
Abstract
This case presents a diagnostic challenge in a 28-year-old male initially evaluated for severe abdominal pain, vomiting, and constipation, leading to the presumption of post-appendectomy complications. Clinical examination revealed abdominal distension, tenderness, and signs of peritonism, along with a reducible inguinal hernia. On subsequent CT scan, a large, inflamed area of omentum localized to the right abdomen extending up to the defect in the inguinal region with mild ascites was revealed. Upon exploration, it was discovered that the patient’s initial surgery had focused solely on an appendix deemed mildly inflamed by the operating surgeon, while a concurrent diagnosis of secondary omental torsion was missed. This oversight underscores the challenges in diagnosing abdominal pathologies, with the initial misdiagnosis leading to ongoing patient distress. Meticulous adhesiolysis and omentectomy were performed, resulting in the resolution of the patient’s symptoms.
Introduction
Omental torsion, a rare abdominal pathology accounting for only 1.1% 1 cases of abdominal pain worldwide, poses diagnostic challenges due to its non-specific symptoms. Omental torsion refers to the rotation of a segment of the omentum along its axis, leading to compromised blood supply, ischemia, necrosis, production of serosanguineous fluid, and peritonitis. 2 It can be primary or secondary depending on the etiology. Primary omental torsion, also known as unipolar, is associated with factors like anatomical variations in the omentum encouraging rotation and risk factors like obesity resulting in abnormal fat distribution. 3 Secondary omental torsion, or bipolar, is related to intra-abdominal pathologies like adhesions, inflammation, cysts, tumors, hernias, etc., where the distal end of the omentum gets attached. 4
So far only 300 cases 5 of omental torsion have been reported in the existing literature with an incidence of 0.0016% to 3.7%. 5 Here, we present a case of omental torsion secondary to right inguinal hernia that was misdiagnosed previously as acute appendicitis.
Case presentation
Twenty-eight years old male with no prior comorbidities, presented in our Emergency Department with severe abdominal pain, distention, relative constipation and vomiting for 3 days. He has had an open appendectomy done via McBurney’s approach at some other hospital with limited medical facilities 5 days prior. His medical history included a previously untreated right inguinal hernia and non-specific intermittent abdominal pain localized to right lower abdomen for 3 months. On physical examination, he was tachycardiac with pulse of 121 bpm, blood pressure 110/70 mmHg, respiratory rate 20 bpm, and a temperature of 100°F. Abdomen was distended, tender in all four quadrants, guarding right abdomen with decreased peristalsis and a right sided, complete, reducible inguinal hernia. Digital rectal examination showed an empty collapsed rectum. Laboratory studies indicated a leukocyte count of 6.2 × 103/μL, neutrophils of 75%, total bilirubin of 4.0 mg/dl, unconjugated bilirubin of 2.9 mg/dl, and conjugated bilirubin of 1.1 mg/dl. The rest of the blood and serum biochemistry parameters were within normal limits. A contrast-enhanced CT scan was performed, revealing an inhomogeneous, irregular fat density mass measuring 20 × 18 × 25 cm localized to the right side of the abdomen (Figure 1). The mass extended up to the defect in the right inguinal region, accompanied by the presence of whirl sign suggestive of torsion of the greater omentum, with mild ascites (Figures 2 and 3). Midline laparotomy was done and surgical exploration unveiled an inflammatory mass involving the right abdomen, adherent to the right colon and cecum, with its distal end attached to the right inguinal sac, along with mild bloody ascites. The inflammatory mass was dissected, revealing omental torsion with one and a half circle twists. The infarcted omentum was resected (Figure 4) and repair of right inguinal hernia was performed. Our patient had an uneventful recovery and was discharged two days after surgery. Outpatient follow-up was performed for one month, showing adequate evolution and no late complications.

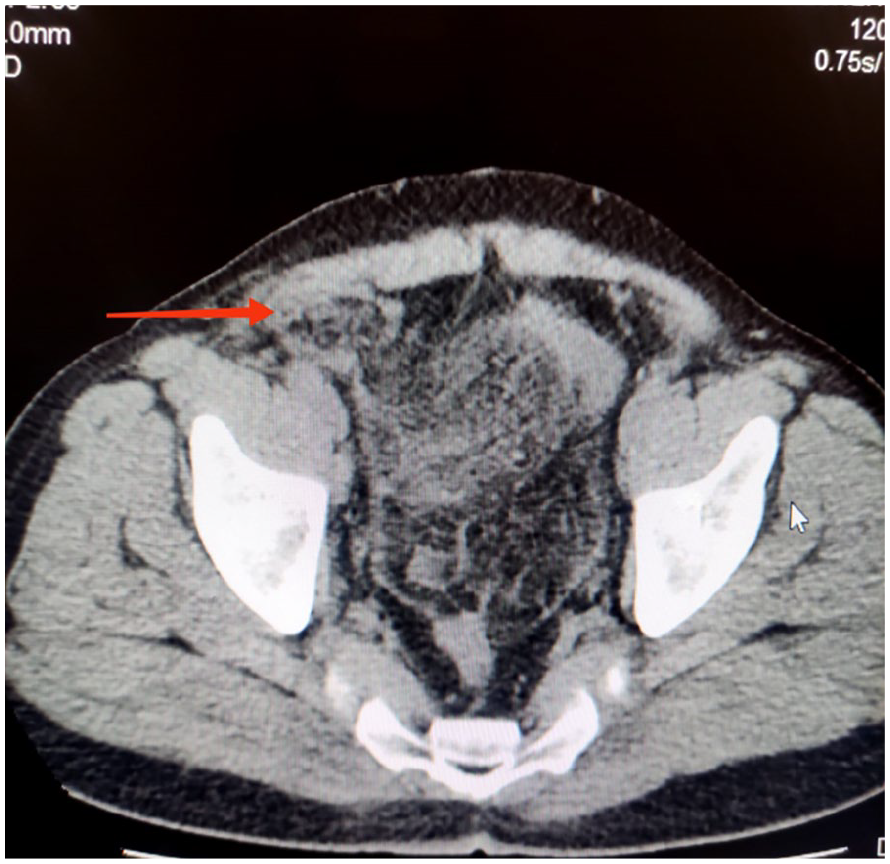
Computed tomography scan-axial view demonstrating characteristic omental whirl suggestive of omental torsion. Red arrow head (whirl sign).
Computed tomography scan-axial view demonstrating fat density mass extending up to the defect in right inguinal canal (red arrow head).

Computed tomography scan-coronal view demonstrating a large well-circumscribed heterogeneous fatty mass in the right side of abdomen (yellow arrowhead) with an associated right inguinal hernia containing omental fat only (red arrowhead).

Intraoperative picture demonstrating gangrenous greater omentum after untwisting.
Discussion
Omental torsion, although a rare abdominal pathology, poses a significant challenge for diagnosis and has been often mistaken for more prevalent conditions like acute appendicitis. Ghosh et al. 6 reported acute appendicitis to be the most common mistaken diagnosis in nearly all patients of omental torsion. It tends to predominantly affect middle aged males, with male to female ration of 5:1. 5 The greater omentum is frequently affected due to its length and greater mobility, 7 although cases involving lesser omentum have also been documented. 8 The primary clinical manifestation, noted in approximately 90% of cases, 9 is right-sided abdominal pain, which can be misleading, similar to the symptoms of acute appendicitis, as presented in our patient.
The classification of omental torsion revolves around its etiology, distinguishing between primary and secondary types. 10 Secondary omental torsion, first documented by Oberst 11 long before the discovery of primary omental torsion by Eitel, 12 is associated most commonly with cases secondary to inguinal hernia. 13 Corner and Pinches conducted comprehensive review of 54 cases, finding inguinal hernia as a cause of secondary omental torsion in 90% of patients. These hernias exhibited distinctive features, such as their location in the right inguinal region, a scrotal type, prolonged duration, easy reducibility and almost always containing omentum, 13 consistent with our research findings.
The misdiagnosis of secondary omental torsion, as acute appendicitis in this case along with the presence of an untreated inguinal hernia, prompts a critical examination of the challenges associated with diagnosing uncommon abdominal pathologies. Omental torsion, though rare, can mimic more common conditions, 14 leading to pitfalls. The initial presentation of abdominal pain localized to the right iliac fossa along with the clinical findings similar to that of acute appendicitis misled the diagnostic focus toward the appendix, contributing to the delayed recognition of omental torsion. The importance of a thorough clinical history and examination cannot be overstated, as this patient had intermittent abdominal pain for 3 months along with a longstanding reducible right-sided inguinal hernia giving insight that whenever a patient presents with right iliac fossa pain along with inguinal hernia, the possibility of omental torsion should be considered.
Our case presents distinctive features in contrast to the established literature on omental torsion. Notably, a normal leukocyte counts of 6.2 × 103/μL deviates from the commonly elevated leukocyte count 15 in other studies. Concurrently, an elevated total bilirubin level of 4 mg/dl aligns with the findings from Katagri et al. 16 who reported a total bilirubin of 2.9 mg/dl. Additionally, Nishiwaki, et al. proposed that involvement of long segment of omentum in torsion and infarction may contribute to hemolysis, impacting the total bilirubin level. 17 This suggests the potential use of total bilirubin as a diagnostic marker for omental torsion in future research.
The widespread use of CT scans for abdominal pain has indeed improved the detection of omental torsion due to its ability to provide detailed imaging, aiding in more frequent and accurate diagnosis. 18 In our patient, CT scan was pivotal in unraveling the true nature of the pathology, revealing a large fat density mass extending up to the defect in the inguinal region accompanied by the presence of whirl sign suggestive of torsion of the greater omentum, with mild ascites (Figures 1–3). This emphasizes the significance of advanced imaging techniques in diagnosing rare abdominal pathologies.
The significance of diagnostic laparoscopy in patients with non-specific abdominal pain cannot be overstated. 19 It offers a definitive means of diagnosis by directly visualizing the abdominal cavity. By enabling precise identification and management of conditions that may otherwise be overlooked, laparoscopy plays a crucial role in averting unnecessary treatment delays and minimizing the risk of complications.20,21 The current management of choice for omental torsion is laparoscopic, proceeding to laparotomy if required and includes identifying and removing the infarcted segment of omentum. Finding of free serosanguineous fluid as a result of hemorrhagic extravasation is a characteristic finding which was also present in our study. 22
Surgical intervention not only resolved the patient’s symptoms but also underscores the importance of adaptability during surgery when unexpected pathologies are encountered.
Reviewing existing literature reveals that omental torsion is often misdiagnosed due to its rarity and non-specific symptoms. Comparisons with similar cases stress the need for a high index of suspicion, especially in patients with abdominal pain with inguinal hernia.
Conclusion
In summary, this case highlights the significance of adopting a thorough diagnostic approach aiming to avert misdiagnoses such as omental torsion. Enhanced awareness, meticulous clinical examination, and the application of advanced imaging techniques play pivotal roles in ensuring precise and timely diagnoses, thereby enhancing overall patient outcomes. Prior to surgical exploration, a CT scan should be consistently considered for accurate diagnosis in such patients. Whenever possible, laparoscopic surgery is recommended, especially in situations where the clinical presentation is atypical.
Footnotes
Acknowledgements
The authors are very appreciative to the patient for the opportunity to learn as well as thankful to the hospital for providing support for completing this report.
Author contribution
N.M. has given substantial contributions to the conception and design of the manuscript. K.S. and N.S. revised the manuscript critically for important intellectual content. S.A.A. supervised the project and final proof reading of the manuscript to be published. All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized informationto be published in this article.