anomalies can be minimized and prevented. TI measurements, compared with different radiographic modalities, can serve as a pilot study for further investigations.
Footnotes
Acknowledgements
The authors thank Dr Argyro Kavadella, Oral and Maxillofacial Radiologist, for her generous help with the radiographic image capturing and analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the authors and the European University Cyprus and received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.