
Abstract
Multiple impacted supernumerary teeth are rare and need a multidisciplinary approach for optimal management to reduce potential complications. Herein, we present the case of an otherwise generally healthy woman in her early 30s who presented to the oral medicine clinic with a chief complaint of multiple missing teeth. Family history revealed that her sister and brother had the same complaint. Panoramic and cone-beam computed tomography radiographic findings revealed the presence of multiple impacted supernumerary teeth in both jaws. Multiple radiopacities and frontal sinus osteoma were noted. The radiographic features were suggestive of Gardner syndrome. An endoscopy was requested, which turned out negative for any polyps, with a recommendation to repeat endoscopy after 10 years. This is because the cranial osteoma might precede the gastrointestinal polyposis. A comprehensive treatment plan was performed by a team of dentists from multiple specialties (oral medicine, oral radiology, orthodontics, prosthodontics, and oral surgery) to ensure optimal outcomes for the patient. Thus, it is essential for dentists to identify and explore any atypical findings that may arise during clinical examination.
Introduction
Supernumerary teeth, also known as “hyperdontia,” refer to the presence of extra teeth that exceed the normal number of dentitions. They can appear anywhere in the dental arch and could be unilateral or bilateral. 1 Impaction, delayed eruption, ectopic eruption, overcrowding, spacing anomalies, and follicular cysts are specific complications associated with supernumerary teeth. 2 The prevalence of supernumerary teeth ranges from 0.5% to 5.3% and varies geographically. 3
The development of multiple impacted or supernumerary teeth is a rare condition and might present as an isolated condition; moreover, it can be associated with several different developmental disorders. Cleft lip and palate, cleidocranial dysostosis, Gardner syndrome, Fabry–Anderson syndrome, Ehlers–Danlos syndrome, and tricorhinophalangeal syndrome are all conditions involving multiple supernumerary teeth. 4 A systematic search was conducted across all peer-reviewed publications in English-language journals utilizing medical journal databases, starting from January 1965 until December 2024. Search terms pertinent to the topic included “Supernumerary,” “Familial,” “oral cancer,” “hyperdontia,” and “Non-syndromic,” which were combined with the Boolean operators AND and OR. Article titles and abstracts were screened for relevance, after which full-text screening was performed, and the most relevant articles were selected (Table 1). Only a few cases of nonsyndromic multiple impaction and supernumerary teeth have been reported in the literature.5–8 Familial occurrences are extremely rare. Only eight familial cases have been reported in the reviewed literature.9–16
Literature review of case reports.

Inchingolo et al. revealed that a family with a normal karyotype had multiple impacted supernumerary teeth among its siblings, highlighting the hereditary aspect of hyperdontia. This observation emphasizes the role of genetic predisposition in nonsyndromic hyperdontia, indicating that healthcare providers should take family history into account when diagnosing and managing this condition, even when no syndromic associations are present. The implications for dental practice are significant, as careful monitoring and potential interventions may be warranted for those with a familial history of hyperdontia. The reinforcement of these findings in subsequent studies further supports the idea that although supernumerary teeth can appear sporadically, familial cases suggest a significant genetic factor that should be recognized in clinical evaluations. 12 However, the link between supernumerary teeth and various genetic syndromes has been extensively documented. Subaşıoğlu et al. conducted a thorough review and indicated that supernumerary teeth can act as an early diagnostic indicator for conditions such as Gardner syndrome and cleidocranial dysostosis. Acknowledging these associations is vital for prompt intervention and management of affected patients. The ability of dental professionals to recognize supernumerary teeth as potential signs of underlying syndromic disorders can facilitate a comprehensive approach to patient care. 17 Lubinsky and Kantaputra further discussed specific Mendelian syndromes linked to supernumerary teeth, revealing that although some associations are well-documented, others may be coincidental. 4 This variability poses challenges in clinical diagnosis and underscores the necessity for differential evaluation between syndromic and nonsyndromic cases, ensuring that patients receive appropriate treatment.
Multiple impacted supernumerary teeth are rare and need a multidisciplinary approach for optimal management to reduce potential complications. In this report, we present the case of a 31-year-old woman with multiple impacted supernumerary teeth in both jaws.
Clinical report
We present the case of an otherwise generally healthy woman in her early 30s who presented to the oral medicine clinic with a chief complaint of multiple missing teeth. The patient reported that she was a healthy child. During clinical examination, no signs of mental retardation, facial abnormalities, or skeletal abnormalities that indicate a systemic syndrome were observed. The patient mentioned that she has had multiple visits to the dental office where she extracted her deciduous teeth due to caries or mobility, which caused her emotional trauma as she did not replace any of the missing/extracted teeth.
Her family history revealed that her sister and brother had the same complaint. Intraoral examination revealed poor oral hygiene; teeth #33, 81, 82, 83, and 84 in the lower jaw and teeth #51, 61, 17, 14, 23, and 24 in the upper jaw were fully erupted (Figures 1 and 2).

Intraoral photograph showing erupted teeth in the maxilla.

Intraoral photograph showing erupted teeth in the mandible.
A panoramic image showed multiple supernumerary teeth in the maxillary premolar area as well as impacted and malapportioned teeth with abnormal tooth morphology and dilacerations in the maxilla and mandible (Figure 3). Other findings included multiple missing teeth, carious teeth with periapical lesions, idiopathic osteosclerosis, and over eruption and tilting of tooth #17; the edentulous areas of the posterior mandible appeared to bulge out due to possible overgrowth of the crest of the ridge.

Panoramic images showing multiple impacted supernumerary teeth.
CBCT images showed the presence of multiple impacted supernumerary teeth with abnormal tooth morphology size and position as well as severe root dilacerations.
In addition, an osteoma was noted within the left frontal sinus (Figure 4). Other maxillofacial features included a protruded mandible and a retruded smaller maxilla. Furthermore, multiple areas of polyp formation were seen in the walls of the oropharynx. Other dental findings included multiple missing teeth and carious teeth with periapical lesions (Figure 5).

Cone-beam computed tomography (CBCT) images. Coronal, sagittal, and axial sections showing osteoma within the left frontal sinus.

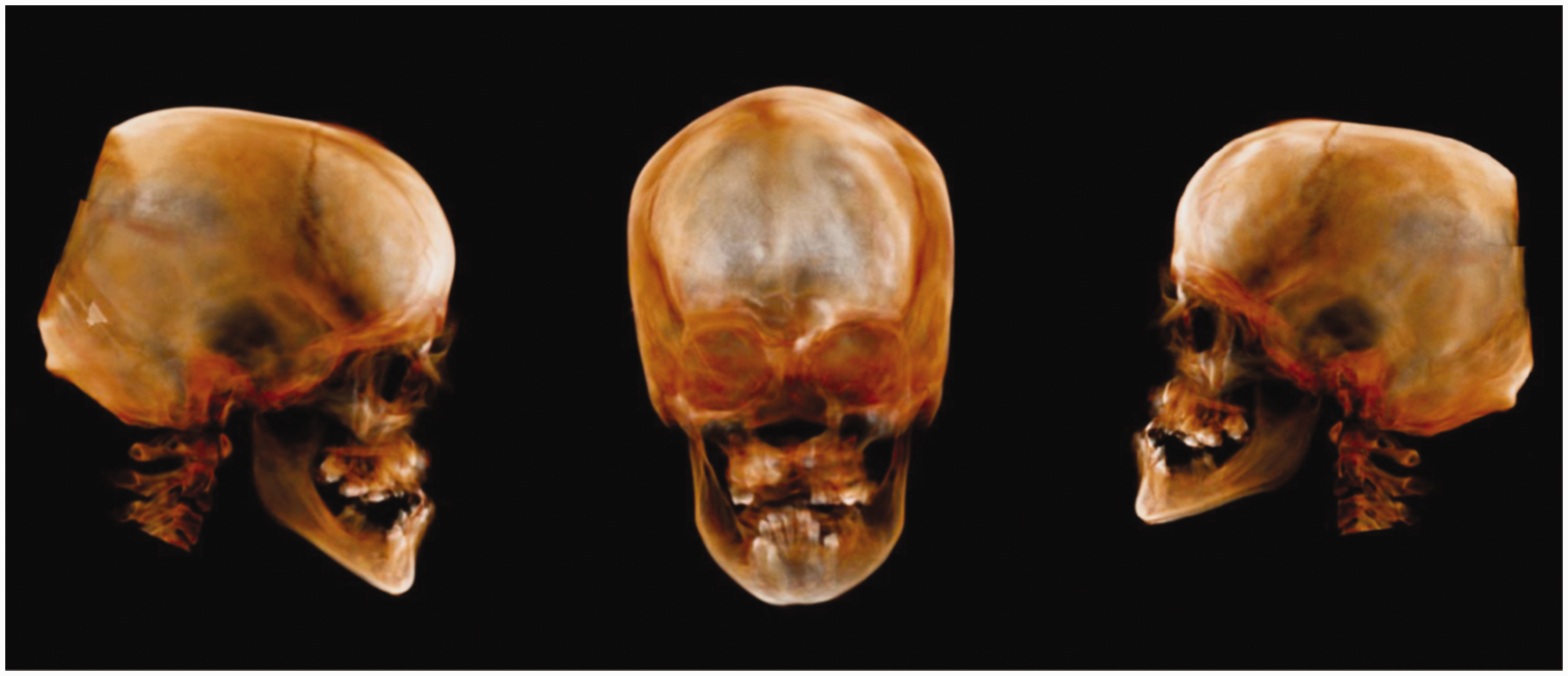
Cone-beam computed tomography (CBCT) images. (a) Deformed, dilacerated, and malopositioned impacted supernumerary teeth; (b,c) Sagittal section showing polypoid formation on the wall of the oropharynx and (d) surface rendered image showing multiple supernumerary teeth in both jaws.
The patient’s sister is 30 years old and has type II diabetes. Examination of her sister revealed that she has two supernumerary upper left and over-retained deciduous teeth with many impactions. The upper right second premolar was congenitally missing and there was impaction in the lower jaw (Figures 6 and 7), but she had dentophobia and refused to continue dental therapy. Her brother could not be examined, as he did not show up because of work commitments. Cone-beam computed tomography (CBCT) was proposed by the radiologist as a means to identify any anomalies or abnormalities, including osteomas. Examination showed multiple carious teeth and missing and remaining roots. In addition, several impacted teeth (#14, 13, 11, 21, 24, and 43) and partially impacted teeth (#17, 27, 34, and 44) as well as retained deciduous (#55, 54, 53, 54, 55, 74, and 83) were noted. There was malposition of tooth #12, which was horizontally impacted. All second premolars were congenitally missing with retained primary teeth #15 and 25. Dilaceration and abnormal tooth morphology were observed in multiple teeth. Moderate-to-severe horizontal bone loss was noted. Other findings included a hypoplastic maxilla with a protruded mandible and a hypoplastic maxillary sinus that was smaller on the right side. Sella turcica appeared to be slightly increased in size (ballooning). Another incidental finding was the deviation of the nasal septum. Nevertheless, due to severe motion (dental phobia), there were some artifacts reducing the quality of the images.

Panoramic images of the patient’s sister showing multiple missing, retained deciduous, and impacted teeth.
Three-dimensional cone-beam computed tomography (CBCT) images showing hypoplastic maxilla and protruded mandible.
The radiographic features were suggestive of Gardner syndrome. A consultation with a gastroenterologist was conducted and an endoscopy was requested. Endoscopy was negative for any polyps, with a recommendation to repeat endoscopy after 10 years, as the cranial osteoma might precede the gastrointestinal polyposis.6,7 Based on the familial history of multiple impacted teeth, the patient was sent for genetic counseling and risk assessment for further investigation.
Moreover, a list of certified psychotherapists was provided to the patient to address her concerns and fear of losing all her teeth. Finally, a thorough treatment strategy was implemented by a multidisciplinary team of dentists, including specialists in oral medicine, oral radiology, orthodontics, prosthodontics, and oral surgery, to guarantee the best possible results for the patient. Consent was obtained from the patient for the publication of the case report, including clinical images.
Discussion
The precise etiology of the development of supernumerary teeth is not well understood, and many different hypotheses have been proposed to explain this phenomenon. The atavism (evolutionary throwback theory) was also proposed to explain the development of supernumerary teeth. It is postulated that the presence of supernumerary teeth represents a reversion to primitive or extinct anthropoid tissues as the evolution had caused a reduction in teeth numbers. 18 Furthermore, the overactive dental lamina theory states that the over-proliferation or failed apoptosis of the dental lamina epithelial cells may cause supernumerary tooth formation. 19
The classification of dental anomalies, including supernumerary teeth, is essential for understanding their relationship with genetic disorders. Dure-Molla et al. introduced a systematic approach that can aid clinicians in diagnosing associated syndromic conditions. 20 This structured classification system is instrumental in bridging the gap between dental anomalies and genetic syndromes, promoting a thorough understanding of the complexities involved in managing supernumerary teeth.
Molecular mechanisms underlying the formation of supernumerary teeth have been explored by Lu et al., who discussed the role of specific signaling pathways. Their findings indicate that although some cases of hyperdontia are sporadic, others correlate with genetic syndromes. 21
Several genetic animal studies have shown that mutations in Fgf, Eda, Bmp, Runx2, Apc, Shh, and β-catenin genes are associated with the development of supernumerary teeth in mice. 22 Supernumerary teeth represent one of the most characteristic dental findings in Gardner syndrome. These additional teeth can be discovered during routine dental examinations and may serve as early diagnostic indicators of the syndrome. 23 The dental manifestations of Gardner syndrome often precede the development of intestinal polyposis, making them valuable early diagnostic markers. Studies have shown that dental professionals may be the first to identify signs of the syndrome during routine examinations. 24
In Gardner syndrome, polyps predominantly occur in the colon and rectum, although they may also be found in the stomach and small intestine. The histological characteristics of these polyps differ by their location; for instance, polyps in the gastric fundus and body are generally non-neoplastic, whereas those in the duodenum and terminal ileum are frequently adenomatous. Although these polyps start as benign, they carry a significant risk of malignant transformation if not appropriately managed. The clinical implications of these polyps remain unclear; however, due to the elevated risk of duodenal cancer associated with Gardner syndrome, it is advisable to conduct periodic evaluations of the upper gastrointestinal tract. Management strategies for these patients usually include regular surveillance via colonoscopy and, in certain cases, prophylactic colectomy. Timely diagnosis and intervention can lead to improved prognoses and better patient outcomes.25,26
Symptoms such as diarrhea, constipation, rectal bleeding, anemia, and abdominal pain may be present at the time of diagnosis. Individuals with Gardner syndrome have a high risk of developing colorectal cancer at an early age. The prevalence of cancer in patients with symptomatic familial adenomatous polyposis ranges from 47% to 67%, and 59% of patients diagnosed with Gardner syndrome die from colorectal cancer due to extensive metastasis. Almost 100% of colorectal polyps will undergo malignant transformation if left untreated.23,25–27
Familial clustering of the reported cases of supernumerary teeth suggests that heredity plays a crucial role in the development of this condition. In addition, a study on identical twins reported that twins tend to have supernumerary teeth in the same location as their parents, which explains a genetic involvement. 28 A heterozygous chromosome 8q24.13 mutation in FER1L6 was identified in a Chinese family with nonsyndromic familial multiple supernumeraries. 29 Multifactorial determinants have been suggested in the literature with an autosomal dominant inheritance pattern.10,12,16
The most commonly reported site of familial supernumerary teeth is the premolar area,10,11,13–15 followed by molars and incisors.10,12,16 In contrast to nonfamilial cases, familial cases occur more frequently in males than in females (9:12).30,31 Furthermore, the mandible is more affected than the maxilla (59:43), and the premolar area is more affected than the premaxilla.30,31
Although the isolated presence of multiple supernumerary teeth is considered extremely rare, multiple supernumerary teeth are a common manifestation of systemic syndromes and metabolic disorders. Cleidocranial dysostosis, Gardner syndrome, Fabry–Anderson syndrome, Ehlers–Danlos syndrome, and tricorhinophalangeal syndrome are all characterized by the presence of multiple supernumerary teeth. 4
Gardner syndrome is a dominant inherited genetic disorder caused by a mutation in the adenomatous polyposis coli (APC) gene on chromosome 5q21. 32 APC is a tumor suppressor gene that controls cell growth. Mutation in APC leads to uncontrolled cell growth. Gardner syndrome is characterized by the formation of multiple colonic polyps. Several dental manifestations are associated with Gardner syndrome, including hypercementosis, odontomas, impacted permanent teeth, retained deciduous teeth, and supernumerary teeth. Maxillofacial diagnostic manifestations of Gardner syndrome include the development of osteomas. 32 Osteomas can develop anywhere in the bones of the face and head, although they are most commonly located in the skull, mandible, facial bones, and paranasal sinuses. 33 Maxillofacial manifestations occasionally precede the formation of colonic polyps by many years and thus might be used as a diagnostic marker for Gardner syndrome. 34 In our case, the maxillofacial manifestation of the patient was highly suggestive of Gardner syndrome, although endoscopy revealed no colonic polyps. Genetic testing will provide a definite diagnosis and will guide treatment decisions. Further consultations and referrals to other dentists with different specialties were initiated to ensure the best treatment outcomes.
This report emphasizes the significance of effective collaboration among various medical and dental specialties to achieve accurate diagnoses in complex cases and guarantee the quality of healthcare delivered to patients. It is advisable to conduct long-term follow-ups, as multiple issues may arise, including follicle enlargement and tooth resorption.35,36
Conclusion
This report highlights the importance of a multidisciplinary approach when managing patients with multiple impacted supernumerary teeth to reduce potential complications and ensure the best outcomes. The dentist should be alert to detect and investigate unusual findings during a routine clinical examination. Understanding manifestations is crucial for early diagnosis and appropriate management. Dental professionals play a vital role in the identification and monitoring of these patients, highlighting the importance of thorough dental examinations in suspected cases.
Footnotes
Author contributions
All authors contributed equally.
Disclosure
The authors report no conflicts of interest related to this work.
Data availability statement
The study data will be available on request.
Ethical approval
The need for ethical review and approval was waived for this study. This is because our institution does not provide an institutional review board (IRB) approval for case reports, considering that they involve the retrospective analysis of a single patient’s medical history and do not require the same level of ethical oversight as other research methodologies.
Funding
This study received no funding.